Medicinal & Aromatic Plants
Open Access
ISSN: 2167-0412
ISSN: 2167-0412
Research Article - (2015) Volume 4, Issue 2
Health issues related to bacterial infections, and the rise of bacterial resistance, have pushed the need for improved control options. Recently there has been a renewed interest in testing essential oils as antimicrobials, and combinatorial therapy combining conventional antibiotics and essential oils is ongoing. The popularity of essential oils as homeopathic remedies has increased in recent years due to the thought that natural products might prove safer than ingredients currently in consumer products. Several scientific reports exist relating to the efficacy of essential oils in controlling microbes, however most of these publications are either microbe centric, or are specific to one particular essential oil or oil constituent. This work was undertaken to develop a more comprehensive picture of the antibacterial effects of essential oils by evaluating the effectiveness of a large panel of essential oils against four diverse strains of bacteria (Escherichia coli, Staphylococcus aureus, Micrococcus luteus, and Serratia marcescens). Of the essential oils tested, cinnamon bark, lemongrass, oregano, and thyme oils were the most potent, and had activity comparable to a concentration of a penicillin-streptomycin solution commonly used to inhibit bacterial growth. This study supports the idea that certain essential oils could play an important role in the development of antimicrobial products.
Keywords: Essential oils; Antimicrobial; Natural products; In vitro; Serogroups
Essential oils (EOs) are natural aromatic compounds isolated from plants. Oil is “essential” in the sense that it contains the “essence of” the plant’s fragrance. These complex mixtures have been used medicinally throughout history for a wide range of purposes. Recently, interest in essential oils has been revived as a natural alternative to conventional treatments and therapeutic practices. One area of study involves the use of EOs to combat microbes. Suggested applications for the use of antimicrobial oils span multiple microbes, such as viruses, fungi, and bacteria, and extend into many industries, from agricultural, to hospitals, to home use. There are many possible advantages of using natural products as antimicrobial compounds, such as fewer adverse effects, better patient tolerance, relatively inexpensive, renewability and biodegradability. As harmful bacterial strains in homes and hospitals become increasingly resistant to conventional antibiotics and antibacterial agents in consumer products, better and alternative products will certainly be needed.
There are several reports in the public domain relating to the efficacy of EOs in controlling microbes, however most of these reports focus on the chemical composition and in vitro activities of a particular singular EO, or a particular constituent of an EO. Furthermore, many studies will indicate how a particular EO used in the study was extracted or manipulated, but this information may not be readily applicable to the general public, as consumer perception and demand encourages public retailers to sell oils of high purity in the most natural composition possible. Other studies in the literature take the approach of focusing on one particular micro-organism, and examine the effect from a small panel of EOs, thus leaving the broad applicability of particular oil against multiple strains in question. Therefore, this work was undertaken to develop a more comprehensive picture of the antibacterial effects of EOs. In this study the antibacterial properties of a sizable library of 31 EOs obtained through a consumer retail source was evaluated against 4 diverse strains of bacteria (Escherichia coli, Staphylococcus aureus, Micrococcus luteus, and Serratia marcescens). Escherichia coli are a Gram-negative rod-shaped bacterium consisting of mostly harmless substrains found in the lower intestine of warmblooded organisms. However, some serogroups can cause serious food poisoning, and are occasionally responsible for product recalls due to contamination [1]. Staphylococcus aureus is a Gram-positive bacterium that is a common cause of skin infections and food poisoning. The emergence of methicillin-resistant Staphylococcus aureus (MRSA) is a worldwide problem in clinical medicine [2]. Serratia marcescens is a species of rod-shaped Gram-negative bacteria involved in hospitalacquired infections, particularly catheter-associated bacteremia, urinary tract infections, and wound infections [3]. Micrococcus luteus is a Gram-variable, nonmotile, bacterium nearly ubiquitous in our environment, and part of the normal flora of the mammalian skin. However, M. Luteus is considered a resilient contaminant in hospital patients [4].
