Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Review Article - (2018) Volume 6, Issue 1
Keywords: Anti-microbial; Nosocomial; Probiotics; Pathogenic; Multi-resistance
Naturally, microorganisms are always present in foods of plant or animal source and during exposure from the field to the consumer’s table. This truth stands because they are everywhere in the air, soil, water, the animals, plants and on the handlers [1-3]. Their presence could spoil the food, making the producer/processor incur economic losses. They could cause food borne illnesses thereby exposing the consumer to health problems. Some microorganisms, however, could still be of direct benefit since they could transform a food’s properties in a beneficial way such as in fermentation [1].
Of major interest in this review are the pathogens, which include all those microorganisms that are capable of endangering the health of the consumers either through infection or ingestion of microbial toxins. They include: Clostridium spp., Staphylococcus spp., Bacillus spp., Campylobacter spp., Listeria spp., Escherichia coli , etc. [1,3].
These interestingly are highly responsive to antibiotic treatments, and that has been the popular treatment given to victims of food borne illnesses. However, over-exposure to antibiotics could lead to resistance by the microorganisms thereby making the treatment ineffective. This has been increasingly the experience in the UK, and the US. Probiotics could reverse multi-drug resistance. This recent development has elicited diverse research [4-9]. This review attempts to consider the effectiveness of probiotics in combatting Clostridium difficile , an opportunistic microorganism.
Foodborne Illnesses
These are illnesses contracted through food. They could be biological, chemical or physical [2,10-13]. Table 1 gives a view of some of the possible causes of the various categories identified.
This review focuses on the biological hazards and anchors on foodborne pathogens.
An Overview of Foodborne Pathogens
Foodborne pathogens are those microorganisms that are capable of causing diseases to consumer [3]. They include Clostridium botulinum , Staphylococcus aureus , Bacillus cereus , Vibrio species , Yersinia enterocolitica, Clostridium perfringens, Salmonella , Shigella , Escherichia coli, Campylobacter , Mycobacterium and Listeria monocytogenes. Other non-bacterial pathogens include mycotoxins, protozoa, helminths, Taenia, Trichinella, Toxoplasma, Scrapie, bovine spongiform encephalopathy, kuru and Creutzfeldt-Jacob disease [2,3].
Foodborne pathogens, when ingested either as a pre-formed toxin or live cell of the microbe has the capacity of causing disease conditions that could lead to vomiting, nausea, diarrhoea, dysentery, fever, cholera, abdominal pains, chills, cramps, sore throat, scarlet fever, etc.[2].
How Do Foods Become Contaminated?
Foods, while in the field could get contaminated with faecal materials. Every pre-processing contamination should be handled by processing operations [14]. However, finished products could be risk factors. Figure 1 describes the channels through which they could be contracted from. This could result from post-processing handling during packaging, heat resistant spores that survived the processing conditions or during storage. A good assessment of foodborne diseases in finished products had always been traced to poor quality control regime, faulty equipment and or poor personnel hygiene [2].
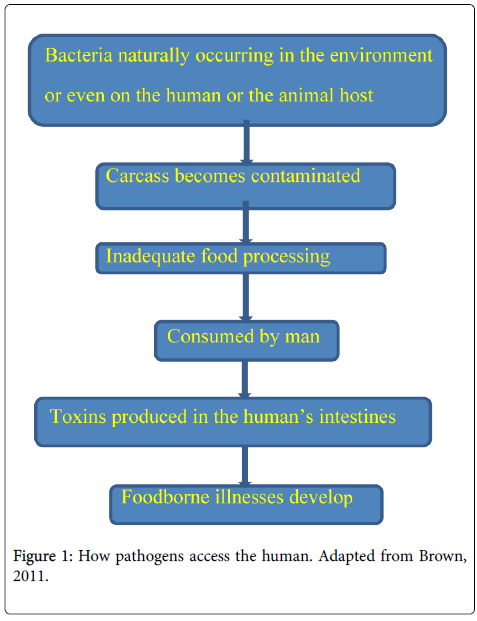
Figure 1: How pathogens access the human. Adapted from Brown, 2011.
Antibiotics are medical formulations made either from safe microbial cells or plant materials which can either kill (bactericidal) or inhibit (bacteriostatic) the growth of microorganisms that are inimical to human or animal’s health [15,16]. Alexander Fleming was the first to formulate an antibiotic (penicillin) in 1928 and that landmark achievement has birthed diverse types of antibiotics that could be described as broad (used on a wide range of pathogens) or specified (specific in their target). Chemically synthesised antibiotics are now available to complement those from natural sources [17].
How antibiotics work
Antibiotics are poisonous to pathogens. When administered, it would locate the pathogen, and either destroys the cell wall, thereby killing it or may disrupt its biochemical process (by not allowing them convert glucose to energy) thereby not allowing it to keep replicating.
The antibodies in the body will then over power them and stop them from replicating [18].
The abuse of antibiotics
Antibiotics are good and have helped in preserving lives in the treatment of infections. They find wide usage during surgical operations. They could be administered orally or through injectable. However, they are often a last resort, in most cases [19].
