Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2013) Volume 3, Issue 2
Background: Clinical researchers are major actors in translating evidence-based medicine into the care of patients. Acute Coronary Syndrome (ACS) is a good example for the implementation of complex intervention in the current context of growing economic pressure. According to the 2012 European Society of Cardiology guidelines, early discharge (approximately 72 hours of hospitalization) is reasonable in selected low-risk patients hospitalized with STEMI (ST-elevation myocardial infarction), if early rehabilitation is arranged. However, early discharge is not widely applied in clinical practice, and the potential barriers to shorten LOS have not been studied for patients hospitalized with an ACS.
Method: We will prospectively enroll 200 patients hospitalized with an ACS at the Geneva University Hospital using a before (100 patients, 2012-2013) and after (100 patients, 2013-2014) prospective cohort design. We will implement a systematic intervention consisting of four steps: (1) identification of low-risk patients treated successfully with percutaneous intervention using the Zwolle index Score; (2) targeting promptly an early discharge date within 72 hours after admission; (3) definition of a standard process of care during the hospital stay and (4) referral to a cardiac rehabilitation program within 10 days.
As primary outcome, we will assess the evolution of LOS using administrative data.
As secondary outcomes, we will analyze the potential barriers to an early discharge, the indicators of quality of care and the cost benefits comparing both periods before and after the implementation of an early discharge strategy. We will also assess the safety with a phone call at 30-day.
Summary: In the area of increase concerns on the long-term sustainability of the current health system,
translational science focusing on clinical effectiveness is more than needed. The systematic application of evidencebased recommendation is a way to improve the efficiency of process of care, as well as the transition from inpatient to outpatient setting.
Keywords: Coronary heart disease, Acute coronary syndrome, Clinical outcome research, Clinical effectiveness research, Translational research, Health economic
ACS: Acute Coronary Syndrome; CR: Cardiac Rehabilitation; DRG: Diagnosis-Related Group; ESC: European Society Cardiology; LOS: Length of Stay; MACE: Major Adverse Cardiovascular Event; NSTE-ACS: Non ST-Segment Elevation Acute Coronary Syndromes; NSTEMI: Non ST-Segment Elevation Myocardial Infarction; PCI: Percutaneous Coronary Intervention; RCT: Randomized Controlled Trial; STEMI: ST-Segment Elevation Myocardial Infarction; TIMI: Thrombolysis In Myocardial Infarction
Health professional and clinical researchers are key actors in translating evidence-based medicine into their clinical practice and questioning its daily application in the care of their patients [1]. They have to develop skills and scientific knowledge and be aware of current emerging concepts in the area of health service research, effectiveness research or translation research, which are fundamental in the development and application of current medicine [2,3]. Integrating all these concepts is challenging but necessary to ensure the viability of the system, as well as the high quality of care. Furthermore, the implication of clinical research physicians is more than needed to assess the feasibility and efficacy of complex clinical interventions and to generate new developments [4].
The management of patients hospitalized with an Acute Coronary Syndrome (ACS) is a well oriented example for the design and implementation of complex interventions integrating concerns on the viability of health care system, translating evidence-based medicine into routine clinical practice and adopting a patient-centered care. This article reviews the main concepts that inevitably influence our practice and present the rationale of a currently performed study.
