Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
Research Article - (2018) Volume 7, Issue 1
Background: Multiple sclerosis (MS) is a multi-component disease characterized by inflammation, neurodegeneration and failure of central nervous system (CNS) repair mechanisms. Autoimmune thyroid disease is a frequently studied disorder in MS, most studies have focused primarily on the increased prevalence of thyroid dysfunction and anti-thyroid antibodies (ATAs) in MS patients compared with a control population.
Objectives: To investigate the effect of treatment with interferon beta on thyroid functions and autoimmune thyroid markers in patients with multiple sclerosis.
Subjects and Methods: This prospective study was conducted on 100 subjects recruited from the inpatient and outpatient clinic of Internal Medicine department and Neurology Unit of Ain Shams University Hospitals. They were divided into group 1, which included 50 patients newly diagnosed with multiple sclerosis according to Macdonald’s criteria 2010 and group 2, which included 50, age and sex matched healthy volunteers. All participants were exposed before and 6 months after treatment with interferon beta to Expanded disability status scale (EDSS), which is a method of quantifying disability in multiple sclerosis, Free T4, Free T3 and TSH, Anti thyroid peroxidase (anti- TPO) and anti-thyroglobulin (anti TG) antibodies, MRI brain and neck ultrasonography.
Results: Anti thyroid peroxidase antibody levels were significantly higher in the drug naïve patients group after treatment with interferon beta (29.660 ± 28.755 IU/ml) in comparison to their baseline values (17.580 ± 4.982 IU/ml) (p-value=0.004). Anti-thyroglobulin antibody levels were significantly higher too after treatment with interferon beta (33.920 ± 32.553 IU/ml) in comparison to baseline values (24.560 ± 20.101 IU/ml) (p- value=0.01).
Conclusion: IFN-β therapy has a strong impact on the auto-immune thyroid markers status and levels in drug naïve MS patients causing increase in both anti TPO and anti TG positivity statues and numerical values.
Keywords: Thyroid auto-immunity; Multiple sclerosis; Interferon beta
Multiple sclerosis (MS) is a multi-component disease characterized by inflammation, neuro-degeneration and failure of central nervous system (CNS) repair mechanisms. Immune dys-regulation appears to originate with dendritic cells (antigen-presenting cells) which have an activated phenotype in individuals with MS. Dendritic cells migrate across the blood-brain barrier and induce differentiation of memory T cells into pro-inflammatory T helper 1 (Th1) and Th17 lymphocytes. In turn, induction of macrophage and microglial activation produces other pro-inflammatory cytokines and oxygen and nitric oxide radicals responsible for the demyelination and axonal loss [1].
The co-occurrence of autoimmune disease has thus been of substantial interest, as associations between MS and other autoimmune diseases may highlight common genetic or environmental exposures. Further, as new therapies emerge that raise the risk of autoimmune diseases such as thyroid disease and idiopathic thrombocytopenic purpura it has become increasingly important to understand the incidence of these conditions in the MS population [2].
Autoimmune thyroid disease is a frequently studied disorder in MS, most studies have focused primarily on the increased prevalence of thyroid dysfunction and anti-thyroid antibodies (ATAs) in MS patients compared with a control population. However, whether the frequency of thyroid disease in individuals with MS and their families is increased is controversial [3].
The cytokine IFN-β is a key molecule in multiple sclerosis, as it maintains the anti-inflammatory status of the immune system and is one of the most widely used treatments for MS patients. The biological activity of IFN-β is mediated through interaction with the IFN α/β cell surface receptor [4].
Since IFN-β, modulates the immune-regulatory system, it may precipitate autoimmune disorders. IFN-β therapy has been associated with a relatively high risk of developing thyroid disease, as either organ dysfunction or autoimmunity. Interferon induced thyroiditis can manifest as clinical autoimmune thyroiditis, presenting with symptoms of classical Hashimoto’s thyroiditis or Graves’ disease, or as non-autoimmune thyroiditis. Non-autoimmune thyroiditis can manifest as destructive thyroiditis, with early thyrotoxicosis and later hypothyroidism, or as non-autoimmune hypothyroidism. It is believed that IFN induces thyroiditis by both immune stimulatory effects and by direct effects on the thyroid [5].
Study participants
This study is a prospective study that was conducted on 100 subjects their age ranging from 20-50 years old, recruited from the inpatient and outpatient clinic of Internal Medicine department, Neurology Unit of Ain Shams University Hospitals during the period from February 2016 to August 2017. They were divided into group 1, which included 50 drug naïve patients of both sex diagnosed with multiple sclerosis according to Macdonald’s criteria 2010, their age ranging from 20-50 years old and group 2, which included 50 healthy age and sex matched individuals as a control.
