Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 5
Background: Majority of the elderly people complain of difficulty in sleeping. Although the causes for the sleep disturbances may be multifactorial in nature, the sleep disordered breathing (SDB) is one of the primary disorder. The study was undertaken to study the effect of complete denture rehabilitation which could have profound impact on rehabilitation protocol on complete edentulous patients.
Aim: The aim of this study is to cephalometrically evaluate the effect of complete denture rehabilitation on upper airway dimensions and position of hyoid bone and also to examine if complete denture rehabilitation influences oxygen saturation and degree of sleepiness by overcoming upper airway collapsibility.
Material and Method: Of 30 edentulous patients who complained of snoring during sleep were selected for the study. The baseline lateral cephalogram of all the patients were taken by asking the patient to attain the natural head position. MAS (Minimal Airway Space), PAS (Posterior Airway Space), SAS (Superior Airway Space), MP-H (Perpendicular distance from hyoid bone to mandibular plane) were also recorded. The patients were also subjected to pulse oximetry test to assess the oxygen saturation and ESS (Epworth Sleepiness Scale) to assess the day time sleepiness. All these subjects were rehabilitated using conventional complete denture fabricated using standard prosthodontic protocol and after 6 weeks to 8 weeks they were subjected to same tests again with dentures in situ.
Results: The results of this study showed no statistically significant difference on minimal airway space (MAS), posterior airway space (PAS), superior airway space (SAS), perpendicular distance from hyoid bone to mandibular plane (MP-H), epworth sleepiness scale (ESS) and oxygen saturation.
Conclusion: Wearing the complete denture during night does not improve the airway space, oxygen saturation and day time sleepiness significantly among edentulous patients.
Keywords: Sleep disordered breathing, Obstructive sleep apnea, Epworth sleepiness scale
Disturbed sleep is a common source of disgruntlement among elderly people. It is estimated that up to 50% of elderly adults complain of difficulty in sleeping, further aggravating the risks of morbidity in the ageing population [1]. It has been described that 43% of those over the age of 65 have difficulty in the onset and maintenance of sleep, while 25% report daily drowsiness [2].
Many authors in 1970 delineated the causes of upper airway sleep disorders and in 1980 they described the oral appliances as pivotal treatment modality. Drowsiness and symptoms of sleep disturbance have been associated with declining cognitive capacity, depression, falls and mortalities. Sleep disturbances are multifactorial in nature and could be impacted by alterations of the circadian rhythm, neuropsychological impairment, use of medications and some medical conditions.
In most of the cases disturbed sleep is constantly associated with sleep-disordered breathing (SDB) which can range from the cessation of respiration lasting for at least 10 seconds (apneas) and or partial or reduced respiration (hypopneas) during sleep [3].
One of the exacerbating factors that were recommended to worsen SDB is edentulism. Complete tooth loss sequels in anatomical changes that may sway upper airway dimensions and pass out by influencing the postural rest position of the mandible, muscle tone and tongue posture during sleep. A decrease in retropharyngeal space and or the hypotonicity of the pharyngeal musculature in edentulous people have been recommended to increase the collapsibility of airways [4].
Using supine lateral cephalometric studies in complete denture wearers, they substantiated decrease in retropharyngeal space and anteroposterior oropharyngeal distance in the absence of dentures. They found that there may be perpetuation of obstructive sleep apnea (OSA) and lower arterial hemoglobin oxygen saturation in patients following the removal of dentures. Thus, they collectively assign edentulism as a reason for exacerbation of OSA [5].
There are very few studies to analyze the role of complete denture rehabilitation on the upper air way dimension and its influence on oxygen saturation to analyze and assess whether edentulism favors the occurrence or alleviating of OSA which would have intense effect on rehabilitation protocol in complete edentulous patients with SDB.
A repeated design measure study was undertaken. The samples were selected from the completely edentulous patients visiting our institution seeking complete dentures. All patients were informed of the modalities and purpose of the study before obtaining consent to participate.
The inclusion criteria for the study were first time complete edentulous patients with well-formed residual ridges in class I relation, presence of snoring or known case of obstructive sleep apnea, age group of between 50 years to 70 years, clinically stable with no systemic involvement especially respiratory disease and infections. The exclusion criteria included any metabolic or craniofacial syndrome, BMI>3, nasal obstruction, pharyngeal tumours, history of tongue, palate or upper airway surgery, skeletal class III relationship, grossly resorbed residual alveolar ridges and musculoskeletal disorders.
All complete dentures were made and assessed by the same clinician at all stages and were fabricated by the same technician in accordance with the standard prosthodontic treatment and laboratory protocol.