Current concept
Viability of the current health system: In an era of growing economic pressures and resource shortage in health care, the Swiss health care deciders introduced in January 2012 the DRG (Diagnosis Related Groups) framework based on flat flees financing system in order to improve efficiency, transparency, benchmarking, quality, responsibility and comparability between hospitals whilst containing global health care costs [5]. Such financial incentives have been introduced in the United States of America (USA) 30 years ago and were progressively implemented in several European and Asian countries (for instance Germany in 2004). The DRG is a standardized prospective reimbursement scheme or diagnostic related package for in-patient hospital financing derived from diagnosis categories and subsequent procedures. For each DRG group a range of Length of Stay (LOS) is attributed encouraging physicians to focus on the main diagnosis and treatment, running procedures as efficiently as possible. As consequences hospital costs can be under control if the real hospital LOS tends to the average LOS defined by the DRG system. Previous studies reported a reduction of LOS at hospital after the implementation of DRG-based financing [5-7], but some controversies occurred regarding potential damaging effects on the quality of care of patients or on the professionals’ autonomy and satisfaction. A recent publication provided a framework on some ethical concerns of DRG implementation defined at different levels and themes that were interdependant: (1) macro-level (viability of the health system, quality of the health care system, development of actors and political organizations), (2) meso-level (hospital organization, complex management) and (3) micro-level (interaction between patient and care givers in the systemic context) [8].
Optimal hospital length of stay: LOS duration for patients hospitalized with a STEMI (ST-elevation myocardial infarction) has considerably and naturally decreased with the improvement of treatment and the adoption of clinical guidelines [9]. The first randomized controlled addressing this issue was performed in 1988 and concluded that three days of hospitalization was feasible and safe in selected uncomplicated patients [10]. Another randomized controlled trial, the PAMI-II trial, reported that low-risk STEMI patients had similar outcomes if they were discharged within 3 days compared to usual care (median 7.1 days). The low-risk criteria were: age ≤ 70 years, left ventricular ejection fraction > 45%, one- or- two-vessel disease, successful PCI and no arrhythmia [11]. A time-event based analysis in 41021 STEMI patients treated with thrombolysis in the GUSTO (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) trial determined an ideal discharge date after 4 days in terms of risk/benefit ratio in uncomplicated patients [12]. A cost-effective analysis with 22’361 patients in the same cohort showed that hospitalization of patients with an uncomplicated STEMI was economically not attractive beyond 3 days [13]. With the widespread use of Percutaneous Coronary Intervention (PCI) in the treatment of STEMI, a new prognostic score (the Zwolle index PCI score) was developed in 1’791 patients treated successfully with PCI to identify patients for early discharge (between 48 and 72 hours, Table 1) [14]. This score included the following variables: age, anterior infarction, Killip class, ischemic time, postprocedural flow and multivessel disease. The patients with a score ≤ 3 points had a 30-day mortality rate < 1% and were eligible to be safely discharged within 72 hours. The safety of those STEMI patients seemed not to be worsened by shortening of LOS, since no association of LOS with increased mortality or readmission within 30 days was clearly found. [9,15,16]. However, a post-hoc analysis of 5571 STEMI patients (APEX-AMI trial, Assessment of Pexelizumab in Acute Myocardial Infarction) reported higher rate of 30-day readmission in the USA compared to other countries, but the difference was greatly attenuated after adjustment for LOS limiting a strong conclusion [17]. One of the potential explanations was that USA patients might also not benefit from a prompt follow-up due to the lack of universal health insurance coverage. These results should therefore be confirmed in other studies.
| Killip Class | Points |
|---|---|
| 1 | 0 |
| 2 | 4 |
| 3-4 | 9 |
| TIMI flow post | |
| 3 | 0 |
| 2 | 1 |
| 0-1 | 2 |
| Age | |
| < 60 | 0 |
| ≥ 60 | 1 |
| 3-vessel disease | |
| No | 0 |
| Yes | 1 |
| Anterior infraction | |
| No | 0 |
| Yes | 1 |
| Ischemia time (> 4 hours) | |
| No | 0 |
| Yes | 1 |
| Total | 16 |
Table 1: Zwolle Risk Score for STEMI (from Giuseppe De Luca et al., Circulation 2004) [14].
