Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2013) Volume 2, Issue 6
Purpose: No age-based comparative studies have investigated clinical and polysomnographic manifestations of adults with Obstructive Sleep Apnea (OSA).
Methods: Retrospective record review of 570 patients with OSA at Naval Medical Center San Diego. Patients were divided into one of four age cohorts: (1) ages 18-29 (n=209); (2) ages 30-39 (n=106); (3) ages 40-49 (n=102); and (4) ages > 50 (n=153). Group comparisons of demographics, Epworth Sleepiness Scale (ESS), Patient Sleep Questionnaire (PSQ), and polysomnography were analyzed.
Results: Patients, ages 18-29 reported more witnessed apneas, Excessive Daytime Sleepiness (EDS), and had higher respiratory related arousal indexes (p=0.018) compared to patients over 30 years old. Patients 50 years and older reported more nocturia (p=0.001), less snoring, and had higher Rapid Eye Movement (REM)-related apneas (p=0.008), and more severe oximetry desaturations than patients less than 50 years old (p=0.001 - 0.004). Age groups were similar with respect to Body Mass Index (BMI), self-reported sleep-related driving impairment, Apnea Hypopnea Index (AHI), non-REM (NREM) AHI, and total obstructive and central apneas.
Conclusions: Snoring, EDS, nocturia, arousal index, and lowest oxygen saturation most significantly differentiated OSA across different age groups of patients with OSA.
Keywords: Obstructive sleep apnea; Sleep-disordered breathing; Older adults; Young adults; Polysomnogram; Epworth sleepiness scale; Age; Apnea hypopnea index
Obstructive sleep apnea is a common condition that is under recognized and under diagnosed. It is characterized by recurrent episodes of complete or partial collapse of the upper airway during sleep and is an important cause of medical morbidity and mortality. The Wisconsin-based cohort study of state employees less than 65 years of age found a prevalence of sleep-disordered breathing in 9% of women and 24% in men [1]. Risk factors for sleep-disordered breathing include obesity, male gender, menopause, alcohol consumption, craniofacial characteristics, and endocrine disorders such as hypothyroidism and acromegaly [2]. Symptoms of Obstructive Sleep Apnea (OSA) include excessive daytime sleepiness, insomnia, morning headaches, erectile dysfunction, snoring, witnessed apneas, and nocturia [2,3]. Polysomnographic features of OSA include increased wakefulness after sleep onset, reduced stage 3 and 4 sleep, reduced REM sleep, increased respiratory arousals, central and/or obstructive apneas, arterial oxygen desaturations, and cyclic variations in heart rate [2,3]. Potential consequences of sleep-disordered breathing include decreased survival [4], cognitive impairment [5], glucose intolerance [6], motor vehicle accidents [7], arterial hypertension [8], pulmonary hypertension [9], arrhythmias [10], stroke [11], sudden cardiac death [12], and diminished quality of life [13].
Age-related differences in sleep-disordered breathing are predominantly based on studies with middle-aged and older adults with minimal studies with young adults. Data from the communitybased Sleep Heart Health Study have shown that disease prevalence increases steadily with age and reaches a plateau after the age of 60 years [14]. Similar trends with increasing age have also been noted in other cohorts in whom the prevalence of moderate to severe obstructive sleep apnea (AHI>15-20 events/h) remains relatively constant after the sixth decade of life [15]. Despite the increasing prevalence of OSA with age, this does not correlate with clinical symptoms or apnea severity [16]. In the Cardiovascular Health Study, the prevalence of reported snoring decreased with increasing age [17]. Snoring decreased from 41% in men ages 65 to 69 to 17% in those over 80. Furthermore, loud snoring, observed apneas, and daytime sleepiness in elderly subjects had no association with hypertension or cardiovascular disease prevalence. The negative correlation of snoring with advanced age and the lack of association between sleep apnea symptoms with cardiovascular disease raises the notion of whether sleep-disordered breathing in the elderly is a different disorder from that of middle age and younger adults.