The sample consisted of 30 edentulous patients who complained of snoring. Out of which 14 were males and 16 were females with mean age of 63 years. Baseline lateral cephalograms were recorded at the end expiration, palate not involved in deglutition and jaws in physiologic rest position by asking the patients to attain natural head position (NHP) (Figures 1 and 2).
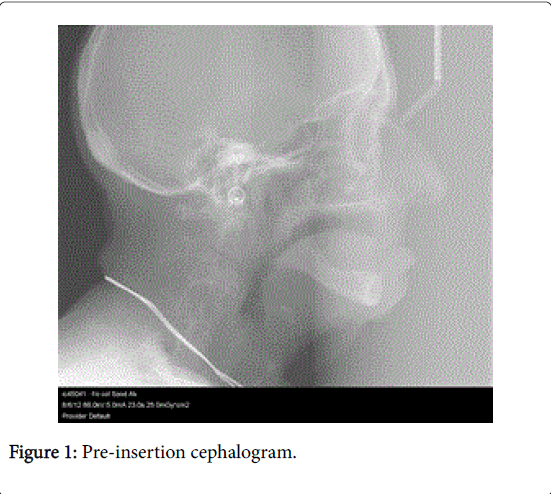
Figure 1: Pre-insertion cephalogram.
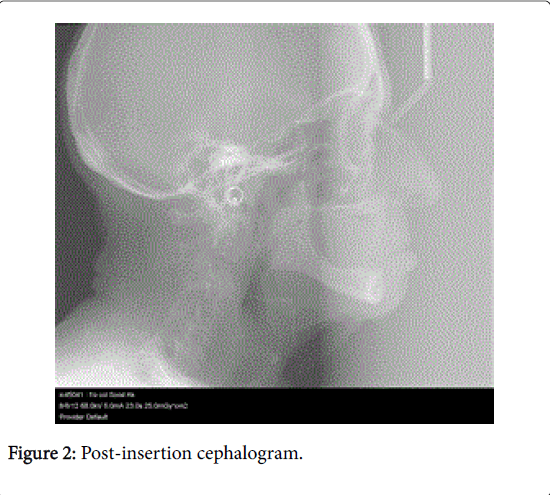
Figure 2: Post-insertion cephalogram.
To attain NHP, patients were made to stand without head fixation in cephalostat, after moving head forward and backward 3 times, swallowing and lips at rest. Exposure time and other parameters were kept constant and radiographs were made with a film object distance of 180 cm and film to median plane distance of 10 cm which was constant for both pre and post cephalometric radiographs.
All the patients were also subjected to overnight pulse oximetry test to assess oxygen saturation and epworth sleepiness scale (ESS) to assess day time sleepiness (Figures 3 and 4).
Figure 3: Sleep study being carried out.
Figure 4: Electrodes attached while doing sleep study.
All the 30 study subjects were rehabilitated with conventional polymethyl methacrylate complete dentures (CD) using standard prosthodontic fabrication protocols.
After 6 weeks to 8 weeks, following the use of CD and having observed the compliance of use, they were subjected to lateral cephalograms with CD in situ as per standardised protocol followed during pre-treatment cephalometry using the same cephalometric machine.
All the rehabilitated study subjects were also subjected to overnight pulse oximetry with wearing CD to assess oxygen saturation and ESS scores were evaluated.
The data recordings of sleep duration lasting for more than 4 h were considered as acceptable for the purpose of our study.
Based on the outer border of the radiograph, vertical and horizontal lines were traced perpendicular to each other.
These two lines acted as references to calculate the angles between the head and neck on the cephalograms and the measurements for posterior airway space (PAS), minimal airway space (MAS), superior airway space (SAS) and perpendicular distance from hyoid bone to mandibular plane (M-PH) (Figure 5 and Table 1).
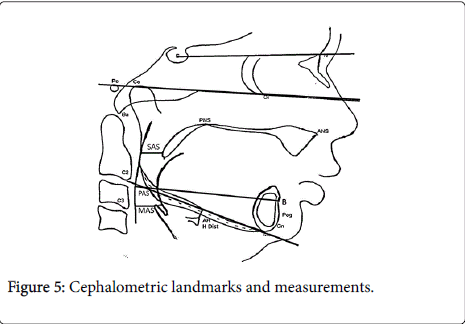
Figure 5: Cephalometric landmarks and measurements.
| S.No. | Cephalometric variables | Definition |
|---|---|---|
| 1) | Superior airway space (SAS) | A horizontal distance from the tip of the soft palate to pharyngeal wall. |
| 2) | Posterior airway space (PAS) | Horizontal distance from the posterior margin of the tongue to pharyngeal wall measured on the B-Go line. |
| 3) | Minimum airway space (MAS) | Minimum horizontal distance between the anterior and posterior wall of pharynx in the oropharyngeal region (or) horizontal distance between the anterior and posterior wall at the narrowest part of oropharynx. |
| 4) | Hyoid distance (H- MP) | A perpendicular distance between the superior most point on the body of hyoid bone and the mandibular plane. |
Table 1: Definitions of various cephalometric measurements.