Application of Evidence-Based Medicine: The European Society of Cardiology (ESC) STEMI 2012 guidelines also proposed recommendations on logistical issues for hospital stay and suggested that early discharge (after approximately 72 hours) was reasonable in selected low-risk patients according to the Zwolle index score, if early rehabilitation and adequate follow-up was arranged (Class IIb, Level B) [18] (Table 2). However, the feasibility of an early discharge in real practice is in fact underused [19]. A large study population of 54’174 patients reported important disparities in patients ‘LOS after an acute myocardial infarction and significantly longer stay in European compared to non European countries, the widespread implementation of early discharge depending on the acceptable risk and the societal readiness to pay incremental costs for prolonged hospitalization [20]. A more recent Italian study showed that only 26% of STEMI patients eligible for early discharge were discharged within 4 days suggesting that there is ample room for a more efficient management [21]. In Switzerland, the mean LOS of patients hospitalized with a STEMI from 1997-2007 was shown to be particularly long (9.5 days) and the attributed costs particularly high (12’100 Euro) [22]. A cost analysis in 2008 for Switzerland reported that direct costs related to the hospitalization represented 43% of the entire costs related to ACS [23]. Safety concerns are probably one of the reasons for prolonged hospital stay, although PCI has dramatically improved prognosis and patients are able to start early mobilization and receive standardized explanation on lifestyle modification and medication. Implementation of an early discharge strategy after an ACS should also focus on the outpatient care system, especially Cardiac Rehabilitation (CR), since it will help patients to regain their normal life and to reinforce cardiovascular secondary prevention strategies. This will require shifting some components of patient’s management from the inpatient to the outpatient care setting, which is a major coordination task to resolve [19]. CR is known to improve prognosis of patients after an ACS and is strongly recommended in guidelines [24], but still dramatically underused [25]. Reasons for non-attendance are multiple (lost of contact, insurance barrier, need to return to work, transportation difficulties), but also include the long median time (35 days in USA) from hospital discharge to program enrolment, which is a considerable gap in the quality of care system [26]. Early appointment to CR within 10 days after discharge is known to improve significantly attendance rates and compliance during the entire CR program [27]. Addressing the issue of early appointment of CR is a crucial step in the implementation of an early discharge strategy after an ACS, also in term of productivity costs after discharge [28].
| 2012 ESC Guidelines of the management of STE-ACS | ||
|---|---|---|
| Recommendations | Class | Level |
| All hospitals participating in the care of STEMI patients should have a coronary care unit equipped to provide all aspects of care for STEMI patients, including treatment of ischaemia, severe heart failure, arrythmia and common comorbities. | I | C |
| Length of stay in the coronary care unit | I | C |
| Patients undergoing uncomplicated successful reperfusion therapy should be kept in the coronary unit for a minimum of 24h, after which they may be moved to a step-down monitored bed for another 24-48h. | I | C |
| Transfer back to a referring non-PCI hospital | ||
| Early transfer (same day) may be considered in selected, low-risk patients after successful primary PCI without observed arrythmia. | IIb | C |
| Hospital Discharge | ||
| Early discharge (after approximately 72 h) is reasonable in selected low-risk patients, if early rehabilitation and adequate follow-up are arranged | IIb | B |
| 2011 ESC Guidelines of the management of NSTE-ACS | ||
Table 2: 2012 ESC Guidelines for Logistic issues for hospital stay [18,33].
The gap of evidence for the burden NSTE-ACS: Most studies addressed this logistic issue in patients with STEMI but very few in patients with NSTE-ACS (Non ST-elevation Acute Coronary Syndrome) [29]. The growing economic burden of patients admitted with NSTE-ACS is expected to exceed the costs of STEMI patients [23]. The application of updated guidelines improved the prognosis of patients hospitalized with NSTE-ACS, thank/inherent to the increased use of coronary revascularization [30]. However, the optimal timing of revascularization with NSTE-ACS is still debated due to a lack of evidence, especially the benefit of early revascularization [31]. In a large dataset of 39’107 patients with NSTEMI (Non ST-Elevation Myocardial Infarction) in the USA, delay to catheterization (> 48 hours) and hospital admission on a Friday afternoon or evening prolonged the LOS [32]. The authors concluded that further research was needed to promote early discharge in patients with NSTEMI in a context of restrictive health care resources. The current ESC NSTEACS Guidelines recommend a minimal hospitalization of 24 hours after the culprit lesion revascularization and the pursuit of care in CR. However, the concept of early discharge has not been clarified for these patients [33].