Essential oils
Thirty one essential oils (peppermint (Mentha piperita), bergamot (Citrus Bergama), wintergreen (Gaultheria procumbens), grapefruit (Citrus x parasisi), basil (Ocimum basilisum), rosemary (Rosmarinus officinalis CT cineol), orange (Citrus sinensis), melaleuca (Melaleuca alternifolia), clove (Syzygium aromaticum), lemon (Citrus limon), balsam fir (Abies balsamea), birch (Betula alba), chamomile (Chamaemelum nobile), cinnamon (Cinnamomum verum), cypress (Cupressus sempervirens), eucalyptus globulus (Eucalyptus globulus), eucalyptus radiate (Eucalyptus radiate), frankincense (Boswellia carteri), ginger (Zingiber officinale), helichrysum (Helichrysum italicum), lavender (Lavandula angustifolia), lemongrass (Cymbopogon flexuosus), marjoram (Origanum majorana), myrtle (Myrtus communis), oregano (Origanum compactum), sandalwood (Santalum album), spruce (Picea mariani), tangerine (Citrus reticulate), thyme (Thymus vulgaris), vetiver (Vetiveria zizanoides), ylang ylang (Cananga odoratac)) were procured through Améo (Lehi, UT, USA).
Bacterial strains and culture conditions
Escherichia coli (ATCC® 25922™), Staphylococcus aureus subsp. aureus Rosenbach (ATCC® 25923™), Micrococcus luteus (Schroeter) Cohn (ATCC® 49732™), and Serratia marcenscens subsp. marcescens Bizio (ATCC® 13880™) strains were purchased through ATCC (Manassas, VA).
Disk diffusion assay
Antimicrobial activity was investigated by the disc diffusion method. Briefly, an overnight culture of bacteria was adjusted to a density of OD600=0.2. Then 100 μL of bacteria was added to a 100 mm tryptic soy agar plate and spread out using an L spreader to create a uniform layer of bacteria. 20 μL of each EO was applied on a sterile paper disc aseptically placed on the inoculated plates. After 24 h of incubation at the recommended temperature in an incubator, the inhibition zones were measured in millimeters. A Penicillin/Streptomycin solution (Gibco, Cat No. 15140) was used as a positive control for bacterial inhibition. Purell Brand® Advanced Hand Sanitizer (active ingredient: Ethyl Alcohol, 70% v/v) and 70% isopropanol were also included as controls. All experiments were done in triplicate unless otherwise noted. The average of inhibition diameters was calculated to classify the EOs as follows: (0)=not sensitive, for a diameter smaller than 8 mm; (+)=moderately sensitive, for a diameter of 8-14 mm; (++)=sensitive, for a diameter of 14-20 mm; and (+++)=very sensitive, for a diameter larger than 20 mm.
Determination of minimum inhibitory concentration
Essential oils with a large inhibition diameter (>20 mm) were examined for their antimicrobial activity against E. coli and S. aureus. The Minimum Inhibitory Concentration (MIC) was estimated by the broth dilution method. Briefly, a 1:200 dilution of overnight culture was plated onto a clear 96-well plate. Each EO was first diluted in tryptic soy both, and half-log dilutions of EOs were carried out in broth with concentrations calculated to give final concentrations ranging from 1% (v/v) to 0.001% (v/v). After 24 h of incubation at 37°C MIC was determined as the lowest concentration of the EO inhibiting visible bacterial growth.
The disk diffusion test was used to evaluate the antibacterial properties of 31 EOs. This method uses antibiotic-impregnated wafers to test whether bacteria are affected by particular agents. In this case, wafers containing essential oils were placed on nutrient rich agar plates recently inoculated with bacteria. If the essential oil stops the bacteria from growing or kills the bacteria, there will be a clear area around the wafer where the bacteria did not grown enough to be visible. This is called a zone of inhibition. A stronger antibacterial should create a larger zone, because a lower concentration of that agent is enough to stop growth. Based on the initial screening of oils, 13 oils showed activity against each of the 4 strains tested. Representative pictorial examples of the bacterial inhibition observed are presented in Figure 1, whereas a complete summary of this initial screen is included in Table 1. The five EOs exhibiting the most potent activity were lemongrass, thyme, cinnamon, oregano, and clove. To further compare and contrast the potency of these oils, the disk diffusion assay was performed again using oils diluted 1:10 in water and evaluated alongside commercial antibiotics (Table 2). Solutions containing 10% oil exhibited similar activity to a 10x (1,000 units/mL penicillin, 1,000 mg/mL) penicillin/ streptomycin solution when tested against and S. aureus (representative replicate shown in Figure 2) and E. coli (numerical results only; Table 2). The 1x (100 units/mL penicillin, 100 mg/mL streptomycin) penicillin/streptomycin solution is the concentration recommended by the manufacturer for inhibition of bacterial contamination, however, under a high bacterial load a 10x solution was needed to generate a modest zone of inhibition for comparison. The 5 most potent oils were similar in their effectiveness, however, cinnamon oil proved most effective against both S. aureus and E. coli when 10% solutions were compared. When tested at a lower concentration of 5%, the activity was absent, expect for minimal activity by oregano, lemongrass, and clove oil in E. coli.