In a recent study comparing the effects of age on the clinical features of OSA, elderly men had a higher percentage and duration of apneas and hypopneas [18]. It is possible there is an age-related spectrum of disease with obstructive sleep apnea with disease progression associated with advancing age. If this were the case, one would expect young adults to have more respiratory related arousals and REM related apneas and hypopneas while of this study was twofold: (1) to describe the agerelated differences in clinical characteristics and polysomnographic findings of OSA in young adults, middle age adults, and the elderly and (2) to determine whether there is an age related spectrum of disease that worsens with age.
Subjects
After approval by the Institutional Review Board, we selected the records of 570 patients evaluated by the Sleep Medicine Clinic, Naval Medical Center San Diego from 2006-2008. Patients had an overnight polysomnogram with sleep-disordered breathing defined by an apnea hypopnea index (AHI) ≥ 5 with clinical symptoms of sleep apnea. Patients with portable sleep studies were excluded. The study population had a mean age of 39 ± 13 (range 18-80), and a mean Body Mass Index (BMI) of 31 ± 6 kg/m2 (range 17-62). There were 538 (94%) males and 32 (6%) females. The mean Epworth score was 12.71 ± 5.22 and mean Apnea-Hypopnea Index (AHI) was 32 ± 27.
Procedures
All subjects completed an Epworth Sleepiness Scale (ESS), Patient Sleep Questionnaire (PSQ), and an overnight polysomnogram (PSG). Demographic data included marital status, race, age, sex, and BMI. The ESS is a self-administered questionnaire to measure daytime sleepiness. A score ≥ 10 suggests significant daytime sleepiness. The Patient Sleep Questionnaire (PSQ) asks patients to rate various sleep behaviors and quantify other behaviors. Items from the PSQ include ratings about snoring, witnessed apneas, excessive daytime sleepiness, and use of alcohol to sleep. Furthermore, patients quantify nocturia frequency, driving impairment due to sleepiness, caffeine use, tobacco use, and alcohol consumption.
Experienced technicians visually scored polysomnographic records for sleep stage and apnea events using the Natus Sleep Works software. Obstructive apneas were defined as a drop in the peak thermal sensor excursion by > 90% of baseline and duration of the event for at least 10 seconds. Hypopneas required a greater than 50% decrease in airflow for at least 10 seconds with an accompanying ≥ 4% oxygen desaturation. The AHI was calculated for each patient based on the average number of events per hour. A physician with Sleep Medicine Certification reviewed the records and scoring. Polysomnographic data analyzed included the following: total sleep time, arousal index, AHI, AHI in REM sleep, AHI in NREM sleep, total number of obstructive and central apneas, lowest desaturation, time spent below 85% oxygen saturation, and whether the overnight polysomnogram was a split-night study. For split-night studies we used the data from the diagnostic portion of the study.
Statistical analysis
Patients were divided into one of four age cohorts: (1) group 1, ages 18-29 years old (n=209); (2) group 2, ages 30-39 (n=102); (3) group 3, ages 40-49 (n=106), and (4) group 4, ages 50 and older (n=153). Group demographics were evaluated using Fisher’s exact test, and racial differences among age groups were evaluated with a chi-square test with pair-wise comparisons using the Fisher exact test with the Bonferroni critical value (significant if p ≤ 0.008). Since the data did not fit a normal distribution, age group differences were analyzed by the Kruskal-Wallis test. Significant differences between multiple age groups were analyzed by pair-wise “rank sum” tests with the Bonferroni critical value (significant if p ≤ 0.008).