Patient-centered care: Whilst discussing economic, safety, risk stratification, quality and logistic issues in the care of patients with ACS, we should not forget to integrate patient-centered care. Patientcentered care is one of the targeted goals for improving health care [34]. Patient-centeredness is defined as “providing care that is respectful and representative of individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” [35]. In the context of emerging personalized medicine and shared decision making concepts, elevating patients’ preferences, values and needs seems necessary while designing and implementing evidence-based medicine. However considering patients’ satisfaction as a main motor in medical decisions rises some concerns [36]. Clinical data on 6467 patients with myocardial infarction across 25 hospitals in the USA showed that higher patient satisfaction was associated with improved guidelines adherence and lower inpatient mortality, which indicate that patient satisfaction might add extra information on the quality of care of patients [37]. However, the association between short or long LOS and patients’ satisfaction was not observed [38]. In order to satisfy patients’ demand in clinical decisions might lead to disproportionate diagnostic exams, therapeutic procedures, and subsequent worse clinical outcomes. As a consequence, physicians have the duty to use resources efficiently and to balance these different conflicting issues. Keeping patients longer than needed might have unfavorable impact on patients due to psychological reasons, insufficient mobilization, hospital infection, patient discomfort and bed capacity [39]. This last issue is especially relevant in high-volume PCI tertiary settings working at full bed capacities.
We design this study to assess the feasibility of a systematic early discharge strategy in patients hospitalized for an ACS with a low risk of complications. As primary outcome, we will measure the LOS comparing two different periods at our hospital: (1) observation phase (usual care, 2012-2013) and (2) intervention phase for an early discharge strategy (2013-2014). We will use administrative data to assess the LOS based on admission and discharge date and time. We will measure quality indicators of discharge medications (dual antiplatelet therapy, statin, β-blockers and angiotensin converting enzyme inhibitor/ angiotensin receptor blocker and referral to CR). We will also collect systematically the reasons of not achieving early discharge in eligible patients or reasons of prolonged hospital stay, especially with a focus on the acceptability among patients. The collection of such data might clarify potentials barriers to shorten LOS. Regarding the safety issue, the investigators will contact each participant at 30 days to assess the clinical outcome. We do not expect any increase of readmission rates because participants are per definition at low risk of complications and all had an uncomplicated 24-hour hospital course. In parallel, we will estimate the reduction of costs after the implementation of an early discharge strategy, especially the reduction of directs costs related to the shortened LOS and those related to possible readmissions. Finally, we will ask patients at 30 days to rate their overall satisfaction with provided care using an unvalidated 5-point Likert scale questionnaire. This protocol was approved by the Geneva Ethical Committee on Human Research and all participants to this study gave written informed consent.
