Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2015) Volume 0, Issue 0
In order to assess the beneficial and harmful effects of biliary stenting via ERCP for pancreaticobiliary stricture confirmed or suspected to be malignant, prior to surgery, we identified trials through Pubmed (1950 to June 2013), Science Citation Index Expanded (1945 to June 2013), and EMBASE (1980 to June 2013). Three authors independently selected trials for inclusion and extracted data. The primary pre-surgical, post-surgical, and final outcome measures were mortality. The secondary outcomes were complications such as cholangitis, pancreatitis, bleeding, pancreatic fistula, intra-abdominal abscess, improvement in bilirubin, and quality of life. Dichotomous outcomes were reported as odds ratio (OR) with 95% confidence interval (CI) based on fixed- and random-effect models. We identified three randomized trials with 634 patients undergoing pancreatico-duodenectomy; 500 patients underwent ERCP with biliary stenting and 134 had ERCP without biliary stenting prior to surgery. Pre-surgical mortality was not significantly affected by stenting (OR 3.14, 95% CI 0.12 to 79.26), while there were significantly more complications in the stented group (OR 18.41, 95% CI 2.46 to 137.85). However, postsurgical complications were significantly less in the stented group (OR 0.31, 95% CI 0.21 to 0.48). Overall mortality (OR 1.05, 95% CI 0.46 to 1.71) and complications (OR 0.31, 95% CI 0.21 to 0.48) were not significantly different in the two groups. We could not find convincing evidence to support or refute endoscopic biliary stenting on the mortality in patients with pancreaticobiliary malignancy. Large randomized trials are needed to settle the question of pre-surgical biliary stenting.
<Keywords: ERCP; Pancreaticobiliary malignancy; Randomized trials
Endoscopic retrograde cholangiopancreaticography (ERCP) is a complex diagnostic and therapeutic approach that is used to identify and treat various hepatobiliary and pancreatic diseases [1]. About one third of the patients with pancreatico-biliary malignancy are amenable to surgical resection after detailed evaluation with trans-abdominal ultrasound, computerized tomographic scan, magnetic resonance cholangiopancreaticography (MRCP), and endoscopic retrograde cholangiopancreaticography (ERCP). Biliary obstruction is a frequent presenting feature of pancreaticobiliary malignancy [2]. Corrective surgery is the therapy of choice, but the majority of patients with pancreatico-biliary malignancy are incurable at the time of diagnosis due to local or distant metastases. Surgical treatment is found to be the best available option for patients diagnosed at a stage where the tumour is confined to the biliary tract. There are two ways to approach patients who are fit for surgical treatment: direct surgical approach or pre-surgical biliary decompression [3]. We have been unable to identify systematic reviews or meta-analyses of randomized clinical trials on the issue. We decided to explore the utility of preoperative endoscopic biliary drainage in patients with pancreatico-biliary stricture confirmed or suspected to be malignant, prior to surgery, by examining all randomized trials in a Cochrane systematic review [4]. We only included trials that compared ERCP with stenting versus ERCP without stenting. Clinical trials on non-endoscopic preoperative drainage will be considered in other systematic reviews.
Criteria for considering studies for this review
Types of studies: We included all randomized clinical trials, which compared presurgical endoscopic biliary drainage with no pre-surgical drainage in patients awaiting surgical procedure for a pancreaticobiliary stricture confirmed or suspected to be malignant. We excluded historically controlled trials, cohort studies, and case series. This decision was taken knowing that it may only be a select group of studies we were able to identify. In spite of the fact that our wish to include such non-randomized studies as a kind of ‘quality control’ on the results from the randomized trials, we stress the risky nature of such control.
Data collection and analysis: Three authors (LM and SH) extracted the pre-specified characteristics of the included trials independently. We sought the opinion of the third author (WJ) in case of disagreement. We performed meta-analyses following the instructions given in the Cochrane Handbook for Systematic Reviews of Intervention and the Cochrane Hepato-Biliary Group Module.