Demographics
The study age groups were predominantly male (94%). The ages > 50 cohort had a greater proportion of females (13%, p<0.001) compared to other age cohorts (Table 1). There were no age group differences with respect to number of split-night studies (p=0.304). Ethnicity by age group showed p=0.002. Caucasians and African-Americans were the two most predominant ethnical groups, representing 49 & 15% of total patient populations, respectively, with an increasing prevalence of Caucasians and decreasing prevalence of African- Americans with increasing age (p<0.001). There were no other significant racial differences (Table 1). Number of non-married patients and the use of tobacco were significantly higher in the group 1. BMI was similar among all age groups (p=0.156).
| Tota lN = 570 | Group 1N = 209 | Group 2N = 102 | Group 3N =106 | Group 4N =153 | P value | |
|---|---|---|---|---|---|---|
| Females | 32 (6) | 7 (3) | 1 (1) | 4 (4) | 20 (13)* | p < 0.001 |
| Split night studies | 194 (34) | 76 (36) | 32 (31) | 29 (27) | 57 (37) | p = 0.304 |
| Married | 406 (75) | 98 (55)* | 75 (74) | 95 (90) | 138 (90) | p < 0.001 |
| Tobacco use | 188 (33) | 75 (36) | 17 (17) | 18 (17) | 19 (13) | p = 0.038 |
| White | 168 (49) | 44 (26) | 27 (45) | 27 (44) | 70 (65) | |
| Black | 55 (15) | 25 (16) | 14 (25) | 9 (15) | 7 (7) | |
| Asian/Pacific Islander | 50 (15) | 21 (16) | 6 (16) | 8 (13) | 15 (14) | |
| Other | 71 (21) | 26 (42) | 13 (13) | 17 (28) | 15 (14) |
Table 1: Demographics and Clinical Characteristics of Patients*.
ESS
Excessiveness daytime sleepiness is one of the most burdensome symptoms of sleep-disordered breathing and ESS is wildly used to assess patients’ sleepiness. The questionnaire asks the patients to rate his or her probability of falling asleep on a scale of 0 to 3 on eight different parameters. Patients, ages 30-39 and 40-49, had higher Epworth scores than patients, ages ≥ 50 (median: 14 for groups 2 & 3 and 12 for group 4, p values: group 2 v. 4, p=0.008; group 3 v. 4, p=0.005). Patients, ages 18-29 had ESS scores similar to other age groups (Table 2 and 3).
| Group 1 | Group 2 | Group 3 | Group 4 | |
|---|---|---|---|---|
| VARIABLE | Median | Median | Median | Median |
| BMI (kg/m2) | 29 (29-30) | 31 (29-32) | 29 (28-30) | 30 (29-31) |
| Epworth | 12 (11-13) | 14 (12-15) | 14 (12.4-16) | 12 (10.9-12.1) |
| Sleep Questionnaire Items | ||||
| Snoring | 5 (5) | 5 (5) | 5 (5) | 4 (4-5) |
| Apneas | 4 (4) | 4 (4) | 4 (4) | 4 (3-4) |
| Excessive daytime sleepiness | 4 (3-4) | 3 (3-4) | 3 (3-4) | 3 (3) |
| Alcohol use to sleep | 1 (1) | 1 (1) | 1 (1) | 1 (1) |
| Nocturia | 1 (1) | 1 (1) | 1 (1) | 1.5 (1.5-2) |
| Sleep related MVA’s | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Sleep related near misses | 0 (0) | 0 (0-1) | 0 (0-1) | 0 (0) |
| Coffee consumption | 0 (0) | 0 (0-1) | 1 (1-1.5) | 1.5 (1-2) |
| Tea consumption (cup/day) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Cola consumption (can/day) | 1 (0.9-1) | 1 (1) | 1 (1) | 0.5 (0-1) |
| Cigarette use (pack/day) | 0.26 (0.2-0.32) | 0.12 (0.05-0.19) | 0.14 (0.06-0.21) | 0.12 ( 0.06-0.18) |
| Alcohol use (/week) | ||||
| Polysomnogram | ||||
| AHI (events/h-1) | 21 (17-27) | 21 (16-27.4) | 21 (15-28.2) | 25 (17-28) |
| Arousal index | 22 (19-24) | 16 (14-22.4) | 16.5 (13-20) | 20 (17-22) |
| Obstructive sleep apneas | 34 (24-41) | 22.5 (12-29.4) | 21.5 (12.4-32.8) | 29 (22.9-40.1) |
| Central sleep apneas | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| NREM AHI | 20 (16-24) | 20 (14.6-26.8) | 18.5 (12-25.6) | 19 (13.8-27) |
| REM AHI | 12 (8.8-16) | 17 (11.6-24) | 22.5 (14.4-34.6) | 25 (19.9-32.1) |
| Lowest oxygen saturation | 83 (82-84) | 82 (81-83.4) | 81.5 (80-83) | 81 (80-81) |
| Time less than 85% | 0.1 (0-0.3) | 0.4 (0.16-0.97) | 0.4 (0.2-0.9) | 0.9 (0.4-1.3) |
| ETOH | 2 (1.5-3) | 1.5 (1-2) | 1 (0-1.5) | 0.2 (0-1) |
Table 2: Age Group Rank Sum Medians*.