Abuse of antimicrobials is a common place in the recent past. Antibiotic abuse occurs when taken without prescription, when prescribed instead of using available alternatives, or when taken below or more than the prescribed dosage [20,21].
Pathogens develop resistance to antibiotics when abused. The condition of the patience worsens at this point leading to depletion of antibodies in the human body. This is the case in so many hospitals [15,22-24]. At present, European Centre for Disease Prevention and Control estimates that health conditions resulting from antibiotic resistance in Europe costs €1.5bn (£1.2bn), every year [24]. Arias and Murray [25] wondered the fate of medical practice in the 21st century without antibiotics. The quickest action must be adopted [26].
Leeb [27] described the development of antibiotic failure as ‘‘A shot in the arm’’ and lamented that ‘‘the pipeline of antibiotic research and development are nearly dry’’. Norrby, et al. [28] emphasised the need for further research and regulatory enabling environment to formulate antibiotics that will salvage the situation [29].
How is resistance acquired by pathogens?
Charles Darwin in 1859 proposed a mechanism of evolution called natural selection in his book, the ‘Origin of species’. He positioned that species survived by their reactions to different environmental factors. Further, he observed that those that survived may have had some traits that others never had and that the surviving species would need another form of environmental manipulations if they must be gotten rid of from their host [30].
Foodborne pathogens, on sensing the presence of antibiotic reacts differently to them. Some will die; some inactivated while some of them will remain undisturbed. Those that survived will begin to feed on the antibiotic and hence resistance results [31].
Plant and animals food products that have resistant species can still transfer such trait to man as well as uncontrolled use of antibiotics [2,32].
Mechanisms of antimicrobial resistance
The mechanisms of acquiring resistance are predominantly biochemical. Figure 2 shows how bacterial cells make nonsense of antibiotics through mutation, destruction or inactivation and efflux thereby acquiring resistance traits.
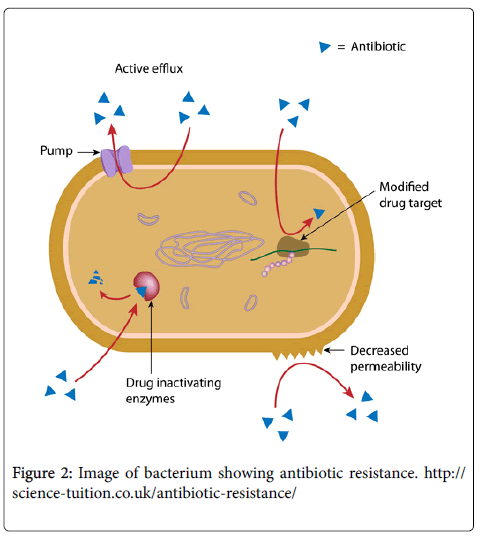
Figure 2: Image of bacterium showing antibiotic resistance. http:// science-tuition.co.uk/antibiotic-resistance/
Mutation-involves a change in the DNA of the microbe and this could result in change in the gene, which is the target of the antimicrobial device. What anti-microbes do is that they will stop the replication of the DNA by inhibiting the secretion of DNA gyrases, which the microbe, needs for replication, and this often, will lead to the death of the cell. When a spontaneous mutation occurs on some areas that encode the gene that produces the enzyme, the microbe continues to replicate its DNA [15,25].
Destruction or inactivation-some bacteria have the capacity of producing an enzyme that can neutralise an antibiotic or prevent it from reaching their target component of the cell that would elicit destruction. By so doing, the antibiotic becomes ineffective [33,34].
Efflux-antibiotics enter the bacterial cell through an opening on the cell wall called porin. The bacterial cell has a pump called efflux pump, which evacuates, the antimicrobials and other compounds out of the cell thereby not allowing an accumulation that would result to the minimum inhibitory concentration (MIC) of the device hence making it ineffective [34,35].
Besides, genetic transfer could as well promote resistance. This is true because some genetic materials could be transferred from a resistant cell to another through plasmids migration. Conjugation, transformation, or transduction is the means of achieving them [36].
Control of antibiotic resistance
Prevention is better than cure. This would play very successfully in the fight against antibiotic resistance. An aggressive approach to public health would prevent infection through adequate food processing and preparation regimes. Proper sanitary strategies and general healthy living will help in controlling the insurgency of these foodborne illnesses and by extension the use of antibiotics [32,37].
Regulation on the prescription and use of antibiotics should be complied with, strictly [38].
Investigating into the pathogens and working out molecular biological strategies to obstruct their resistant traits would be helpful [26]
Identification of new antibiotic, which could be formulated using natural sources, as well as expanding research on the synthesis of new chemical antibiotics, could be helpful. This could be achieved using combinatorial chemistry and structural biology [39,40].
Closridium difficile is an opportunistic gram positive, sporulation bacillus . The name derives from a Greek and a Latin word ‘kloster’ (Greek word for spindle) and ‘difficile’ (Latin word for difficult/ obstinate). The name, therefore, pictures its behaviour. It accounts for the majority of the diarrhoea cases in antibiotic treated patients, the immune-compromised and children and has resulted to about 20, 642 deaths in US between 1999-2004 [4,41,42]. When the antibodies (good bacteria) are destroyed by the use of antibiotics, Clostridium difficile will attack. The medical personnel and environmental issues are responsible for their proliferations [41,43]. They are spore formers and can survive adverse conditions of pH, heat and even antibiotics. Figure 2 shows the route of transmission through a hospital setting [41].