Selection and data-extraction: We retrieved full articles for assessment and applied independently the inclusion criteria to all potential studies. From each trial we extracted age, gender, symptoms, biochemical laboratory parameters, including serum bilirubin, transaminases, alkaline phosphatases; type of the tumour such as periampullary carcinoma (pancreatic head tumour, duodenal tumour, ampullary tumour), or cholangiocarcinoma involving intra-hepatic, peri-hilar or distal bile duct along with pathologic diagnosis. We recorded ERCP findings with specifications of the biliary stent used, alongside with complications arising during ERCP and stenting such as pancreatitis, cholangitis, and bleed; the mortality related to the surgical intervention in both groups; and retrieved the data of surgical outcome in patients from both the groups. Two of the authors analyzed all the included randomized trials independently and solved eventual disagreements by discussion.
Statistical methods: We used Review Manager 4.2 (RevMan 2003). We used the intention-to-treat principle when analysing the data, that is, patients with missing data were considered treatment failures. Binary outcomes were expressed as relative risks (RR) and continuous outcomes as weighted mean differences (WMD) both with 95% confidence intervals (CI). We employed both randomeffects and fixed-effect models. We reported the fixed-effect results when there was no discrepancy between the two models (both showing a significant intervention effect and both showing no significant intervention effect). Discrepancy between the two methods occurs only when there is heterogeneity. We will explore sources of heterogeneity in assessment of treatment response in meta-regression analyses and subgroup analyses if enough trials are identified. When the number of trials allow, we will perform the following subgroup analyses to determine the impact of trial characteristics.
Search result
The search process of the study is shown in Figure 1. A total of 227 publications were identified after initial search. The titles and abstracts of these articles were examined to exclude irrelevant trials. We also examined the reference lists of all relevant letters, editorials and review articles. As a result, three articles possibly meet the selection criteria (Figure 1).
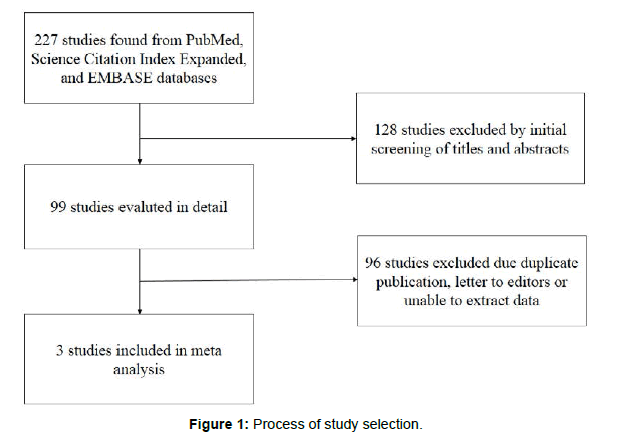
Figure 1: Process of study selection.
Pre-surgical outcome
Pre-surgical mortality was not significantly affected by stenting (OR 3.14, 95% CI 0.12 to 79.26) (Figure 2).
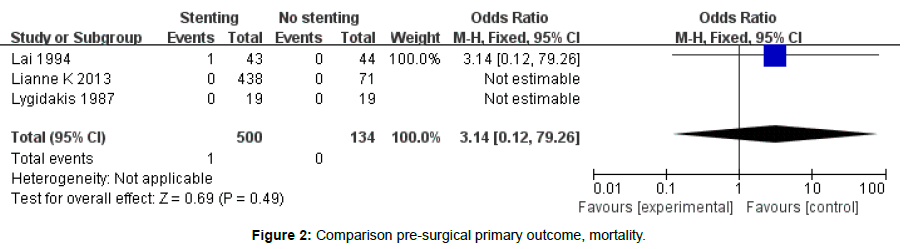
Figure 2: Comparison pre-surgical primary outcome, mortality.
There were significantly more complications in the stented group (OR 18.41, 95 % CI 2.46 to 137.85) (Figure 3).
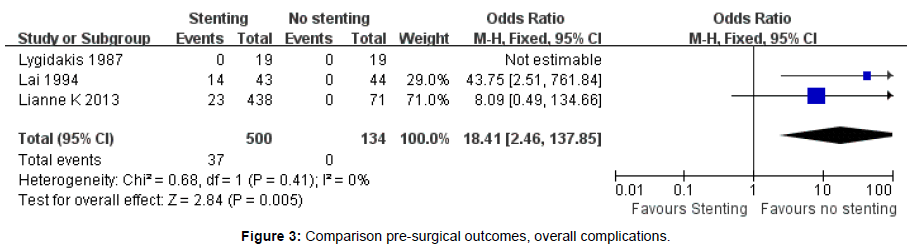
Figure 3: Comparison pre-surgical outcomes, overall complications.