| Essential Oil | E. coli | S. aureus | M. leteus | S. marcescens |
|---|---|---|---|---|
| Balsam fir | 0 | 0 | 0 | 0 |
| Basil | 0 | + | +++ | 0 |
| Bergamot | + | + | + | ++ |
| Birch | + | + | 0 | + |
| Chamomile Roman | 0 | + | + | 0 |
| Cinnamon Bark | +++ | +++ | +++ | +++ |
| Clove | +++ | ++ | +++ | +++ |
| Cypress | 0 | + | 0 | + |
| Eucalyptus Globulus | + | + | 0 | + |
| Eucalyptus Radiata | 0 | + | ++ | 0 |
| Frankencense | 0 | ++ | 0 | 0 |
| Ginger | + | + | +++ | ++ |
| Grapefruit | 0 | + | 0 | 0 |
| Helichrysum | + | + | + | ++ |
| Lavender | + | + | ++ | + |
| Lemon | 0 | + | 0 | 0 |
| Lemongrass | +++ | +++ | +++ | +++ |
| Marjoram | ++ | ++ | ++ | +++ |
| Melaleuca | 44 | + | 44 | +++ |
| Myrtle | 0 | + | 0 | 0 |
| Orange | 0 | + | 0 | 0 |
| Oregano | +++ | +++ | +++ | +++ |
| Peppermint | + | ++ | +++ | + |
| Rosemary | 0 | ++ | +++ | 0 |
| Sandalwood | 0 | + | ++ | 0 |
| Spruce | 0 | + | 0 | 0 |
| Tangerine | 0 | 0 | 0 | 0 |
| Thyme | +++ | +++ | +++ | +++ |
| Vetiver | 0 | + | +++ | 0 |
| Wintergreen | + | + | +++ | + |
| Ylangylang | 0 | + | ++ | 0 |
Table 1: Bacterial sensitivity to essential oils.
| Zone of inhibition | Activity relative to commercial hand sanatizer | |||
|---|---|---|---|---|
| E. coli (mm) | S. aureus (mm) | E. coli | S. aureus | |
| 70% isopropanol | 10.2 | 9.2 | 138% | 138% |
| Hand sanitizer, 63% alcohol | 7.3 | 6.7 | 100% | 100% |
| Pen/Strep 10x (1,000 u/mL; 1,000 mg/mL) | 14.4 | 23.0 | 196% | 345% |
| Lemongrass 10% | 9.1 | 6.0 | 124% | 90% |
| Thyme 10% | 14.3 | 11.8 | 195% | 177% |
| Cinnamon 10% | 16.3 | 17.8 | 222% | 267% |
| Oregano 10% | 13.4 | 10.1 | 182% | 152% |
| Clove 10% | 9.9 | 6.4 | 135% | 96% |
| Lemongrass 5% | 5.0 | 0.0 | 68% | 0% |
| Thyme 5% | 0.0 | 0.0 | 0% | 0% |
| Cinnamon 5% | 0.0 | 0.0 | 0% | 0% |
| Oregano 5% | 9.0 | 0.0 | 123% | 0% |
| Clove 5% | 4.5 | 0.0 | 61% | 0% |
| *n=5 | ||||
Table 2: Activity of five most potent oils.