| Kruskal Wallis*p < 0.05 | Pair-Wise Rank Sum Comparisons (Mann Whitney) *p < 0.008 | ||||||
|---|---|---|---|---|---|---|---|
| VARIABLE | 1-4 | 1,2 | 1,3 | 1,4 | 2,3 | 2,4 | 3,4 |
| BODY MASS INDEX | 0.156 | - | - | - | - | - | - |
| EPWORTH | 0.002* | 0.206 | 0.031 | 0.044 | 0.541 | 0.008* | 0.005* |
| SLEEP QUESTIONNAIRE ITEMS | |||||||
| Snoring | <0.001* | 0.107 | 0.206 | 0.001* | 0.770 | <0.001* | <0.001* |
| Apneas | 0.007* | 0.117 | 0.615 | 0.001* | 0.384 | 0.161 | 0.027 |
| Excessive daytime sleepiness | 0.001* | 0.095 | 0.153 | <0.001* | 0.725 | 0.097 | 0.023 |
| Alcohol use to sleep | 0.051 | - | - | - | - | - | - |
| Nocturia | <0.001* | 0.175 | 0.001* | <0.001* | 0.148 | <0.001* | <0.001* |
| Sleep related motor vehicle accidents | 0.528 | - | - | - | - | - | - |
| Sleep related near misses | 0.100 | - | - | - | - | - | - |
| Coffee consumption | <0.001* | <0.001* | <0.001* | <0.001* | 0.001* | <0.001* | 0.124 |
| Cola consumption | 0.004* | 0.151 | 0.982 | 0.014 | 0.200 | <0.001* | 0.022 |
| Tea consumption | 0.175 | - | - | - | - | - | - |
| Cigarette use | <0.038* | 0.841 | 0.783 | 0.003* | 0.932 | 0.060 | 0.062 |
| Alcohol use | <0.001* | 0.050 | 0.004* | <0.001* | 0.354 | 0.016 | 0.169 |
| POLYSOMNOGRAM | |||||||
| Apnea hypopnea index | 0.802 | - | - | - | - | - | - |
| Arousal Index | 0.018* | 0.021 | 0.006* | 0.238 | 0.742 | 0.172 | 0.091 |
| Obstructive sleep apneas | 0.066 | - | - | - | - | - | - |
| Central sleep apneas | 0.553 | - | - | - | - | - | - |
| NREM AHI | 0.621 | - | - | - | - | - | - |
| REM AHI | 0.008* | 0.171 | 0.009 | 0.003* | 0.221 | 0.164 | 0.943 |
| Lowest Oxygen Saturation | 0.004* | 0.272 | 0.051 | <0.001* | 0.525 | 0.054 | 0.208 |
| Time less than 85% | 0.001* | 0.030 | 0.014 | <0.001* | 0.977 | 0.177 | 0.138 |
Table 3: Age Group Differences*.