Postsurgical outcome
Postsurgical complications were significantly less in the stented group (OR 0.31, 95% CI 0.21 to 0.48) (Figure 4).
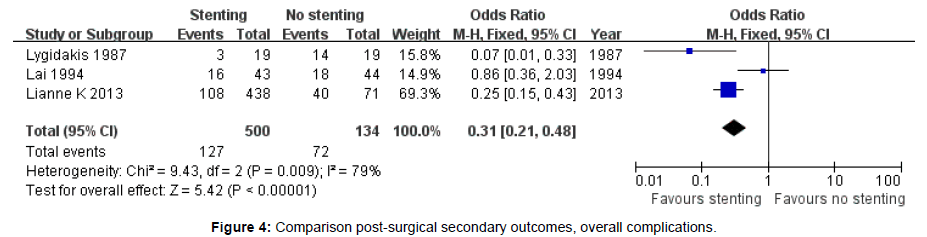
Figure 4: Comparison post-surgical secondary outcomes, overall complications.
Overall mortality (OR 1.05, 95% CI 0.46 to 1.71) and complications (OR 0.31, 95% CI 0.21 to 0.48) were not significantly different in the two groups (Figure 5).
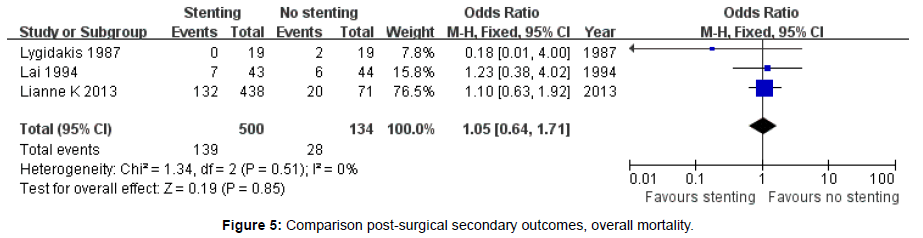
Figure 5: Comparison post-surgical secondary outcomes, overall mortality.
Bleeding
Bleeding occurred in 4/62 patients in the stented group versus 0 / 63 patients in the no stented group (OR 1.86, 95% CI 1.15 to 22.48)(Figure 6).
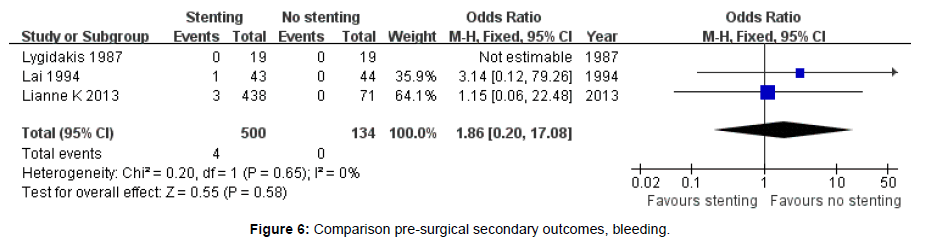
Figure 6: Comparison pre-surgical secondary outcomes, bleeding.
Diagnosis outcome
Pancreatic carcinoma diagnosis were significantly in the stented group (OR 0.49, 95% CI 0.32 to 0.74) (Figure 7).
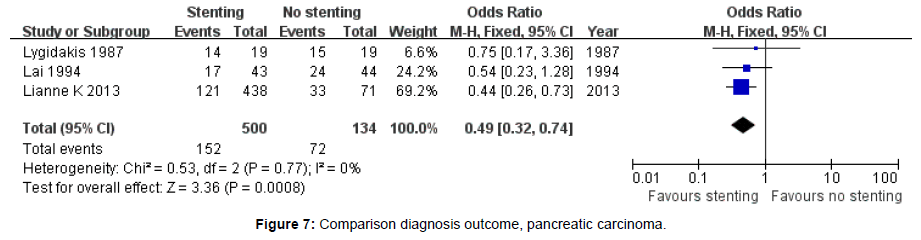
Figure 7: Comparison diagnosis outcome, pancreatic carcinoma.