Rationale for a non-randomized trial
One randomized controlled trial assessed the safety and the feasibility of an early discharge strategy (hospitalization of 72 hours) compared to usual care in 54 low-risk patients with a STEMI. The median LOS was similar in both groups (55 hours) and the statistical power too limited to make any conclusion on safety [40]. For this study, we examined the feasibility of a randomized trial with a non-inferiority hypothesis as previously performed in the outpatient treatment of pulmonary embolism [41]. To calculate the estimated sample size, we had to define two parameters besides alpha (0.05) and power (0.80): the outcome rate and the margin of non-inferiority. Considering a primary safety composite cardiovascular endpoint of death, myocardial infarction, stroke or recurrent ischaemia, we expected a very low event rate at 30 days (2%). With a non-inferiority margin of 0.5% (acceptable clinical risk), we finally obtained a total sample size of 24’622 patients. A non-inferiority randomized study was therefore abandoned because of the too large sample size, which was also due to a research question focusing on safety instead of feasibility. Furthermore, randomization at the patient level was problematic in an intervention study aiming to act also at the hospital organization, thus influencing all participants, even those assigned to usual care (non-early discharge group). Therefore, we chose a time-series design and a primary outcome of efficiency and feasibility, such as LOS. The LOS will be measured before and after the implementation of the early discharge strategy using administrative data (Figure 1). For the power calculation, we estimate that the usual mean LOS of patients hospitalized for ACS is 4.5 days and the deviation standard 1.9 days (results based on the local previous data). With the implementation of an early discharge strategy, we expect to reduce LOS of 20%. We calculate that 100 patients per treatment group will provide 90% power to detect superiority using a one-sided alpha of 0.05. As the primary outcome will be a continuous variable (LOS), we will use a parametric test (t-test) to compare the LOS between both phases: observation (2012-2013) and intervention phase (2013-2014) and a non-parametric test (Wilcoxon rank sum test) if the distribution of LOS does not satisfy the normal distribution. We will use descriptive statistic tests to compare baseline characteristics between both groups and in case of significant differences, these variables will be used to adjust the comparisons of LOS. The safety will be measured as secondary endpoint, such as the assessment of the occurrence of major cardiovascular events 30 days. The sample size and the design of the study have not been performed to assess the non-inferiority of an early discharge strategy, but the feasibility of a recommended strategy in the real practice. This design is justified, as the selected patients are per definition at low risk of complications and the safety well accepted in the guidelines.
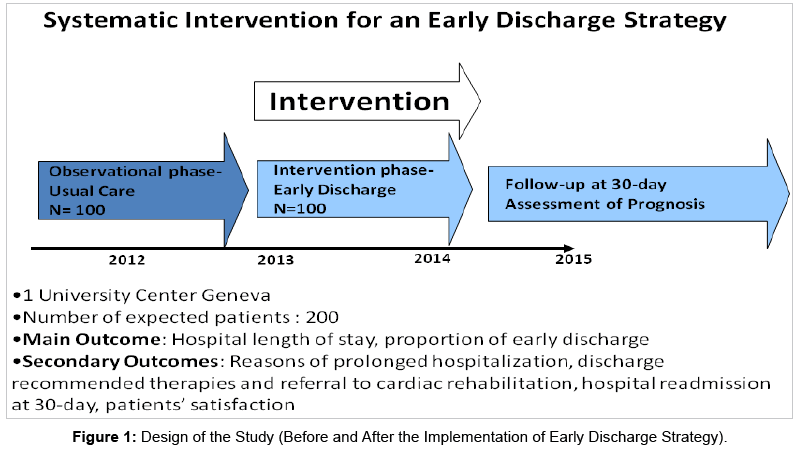
Figure 1: Design of the Study (Before and After the Implementation of Early Discharge Strategy).
Description of population
We will perform this study at the Geneva University hospitals, in the Western part of Switzerland, which is the reference centre for acute coronary revascularization in the region.
Two catheterization laboratories as well as intermediate and intensive coronary care units are available on a 24 hours/7 days basis. Patients aged 18 years or older with the following criteria will be eligible: hospitalization with the main diagnosis of ACS, successful treatment by PCI, uncomplicated 24-hour hospital course, ≤ 3 points on the Zwolle primary PCI-index risk score. The Zwolle primary PCIindex (Table 1) is a clinical model for the 30-day mortality prediction in STE-ACS patients that permits the identification a large subset of low-risk patients (score ≤ 3) [14]. This score was derived in 1791 patients (c statistic = 0.907) and validated in 747 patients (c statistic = 0.902). Figure 2 shows the trial flowchart. We will exclude patients with one or more of the following criteria: procedural complications, peri-procedural myocardial infarction (type 4a), non-atherosclerotic lesions (for instance coronary spasm on cocaine use, coagulopathy, patent foramen ovale), ACS following a surgical procedure, additional coronary lesions requiring staged PCI treatment during the index hospitalization, cardiac tamponade, bleeding requiring further investigations, left ventricular ejection fraction < 40%, severe renal failure (estimated glomerular filtration rate < 30 mL/min/1.73 m2 based on the Cockroft-Gault equation), persistent arrhythmia during 24-monitoring, uncorrected severe hyperglycemia (> 15 mmol/l), severe physical disability, dementia or other clinical conditions requiring hospitalization, language barriers and patients transferred to outside hospitals.