PSQ
The sleep questionnaire contained a series of questions including sleep-related habits & complaints, and social behavior. Patients, ages 18-29, 30-39, and 40-49 endorsed more snoring in comparison to patients ages ≥ 50 (Group 1 v. 4, p=0.001; Group 2 v. 4, p<0.001; Group 3 v. 4, p<0.001). Patients, ages 18-29 reported more witnessed apneas and EDS than patients ages ≥ 50 (Group 1 v. 4 apneas, p=0.001, EDS p<0.001). Patients ages ≥ 50 endorsed more nocturia than other age groups (patients, ages 30-39, p<0.001; patients, ages 40-49, p<0.001; patients, ages 18-29, p<0.001). Patients, ages 40-49 also endorsed more nocturia than young adults (p=0.001). There were no age-related differences related to driving impairment due to excessive sleepiness.
Alcohol, caffeine, and tobacco
Patients, ages 18-29 reported more alcohol and tobacco use than patients, ages ≥ 50. Patients, ages 18-29 consumed the most alcohol compared to patients, ages 40-49 (p=0.004) and patients, ages ≥ 50 (p <0.001) with a trend toward use of alcohol to sleep (p=0.051). Although the majority of patients did not smoke (77%), there was a greater prevalence of smoking among patients, ages 18-29 compared to patients, ages ≥ 50 (p=0.003), but patients, ages ≥ 50 smokers used more tobacco than patients, ages 18-29. Patients, ages 30-39, 40-49 and ≥ 50 consumed more caffeinated beverages than patients, ages 18-29. Patients, ages 40-49 and ages ≥ 50 consumed more coffee than patients, ages 18-29 and 30-39. Patients, ages 30-39 consumed more coffee than patients, ages 18-29 (p<0.001). Patients, ages 30-39 reported more cola beverage consumption than patients, ages ≥ 50 (p<0.001).
Polysomnography
Arousal is an intrusion or disturbance in the patients’ sleep pattern as measured by EEG brain wave activity. The arousal index is the average number of arousals per hour, regardless of the source of those arousals. In our study the arousal index was higher in patients, ages 18-29 compared to patients, ages 40-49 (p=0.006). Compared to patients, ages 18-29, patients, ages ≥ 50 had lower oxygen desaturations (p=0.003), more prolonged oxygen desaturations greater than 85% (p<0.001), and higher REM AHI’s (p<0.001). There were no significant age-related differences with respect to AHI, total number of obstructive and central apneas, and NREM AHI.
Combined sleep-related parameters in function of age
A multiple linear regression analysis was conducted for different sleep-related parameters against OSA patients’ ages. The plot of snoring, EDS, nocturia, arousal index, and lowest oxygen saturation against age had all individually significant p value (p<0.01). When these sleep-related parameters were used in combination (Combined Sleep-Related Parameters or CSRP) and a multiple linear regression statistic analysis was performed against patients’ ages , an even stronger linear relationship was established, exhibiting a highly significant F-test of the overall fit p value < 0.00001, and a goodness of fit R-squared= 0.15 (Figure 1).