The mean SAS without dentures was 8.96 mm (± 1.84) and with denture wear was 8.90 mm (± 1.79) with difference in mean of 0.06 (± 0.52). The comparison of means was done using paired t-test, wherein p-value was of 0.48 indicating no statistically significant difference in SAS, between with and without denture wearers (Table 2).
| Variable | Pretreatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| SAS | 8.96 | 1.84 | 8.9 | 1.79 | 0.066 | 0.489 |
Table 2: Effect of wearing complete denture on SAS.
The mean MAS without dentures was 7.00 mm (± 1.59) and with denture wear was 7.30 mm (± 1.46) with difference in mean of 0.30 (± 0.53).
The p-value was of 0.005 indicates statistically significant difference in MAS, between with and without denture wearers (Table 3).
| Variable | Pre treatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| MAS | 7 | 1.59 | 7.3 | 1.46 | 0.3 | 0.005 |
Table 3: Effect of wearing complete denture on MAS.
The mean PAS without dentures was 11.76 mm (± 1.83) and with denture wear was 11.93 mm (± 2.08) with difference in mean of 0.16 (± 0.53). The p-value of 0.096 indicates no statistically significant difference in PAS, between with and without denture wearers (Table 4). The mean H-distance without denture was 11.73 mm (± 1.7) and with denture wear was 11.7 mm (± 2.08) with difference in mean was 0.03 (± 0.85). The p-value of 0.83 indicates no statistically significant difference in H-distance to the mandibular plane, between with and without denture wearers (Table 5).
| Variable | Pre treatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| PAS | 11.76 | 1.83 | 11.93 | 2.08 | 0.16 | 0.096 |
Table 4: Effect of wearing complete denture on PAS.
| Variable | Pre treatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| H - Distance | 11.73 | 1.7 | 11.7 | 2.08 | 0.03 | 0.831 |
Table5: Effect of wearing complete denture on H-distance.
The ESS score without denture was 8.83 (± 1.64) and with denture wear was 8.83 (± 1.81) with difference in mean of 0.00 (± 0.74). The pvalue of 1.00 indicating no statistically significant difference in ESS between with and without denture wearers (Table 6). The oxygen saturation percentage score without dentures was 93.30 (± 1.74) and with denture wear was 93.20 (± 1.58) with difference in mean of 0.10 (± 0.88). The p-value of 0.54 indicates no statistically significant
| Variable | Pre treatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| ESS | 8.83 | 1.64 | 8.83 | 1.81 | 0 | 1 |
Table 6: Effect of wearing complete denture on ESS.
From a methodical viewpoint, sleep is defined on the basis of both the behavior of the person while asleep and related physiological changes that occur to the alert brain’s electrical rhythms in sleep [6]. The behavioral criteria consist of a complete lack of mobility or slight mobility, sluggish eye movements, peculiar sleeping posture, decreased response to external stimulation, increased reaction time and arousal threshold, an impaired cognitive function and a reversible unconscious state. The physiological parameters are based on the findings of EEG, electro-oculography (EOG) and electromyography (EMG).
Sleep apnea, based on the denotation, should have at least five apneas or hypopneas per hour of sleep accompanied by excessive daytime sleepiness (EDS). The manifestations of OSAS can be divided into two groups; those occurring during sleep and those occurring during awake. Nocturnal symptoms includes choking during sleep. Habitual loud snoring and halting of breathing and abnormal motor activities during sleep, severe sleep disruption, heartburn as a result of gastro esophageal reflux, nocturnal enuresis which is seen mostly in children and profuse sweating at night. The daytime symptoms includes sleep attacks lasting 0.5 h to 2 h and occurring mostly when the patient is relaxing i.e. sitting down or watching television.
Increased pharyngeal collapsibility is a frequent cause of obstructive sleep apnea (OSA) [5] which results from the combination of anatomical abnormalities of the upper airway with changes in neural activation mechanisms. Innumerable structural changes in facial morphology have been associated with OSA pathogenesis like retrognathic mandibles, posteriorly placed pharyngeal walls, large tongues and soft palate. Missing teeth produces prominent anatomical changes that may influence upper airway size and function, such as decreased vertical dimension of occlusion, reduction of the lower third facial height and mandible rotation correlating its role in the pathogenisis of OSA [7].