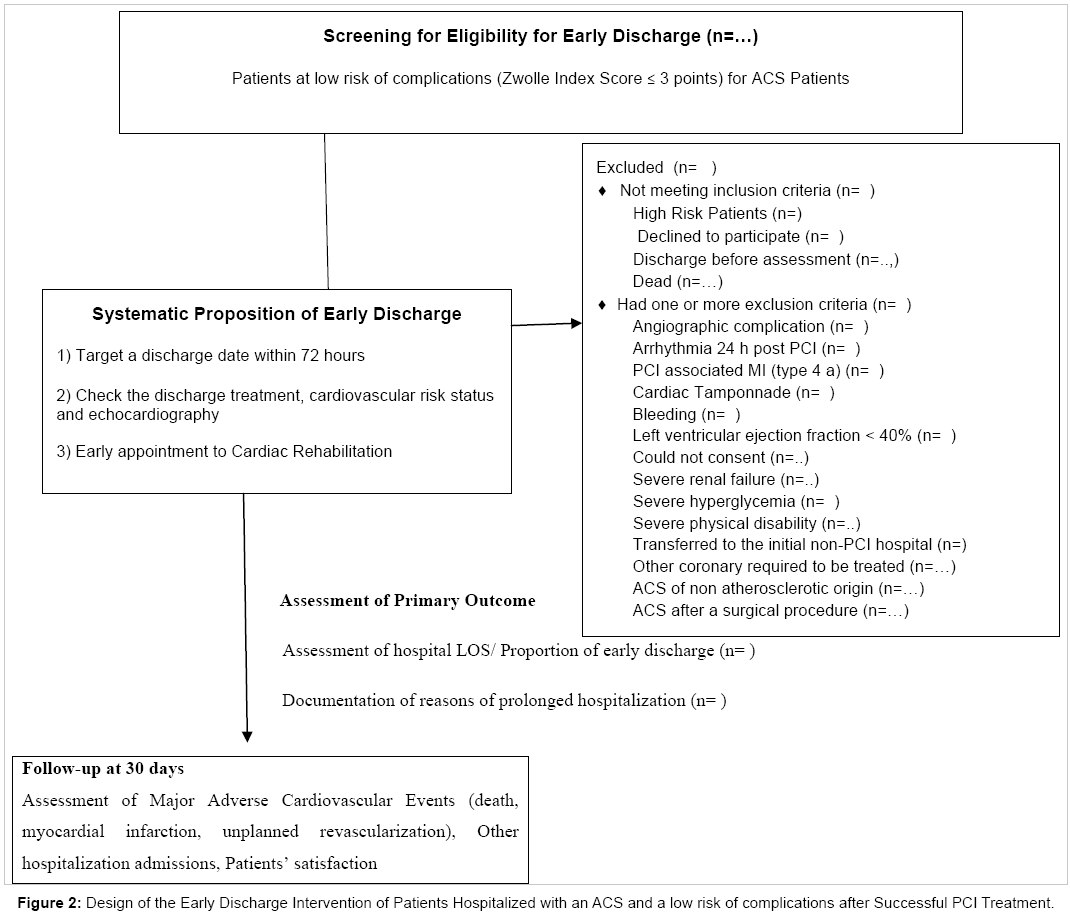
Figure 2: Design of the Early Discharge Intervention of Patients Hospitalized with an ACS and a low risk of complications after Successful PCI Treatment.