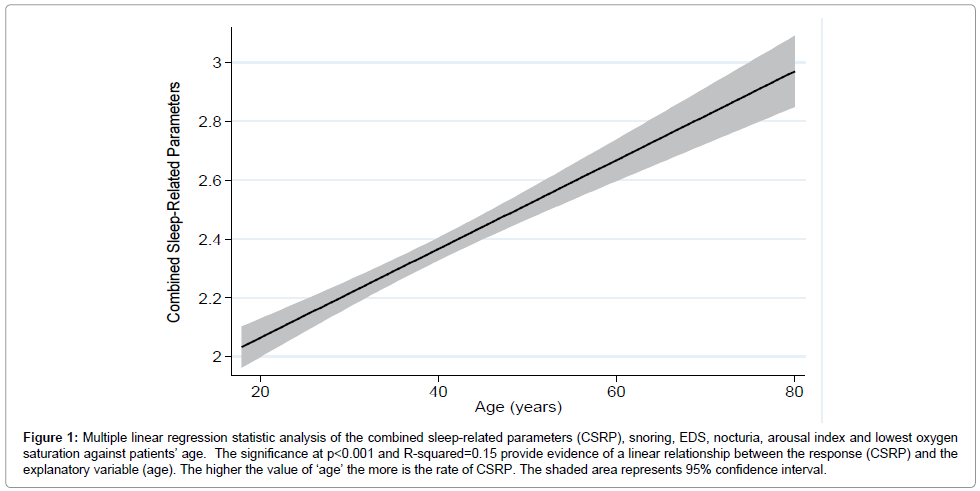
Figure 1: Multiple linear regression statistic analysis of the combined sleep-related parameters (CSRP), snoring, EDS, nocturia, arousal index and lowest oxygen saturation against patients’ age. The significance at p< 0.001 and R-squared=0.15 provide evidence of a linear relationship between the response (CSRP) and the explanatory variable (age). The higher the value of ‘age’ the more is the rate of CSRP. The shaded area represents 95% confidence interval.
Our study demonstrated an increased arousal index in patients, ages 18-29 compared to patients, ages ≥ 50, however, in the latter there was an increase in REM-related apneas and hypopneas as well as more severe desaturations despite similar AHI’s. Our study suggests that the greatest differences in clinical symptoms and polysomnographic findings between patients, ages 18-29 and patients, ages ≥ 50 with OSA were not accounted for by BMI. Patients, ages 18-29 report many of the common symptoms associated with OSA such as snoring, witnessed apneas, and excessive daytime sleepiness. Patients, ages ≥ 50 report less snoring, less witnessed apneas, and less daytime sleepiness than patients, ages 18-29.Our study suggests that snoring, witnessed apneas, and obesity are insensitive indicators for identifying OSA in patients, ages ≥ 50. Data from the Sleep Heart Health Study on people ages 40 to 98 years demonstrated that male sex, BMI, neck size, snoring, and witnessed apneas were associated with OSA, but in older adults the magnitude of associations between OSA, body habitus, snoring and witnessed apneas decreased similar to our findings [19]. As a result, health care practitioners may not recognize OSA in older adults, and older adults may ascribe symptoms of OSA to aging, medications, or other medical problems. Maintaining a high index of suspicion and obtaining a complete medical history are valuable assets in assessing for OSA in the elderly.
Patients, ages ≥ 50 report more nocturia compared to the patients, ages 18-29. Nocturia has been previously reported as a common complaint in older adults and associated with increased falls and fractures [20,21]. A cross-sectional study investigating OSA in community-dwelling older adults demonstrated more nocturia with an AHI of 25 or greater [22]. The increased nocturia in the elderly and late middle age patients may be due to diuretic medications, increased intraabdominal pressure, confusion associated with arousals, and increased secretion of Atrial Natriuretic Peptide (ANP). Increased plasma and urine ANP result in increased natriuresis and dieresis [23]. The increased ANP levels in patients with severe sleep apnea are attributed to hemodynamic changes associated with sleep apnea to include atrial distension, acute hypoxemia, and pulmonary hypertension [24-26].
A greater proportion of patients, ages 18-29 reported alcohol and tobacco consumption compared to older age groups. The increased use of tobacco and alcohol consumption among patients, ages 18-29 may worsen sleep apnea severity in young adults. One epidemiologic study that focused on smoking found that current smokers were three times (95% CI, 1.4 to 6.4) more likely to have OSA than never-smokers [27]. There are several mechanisms to explain the link between smoking and OSA. Smoking can induce upper airway edema and increase sleep instability. Upper airway inflammation and edema may increase vulnerability to OSA. Sleep instability is associated with OSA and may be increased by reductions in blood nicotine levels. Nicotine may also cause a “rebound effect” where acutely nicotine increases upper airway tone that is reversed overnight with withdrawal of nicotine resulting in worsening OSA [27].