Bucca et al. [5] and Gupta et al. [8] confirmed that removal of dentures significantly decreases the retropharyngeal space and sleeping without dentures is associated with significant decrease in apneahypopnea index (AHI) and decrease in mean arterial hemoglobin saturation. The authors stressed the fact of wearing complete dentures during night will negate the effects of OSA. Their results were in contrast to our study results, wherein there was no significant difference in cephalometric findings in superior airway space (SAS) (Table 2) and posterior airway space (PAS) (Table 4) whereas there was a significant difference in minimal airway space (MAS) (Table 3) between patients with and without complete dentures. This could be because our study sample was of non-confirmed cases of OSA with only snoring as an inclusion criteria.
Carossa et al. [9] described the effect of removal of dentures and modifications of prosthesis on pharyngeal collapse and showed statistically significant reduction in PAS. They concluded that wearing denture induces modifications in the position of tongue, the jaw and the pharyngeal air way space which was not in accordance with our study. This may be because of the selection of sample size of 27 subjects with reduced vertical dimension compared to our study sample of ideal jaw relations.
Gupta et al. [4] evaluated completely edentulous patients cephalometrically with increasing vertical jaw relation using an acrylic jig of 2 mm to 3 mm and revealed that there was a statistically significant correlation between PAS and retropharyngeal space between edentulous and patients with complete dentures and they concluded that increasing vertical dimension of occlusion within acceptable limits is beneficial to patients with OSA.
Ariska et al. [10] and Bucca et al. [11] had evaluated the risk for OSA in completely edentulous patients with and without complete dentures respectively and concluded that the episode of AHI increases along with reduction in oxygen saturation and retropharyngeal space without dentures indicating worsening of the OSA among subjects. But although there was a definite improvement of AHI among all denture wearers, the oxygen saturation level was recorded at 95.4 ± 2.4 without dentures and 95.6 ± 1.6 with dentures indicating no statistically significant difference. This result is in concurrence to our study wherein the oxygen saturation level was recorded at 93.30 ± 1.74 without dentures and 93.20 ± 1.58 reveling no statistically significant difference.
In a study by Tsuda et al. [12], they demonstrated that edentulism favors upper airway obstruction during sleep. In fact, both AHI and mean SaO2 were significantly worse in the patients who slept without dentures than in the patients slept with dentures. Almeida analysed completely edentulous patients with OSA and contrary to other study findings concluded that dentures substantially increases AHI especially in supine position. They had the mean oxygen saturation percentage value of 94.2 ± 1.57, almost similar to our study findings 93.25 ± 1.31 (Table 7), which is almost nearer to the proved normal basal oxygen saturation of 95.5%. The findings may be attributed due to the recordings taken only during sleep and supine position and not compared with patients when awake. This can be attributed due to interruption of elevator muscles due to the denture wear during sleep leading to the more collapsibility of the airway thus leading to reduced oxygen saturation. The day time sleepiness measured using Epworth Sleepiness Scale score was 10.2 ± 4.4 compared to our results of 8.83 ± 1.72 (Table 6), indicating there was no EDS compared between patients with or without complete dentures. The variation between the results may be attributed to the selection of subjects with non-confirmed OSA subjects selected by us.
| Variable | Pre treatment | Post treatment | Mean of diff | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Oxy Sat | 93.3 | 1.74 | 93.2 | 1.58 | 0.1 | 0.541 |
Table7: Effect of wearing complete denture on oxygen saturation.
Our study results showed no correlation between oxygen saturation and hyoid bone distance to mandibular plane. The anteroposterior measurement of retro pharyngeal space on cephalograms at three areas of SAS, PAS and MAS, revealed only MAS significant when compared between completely edentulous patients wearing with and without complete denture.
Within the limitation of the study it is concluded that denture wearing at night in healthy completely edentulous patients will not significantly improve quality and quantity of sleep as determined by oxygen saturation levels and ESS scoring. There is no significant increase in airway space and oxygen saturation levels are not affected with the use of complete dentures during sleep. It is recommended that further studies involving large sample size with OSAS may be required to be studied to conclusively prove the hypothesis of wearing denture at night improves the air way space and reduces the symptoms of OSAS. Further studies with confirmed OSA patients and varying the prosthesis vertical dimension of occlusion and MRI study with 3D measurements may give definite insight on understanding their effect on sleep parameters and on airway changes.