Description of intervention
During the early discharge intervention, the low-risk patients will be actively targeted for an early discharge with a LOS of 72 hours (3 days). We designed the measures based on a previous published matrix that classified actions on admission, during the stay and at discharge (Table 3) [42]. Briefly, we will work on four axes: (1) Systematic identification of low-risk patients using the Zwolle primary PCI index (the assessment will be performed shortly after PCI); (2) Targeting a discharge date within 72 hours of admission time at the beginning of hospitalization; (3) Coordination of recommended clinical exams (early request for a transthoracic echocardiogram and shift of symptom-limited exercise stress testing to the outpatient setting), care (early mobilization) and systematic cardiovascular prevention education counseling (http://elips.hug-ge.ch, the ELIPS program was implemented in our institution and aimed at educating patients using different tools, such as a film, an internet site, flyers, a discharge medication card and a wall chart); (4) Systematic outpatient CR appointment will be programmed. The CR team will recruit actively participant in the ward and promote the accessibility to the program. The appointment date will be organized shortly after discharge (< 10 days) and patients will be offered discount on public transportation during the entire CR program, as well as a rent of an electric bicycle during one week. The on-call cardiologist will be available 24h/24h for the patients after discharge if they need any information or advice [33].
| General Measures | Specific to the study |
|---|---|
| Admission | |
| On admission anticipate and evaluate the discharge situation | Target a discharge within 72 hours after discharge in partnership with the low-risk patient |
| Stay | |
| Intensify supervision and communication from physicians to residents | Systematic identification of low-risk patients with PCI Zwolle Index Score |
| Improve communication and cooperation between physicians and nurses | Establishment of clinical itinerary and fast transfer from coronary unit to the cardiology ward |
| Optimise the number of beds for each ward and make arrangements about 'own beds' so that these beds will not be occupied by other specialties | Care of patients in specialized cardiology division, avoid dissemination of low-risk coronary patients in other specialties |
| Reducing waiting times for diagnostic tests or interventions | Limit clinical exams according to recommendations. Request an early echocardiography and shift some exams in outpatient setting (treadmill test) |
| Optimise cooperation with paramedics and stimulate early rehabilitations | Early mobilization with a shortened time, start of secondary prevention using ELIPS program (film, motivational interviewing) |
| Discharge | |
| Work up to an expected discharge date | Target a discharge within 72 hours after discharge in partnership with the low-risk patient |
| Stipulate conditions at which discharge at weekends is possible | Encourage patients and physicians to anticipate a discharge at weekends |
| Develop a team of effective discharge planners | A team of CR will recruit participant at hospital stay for the program |
| Arrange effective aftercare in the outpatient department | Systematic referral to the CR unit within 10 days |
| Make good use of the next health care facilities | Offer to the patients a public transportation discount during the CR program |
| Arrange follow-up care in order to avoid delays discharging patients | Increase CR program resources to shorten time the appointment after discharge |
Table 3: Identified measures to reduce LOS based on previous published matrix [38].
The aim of our project is to improve clinical effectiveness while maintaining quality care of patients hospitalized with low-risk ACS. We plan to implement an early discharge strategy (approximately 72 hours of hospitalization) as recommended by the ESC Guidelines. Using time-series analysis, we will assess the evolution on LOS and expect to show an incremental decrease of LOS after the introduction of the strategy. Early discharge is currently not applied in the care of patients, although the health system is under growing economic pressure. We design our intervention on four main measures: (1) systematic selection of low-risk patients; (2) target an early discharge date at the beginning of hospitalization, (3) coordinating complementary exams and (4) proposing a systematic early enrolment in a CR program. We expect to add new insights in the research area of clinical effectiveness, as well as to develop health system research in the context of growing concerns on the sustainability and viability of the costly health care system.
Dr Gencer and Professor Mach’s research on cardiovascular prevention is supported by grants from the Swiss National Science Foundation (SNSF 33CM30- 140336). Dr Gencer’s research on cardiovascular epidemiology is supported by a grant from Geneva University Hospital (CGR 71-225) for the development of research projects.