Many studies in which defined quantities of alcohol were administered to healthy subjects or patients with OSA before bedtime demonstrated increased number and duration of hypopnea and apnea events [28,29]. In one CPAP-titration experiment moderate alcohol consumption near bedtime increased the level of nasal pressure necessary to prevent apneas and hypopneas in patients with OSA [28]. Alcohol ingestion can inhibit the activity of upper airway muscles and increase airway collapsibility resulting in increased nasal and pharyngeal resistance. In addition, alcohol can diminish arousal responses resulting in prolonged apnea duration and worsening oxygen desaturation.
Although there was no difference in AHI between age cohorts, patients, ages ≥ 50 had more severe oxygen desaturations and an increased REM-related AHI while patients, ages 18-29 had an increased arousal index. The severe desaturation and high REM AHI in the elderly may be due to disease progression associated with age. The proposed mechanism may be increased deposition of parapharyngeal fat, lengthening of the soft palate, and changes in body structures surrounding the pharynx [27,28]. Respiratory related arousals are associated with Upper Airway Resistance Syndrome (UARS), and mild to severe OSA [29]. Frequent respiratory arousals disrupt sleep architecture and may account for the higher ratings of excessive daytime sleepiness on the PSQ.
Our study failed to demonstrate an increase in REM related apneas and hypopneas and a decrease in NREM-related apneas and hypopneas in patients, ages 18-29 compared to patients, ages > 50. Our hypothesis was that sleep apnea has a continuum of disease severity that can be identified by examining age cohorts. Early manifestations of OSA in young patients would manifest with high arousals and REM predominant apneas and hypopneas while late manifestations of OSA would have predominantly NREM apneas and hypopneas. One explanation is that a number of patients, ages 18-29 already had moderate to severe apnea accounting for the REM and NREM apnea events. Another hypothesis is that apnea severity does not correlate with the proportion of REM vs. NREM apneas and hypopneas. A retrospective study examining the differences between patients with REM AHI vs. NREM AHI found that BMI, apnea severity, and severity of oxygen desaturation did not account for group differences. Only the duration of apnea was longer in the REM AHI group [30].
Our study has several limitations. First, the mean AHI was high which may have resulted in comparing age groups with severe OSA under representing adults with mild OSA, which may have better identified a spectrum of OSA. The study was also retrospective and patients were not randomized to the different age groups. Furthermore, investigators were not blinded when selecting patients for the different age cohorts and this could be perceived as a source of selection bias. A randomized double blind, prospective study with different age groups may have provided different data. Split-night studies compared to full-night diagnostic studies would potentially have shorter total sleep times that may alter sleep parameters; however, the number of split-night studies were similar between groups. There was also a significant proportion of male patients whose race was unknown as the information was either not available in the patient’s electronic medical record or the patient’s race was identified as “other.” Finally, the findings may not apply to women as they were underrepresented in this study.
There were a greater percentage of women represented in the age ≥ 50 group which is consistent with epidemiological data which supports the higher prevalence of obstructive sleep apnea in postmenopausal women compared to premenopausal women [30]. The greater percentage of women in the older age group may have affected our results. With regards to the severity of sleep apnea among the younger age group, the main reasons young adults are referred for evaluation of sleep disordered breathing is due to occupational impairment due to daytime sleepiness or reports by roommates or spouses other of snoring and witnessed apneas. Young adults have similar risk factors for obstructive sleep apnea in comparison to older adults and therefore do not differ in apnea severity.
In conclusion, this study evaluated different sleep related parameters for patients with OSA at different age ranges. Patients, ages 18-29 had the largest differences in clinical and polysomnographic manifestations of OSA compared to patients, ages ≥ 50. Patients, ages 18-29 reported symptoms commonly associated with OSA and had higher arousal indexes. In contrast, patients, ages ≥ 50 reported more nocturia, less snoring, less witnessed apneas, and less daytime sleepiness and had an increased REM AHI with more severe oxygen desaturations.