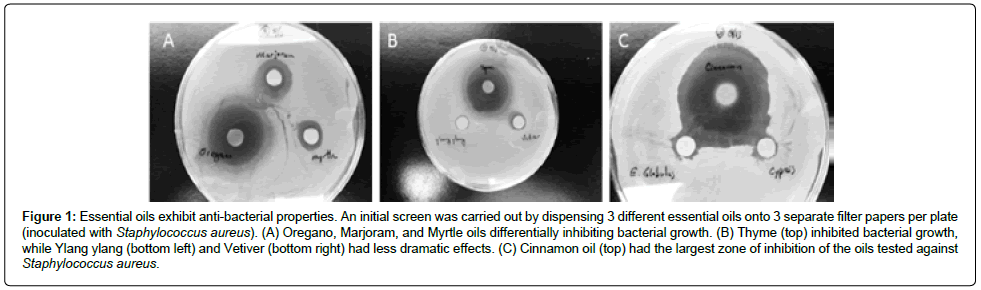
Figure 1: Essential oils exhibit anti-bacterial properties. An initial screen was carried out by dispensing 3 different essential oils onto 3 separate filter papers per plate (inoculated with Staphylococcus aureus). (A) Oregano, Marjoram, and Myrtle oils differentially inhibiting bacterial growth. (B) Thyme (top) inhibited bacterial growth, while Ylang ylang (bottom left) and Vetiver (bottom right) had less dramatic effects. (C) Cinnamon oil (top) had the largest zone of inhibition of the oils tested against Staphylococcus aureus.
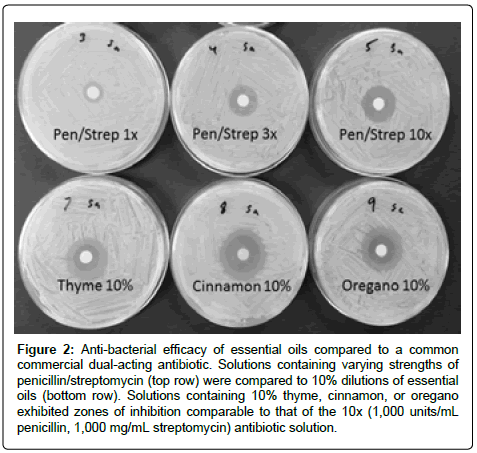
Figure 2: Anti-bacterial efficacy of essential oils compared to a common commercial dual-acting antibiotic. Solutions containing varying strengths of penicillin/streptomycin (top row) were compared to 10% dilutions of essential oils (bottom row). Solutions containing 10% thyme, cinnamon, or oregano exhibited zones of inhibition comparable to that of the 10x (1,000 units/mL penicillin, 1,000 mg/mL streptomycin) antibiotic solution.
The Minimum inhibitory concentrations (MIC) are the lowest concentration of an antimicrobial agent that will inhibit the visible growth of a microorganism in an overnight liquid culture. MICs were determined for lemongrass, thyme, cinnamon, oregano, and clove against E. coli and S. aureus (Table 3). Against E. coli, thyme and oregano had an MIC of 0.1% oil, while the other oils were about a half log less potent. Thyme and cinnamon were more potent against S. aureus, having an MIC of 0.03% oil, with the other oils being a half log to a log less potent.
 |
Table 3: Minimum inhibitory concentrations of 5 essential oils.
This work was undertaken to investigate a comprehensive array of EOs against multiple bacterial strains. The ability to directly assess relative antibacterial activity of such a large set of EOs makes this study unique compared to that which has been previously published. Of the 31 EOs evaluated herein, several exhibited antibacterial properties, however lemongrass, thyme, cinnamon, and oregano, stood out as being the most active. In contrast, balsam fir, grapefruit, lemon, myrtle, orange, spruce, and tangerine showed little to no activity against the strains of bacteria tested. Therefore the majority of oils that did not appear to have antibacterial properties were citrus oils and those from coniferous trees. Citrus oils contain limonene as their major constituent, and although web searches for antibacterial activity of limonene will produce positive hits, the results in this study support conclusions found elsewhere that limonene is among the poorer essential oil constituents with respect to antibacterial activity [5,6].
Interestingly, some of the EOs showed selectivity for particular types of bacteria. For example, S. aureus was more susceptible in general to EOs in comparison to E. coli, however, melaleuca and clove oils reversed the trend and had more activity against E. coli than S. aureus. These types of differences might hold clues to the mechanism of action for these oils, and might prove important in tailoring specific oils to specific bacteria.