Periampullary carcinoma diagnosis were not significantly in the stented group (OR 1.29, 95% CI 0.69 to 2.42) (Figure 8).
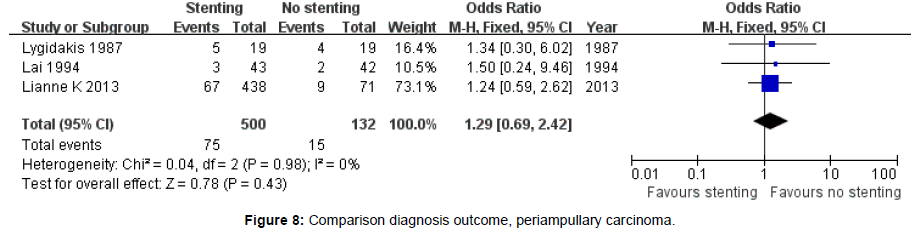
Figure 8: Comparison diagnosis outcome, periampullary carcinoma.
There has been a significant evolution in biliary drainage procedures over the last three decades in order to improve morbidity and mortality in patients with biliary obstruction awaiting corrective surgery [5]. We found that ERCP with stenting has no significant harmful or beneficial effect on post-surgical mortality.
Earlier attempts at biliary drainage mainly related to the percutaneous route. The concept of biliary drainage in this context was proposed in 1970s, when Takada et al. [6] in a non-randomized study found that mortality fell from 28% to 8% when percutaneous biliary drainage was performed in patients with malignant jaundice before a surgical procedure [7,8]. Further non-randomized studies by Nakayam and Gobien [9] also found pre-surgery percutaneous biliary drainage to be useful. In 1980s, Denning and Grundy [10,11] again demonstrated effectiveness of percutaneous biliary drainage in non-randomized cohort studies [10,11]. In order to confirm this finding, Hatfield , McPherson, and Pitt [12-14] conducted randomized trials and showed that, in fact, mortality and morbidity were higher in percutaneous biliary drainage patients as compared to those who went to surgery directly [15,16].
Similarly Karsten [6] in their 30 patients studied the morphological changes of the extra-hepatic biliary tract during obstruction and the effects of biliary decompression by means of an endoprosthesis on the bile duct wall by light microscopy and scanning electron microscopy. They found that their patients with endoprosthesis were having severe inflammatory changes with considerable fibrosis and ulcerative lesions, resulting in markedly thickened ducts with lumina approximating the diameter of the stent [17,18]. On the other hand, the patients with obstructed ducts without endoprosthesis had mild inflammation, a moderate degree of fibrosis, and local epithelial disintegration. Though the above evidence is not conclusive, it appears that there is likelihood that the local inflammation due to stent can cause operative problems, such as difficult dissection, increased per-operative bleeding and thickening of the bile duct with fibrosis causing anastomosis problems [19,20].
When we analysed the results of three trials together, we found that the rate of overall post-surgical mortality was not significantly different in the groups that did or did not have pre-surgical stent placement, but that there was weak evidence of benefit of presurgical stenting in preventing post-surgical complications.
There is a need for a large randomized trial with good collaboration between gastroenterologists and surgeons to settle this very important issue of presurgical drainage in patients with pancreatic-biliary malignancy. Furthermore, whenever such trials are designed, they must address the issue of surgical problems with or without stenting [17].
On the basis of the only three randomized high-bias risk trials included in this systematic review, pre-surgical endoscopic biliary drainage in patients with malignant pancreaticobiliary stricture awaiting surgery cannot be supported or refuted [18].
Further properly designed randomized trials with sufficient statistical power, adequate generation of the allocation sequence and allocation concealment, and adequate blinding of outcome assessment should be initiated to evaluate the use of pre-surgical endoscopic biliary drainage in patients with malignant pancreaticobiliary stricture awaiting surgery. This clinical practice of endoscopic biliary drainage must be avoided until result from such trials can guide future practice [20,21]. Furthermore, future trials should also provide data regarding additional, clinically relevant aspects, such as duration of hospital stay, frequency of post ERCP cholangitis, pancreatitis, individual postsurgical complications, and problems during the following surgery. None of the trials has dealt with the important issue of quality of life so it has to be incorporated in the future trials also. Future trials ought to be reported following the CONSORT Guidelines [22].