Control of Clostridium difficile-associated diseases (CDAD)
Hand washing, use of gloves, restriction of the use of antibiotics and regular surface cleaning of the environment are helpful [41,44].
Many know probiotics as a ‘new’ health miracle. They help in treating or at least mitigating health conditions such as constipation, diarrhoea and prevent cold or fight against them when they developed [44].
The word, probiotic is from two Greek words pro and biotic meaning ‘promoting’ and ‘life’, respectively. Food and Agricultural Organisation (FAO) of the World Health Organisation (WHO) defines probiotics as ‘‘live microorganisms, which, when administered in adequate amounts, confer a health benefit on the host’’ [45].
Why use probiotics?
It could be worrisome to think of using bacteria or any other microorganism to fight other bacteria or microorganism. This is akin to creating problems in the bid to solving an already existing one. It is needful to point out that, in the human body, we have what could be described as the ‘good’ and the ‘bad’ bacteria [4,5,8] and the body keep going despite this pressure by striking a balance. The abuse of antibiotics, improper nutrition, emotional stress, insomnia and environmental influences distort the balance [4]. Probiotics restores the balance in the digestive tract and impact on the immune system [46].
How is probiotics novel?
It is interesting to observe that probiotics has always been there even from birth. The new born contracts some bacteria as it passes the birth canal of the mother, this is not possible through caesarean section. This position underscores the reason why children delivered through caesarean section are more likely to be allergic than those of normal delivery. Besides, those delivered through the birth canal have their immune systems at optimal; this is not the case with caesarean section [47].
Types of probiotics
Some of the microflora of the gut includes Clostridia , Lactobacilli , Enterococci and Escherichia coli [8].
Previous studies show that several species of the Lactobacillus , Lactobacillus acidophilus , Lactobacillus bulgaricus , Lactobacillus casei , Lactobacillus gasseri, Lactobacillus johnsonii, and Lactobacillus plantarium are beneficial to man. They help in prevention and/or treatment of several disease conditions including lactose intolerance, urinary tract infection, irritable bowel syndrome, anti-biotic related diarrhoea, diarrhoea other Clostridium difficile , associated diseases (CDAD) [44,48].
It reported that Bifidobacteria bifidium , B. longum , B. breve , B. infantis , B. thermophilum , and B. pseudolongum help in dental cavities, improved blood lipids and glucose intolerance.
Saccharomyces boulardii, a yeast probiotic, is efficient in the treatment of antibiotic use associated diarrhoea and traveller’s diarrhoea. Report has it that Saccharomyces boulardii prevents the reoccurrence of Clostridium difficille [49].
Streptococcus thermophilus helps the prevention of lactose intolerance. Enterococcus faecium found in the tracts of humans and animals help in the balancing off of the bad bacteria. Leuconostoc has found several uses in the food processing industries [44].
Sources of probiotics
‘Beneficial cultures’ are products advertised as off the shelf in the UK and the USA. These are good sources of probiotics. Others include yoghurt, juice, cereal, candy bars and cookies. A combination of more than one of this is more effective in the treatment of Clostridium dificille [49].
Probiotics: Any side effects?
In the USA, food supplements are not strictly regulated like food and drugs. The FDA can only step in if there is any reported case. Dietary Supplements, Health and Education Act of 1994 (DSHEA) ‘‘demands manufacturers of dietary supplement or dietary ingredient to ensure the safety of their products before marketing’’ However, Consumerlab.com (CL) provides independent test results. Products that passed their tests get a seal of approval. Consumers make their choices relying upon the seal [50].
Management and administration of probiotics
Only living bacteria or yeast cells beneficial to man could be used as a probiotic. It is, therefore, necessary to comply with prescribed storage conditions. If the cells are dead, they will not deliver the benefits [6,49].
Consistency in the use of the identified strain is paramount in its efficacy. This true with microorganisms since different strains of the same genus and specie may not behave alike [9].
Several probiotics are off the shelf. Consumers should be able to know which of them is needful for their health conditions to avoid abuse, which may result into another problem. Medical doctors would be helpful at this point to advice patients on the type and amount of probiotic that would be helpful in their case [44].
How probiotics attack Clostridium difficile
Saccharomyces boulardii could interrupt the pathogenicity of Clostridium difficile either by neutralising the toxin or inhibiting the inflammatory response. Besides, the extracellular activities of bifidobacteria reduce the adhesion of the enterocyte-like cells of the pathogens [9].
The popularisation of the use of probiotics could remedy the defeat over foodborne pathogens, which antibiotics have lost in the recent times.
It is needful that more research efforts be invested in the activities of probiotics and its production. The probiotics so far discovered has not in any way adversely affected the health of the users. Some of these naturally occurring non-pathogenic microbes could still be genetically manipulated to enhance their efficiency in the treatment of health disorders such as Clostridium difficile -associated diseases.