Lemongrass is composed primarily of the monoterpene citral (65-85%), and citral has been reported to have antimicrobial effects, especially against MRSA methicillin resistant Staphylococcus aureus, where it was found to have similar activity as currents drugs like ampicillin [7]. Furthermore, high citral content is desirable in lemongrass oil, and has been the focus of studies to determine optimal plant harvesting times to obtain high citral levels [8]. The lot of oil that was tested in the present study had a citral content of nearly 80%, with the closely related compound geraniol as the next major constituent (GC-MS integration values not shown). Other reports suggest that geraniol by itself also has antibacterial properties [9].
It is well known that thyme oil exhibits antimicrobial properties. One comprehensive report states that thyme oil has potent activity against 120 clinically relevant strains of bacteria, and more importantly, has activity against antibiotic resistant strains as well [10]. Thymol is the major constituent of Thyme oil, and thymol by itself has shown good activity against E. coli, and is thought to work by permeabilizing and depolarizing the bacterial membrane [11]. GC-MS quality control analysis of the thyme oil used in this study was composed of two major constituents; those being thymol, at about 50% of the oil, followed by p-Cymene, at nearly 30% (GC-MS integration values not shown). Interestingly, it has been reported that these two compounds work synergistically to control the growth of Bacillus cereus [12].
Oregano is most known and studied for its potential antioxidant activities, but is has also been identified as having antimicrobial properties [13,14]. The major constituents of oregano oil are carvacrol, thymol, and p-cymene. However the ratios of these constituents can vary widely depending upon extraction method and plant growth conditions [15,16]. GC-MS quantification of the particular oil used in this study showed 77% carvacrol, 10% p-Cymene, and 7% thymol (GCMS integration values not shown).
There are other published works in the literature consisting of a similar theme of testing a subset of EOs against a subset of bacterial species. It would be appropriate to compare and contrast the results of those studies that overlap in some ways. Prabuseenivasan et al. conducted a study with a library of 21 EOs (12 overlapping with the current study) tested against 6 strains of bacteria (2 strains overlapping with the current study) [17]. In agreement with the present work, it was concluded that cinnamon oil exhibited the best broad spectrum antibacterial activity. Interestingly, Prabuseenivasan et al. observed activity against E. coli and S. aureus with orange and lemon EOs, whereas our results did not support this conclusion. Additionally we observed activity with EO from eucalyptus globulus, yet their work indicated no activity. The activity indicated for clove, lavender, lemongrass, peppermint, rosemary, basil, vetiver, and wintergreen were similar to the findings of the current study. In a separate study, Inouye et al. examined the antibacterial activity by gaseous contact of 14 EOs (8 overlapping with the current study) against 6 bacterial strains (2 strains overlapping with the current study) [5]. It was observed that cinnamon bark, lemongrass, and thyme had the most potent activity overall. When looking specifically at S. aureus and E. coli, cinnamon bark and thyme exhibited identical activity, with melaleuca and lemongrass also exhibiting strong activity. These reports combined with the data presented herein show that cinnamon EO consistently performs well as an antibacterial. Like previously discussed for thymol, cinnamon oil is thought to have a membrane disrupting mechanism of action against bacteria. Yap et al. found that cinnamon bark oil disrupts the bacterial cell membrane of E. coli, and is very potent against resistant strains of E. coli [18]. Cinnamon oil is comprised mostly of cinnamaldehyde, and GC-MS of the oil used in this study contained 75% cinnamaldehyde (GC-MS integration values not shown).
The results herein suggest that EOs exhibit a wide range of antibacterial activity. Of the 31 oils tested, 13 had at least some activity against all 4 different strains of bacteria tested in the disk diffusion method. Of the remaining 18 EOs, only 2 EOs exhibited no activity against any of the bacteria tested. Lemongrass, thyme, cinnamon, clove, and oregano oils were found to be the most potent relative to the other EOs, and further evaluation of these 5 oils as 10% solutions provided equivalent or better activity than that of an equal volume of commercial hand sanitizer or isopropyl alcohol. Evidence for the usefulness of essential oils in combating undesirable bacteria continues to build, and further research and development of these oils in consumer products is warranted.
Joshua Plant is employed by the supplier of the essential oils, Zija Corp. No other conflicts of interest are declared regarding the publication of this paper.