All persons including the control group and MS patients were subjected to full medical history taking, thorough clinical examination (emphasizing on thyroid examination and neurological examination) and autoimmune manifestations as Vitiligo and arthritis, expanded disability status scale (EDSS), it quantifies disability in eight Functional System (FS) and allows neurologists to assign a Functional System Score (FSS) in each of these. The functional symptoms are pyramidal, cerebellar, brainstem, bowel and bladder, visual and cerebral. EDSS steps 1.0 to 4.5 refer to people with MS who are fully ambulatory, EDSS steps 5.0 to 9.5 are defined by the impairment to ambulation. Laboratory investigations included Basal serum Free T4, Free T3 and TSH measured by ELISA, Anti TPO antibodies, Anti-thyroglobulin antibodies and radiological investigations as MRI brain and neck ultrasonography.
Medical consent informed consents were taken from all patients and controls. Ethical approval was obtained from Ain Shams University, Faculty of Medicine, research Ethics Committee FWA000017585.
Exclusions criteria were history of any thyroid diseases (autoimmune thyroid diseases, thyroid tumors and thyroiditis), family history of thyroid diseases, history of previous thyroid operation or radioactive iodine, history of previous prolonged exposure to radiations, being on drugs altering thyroid function such as amiodarone, immune modulators used in infectious, inflammatory and neoplastic conditions and lithium, history of other autoimmune disorder as systemic lupus erythromatosis, rheumatoid arthritis, other neurological concomitant disease or contraindications to do MRI brain, history of interferon therapy, pregnancy and EDSS>6.
Methods
8 ml of venous blood was collected by venipuncture. 4 ml of the sample was used for measurement of free T3, T4 and TSH and the other 4 ml was used for measurement of serum anti TPO antibodies and anti-thyroglobulin antibodies then serum was separated by centrifugation. It was frozen at -20°C until assayed. Assay of serum free T3, T4, TSH, anti TPO antibodies and serum anti-thyroglobulin antibodies by ELISA [6-8]. Sonographic examination of the thyroid gland was performed with a 7.5-MHz transducer [9].
Statistical methods
The data was collected, revised, verified and analyzed statistically using SPSS (Statistical Package for the Social Sciences) version 18. Description of parametric data done using mean ± standard deviation (mean ± SD). Mean (average): sum off all variables divided by total numbers of variables. Standard deviation (SD): the positive square root of variance. Comparative analysis of quantitative data was done using student t-test. Correlations were done using Pearson correlation coefficient and then multi-variant regression was done between all significant correlations with anti TPO and anti TG (Pearson correlation co- efficient (r)). Graphical expression of significant correlation was done using scatter plot diagrams (is a type of mathematical diagram using Cartesian coordinates to display values for two variables for a set of data). The significance of the test was determined according to the P value to be: Non-significant (NS) if P>0.05. Significant (Sig) if P<0.05. Highly significant (HS) if P<0.001.
We found that in group I that included 50 patients (37 females and 13 males with drug naïve multiple sclerosis newly diagnosed by Macdonald’s criteria), their mean age was 30.00 ± 7.725 years.
Their mean duration from the first attack was 2.729 ± 1.244 years. Their mean free T4 was 1.087 ± 0.737 ng/dl, and mean free T3 was 3.142 ± 0.419 pg/dl. Their mean TSH level was 1.661 ± 1.125μIU/ml, mean EDSS was 2.850 ± 1.546. Anti TPO antibodies were negative in all patients with a mean level of 17.580 ± 4.982 IU/ml.
Anti TG antibodies were negative in 35 patients and positive in 15 patients with a mean level of 24.560 ± 20.101 IU/ml. Neck U/S findings before treatment were normal in all patients. While in group II that included 50 normal healthy volunteers (31 females and 19 males), their mean age was 31.340 ± 5.061 years. Their mean free T4 was 1.064 ± 0.134 ng/dl and mean free T3 was 3.119 ± 0.340 pg/dl. Their mean TSH level was 2.587 ± 0.769 μIU/ml. Anti TPO antibodies were negative in all volunteers with a mean level of 17.040 ± 5.890 IU/ml. Anti TG antibodies were negative in all volunteers with a mean level of 14.800 ± 2.449 IU/ml (Table 1).
| Groups | T-Test | ||||
|---|---|---|---|---|---|
| Patients ( before ttt) | Control | t | P-value | ||
| Age (years) | Range | 17-50 | 22-48 | -1.026 | 0.307 |
| Mean ± SD | 30 ± 7.725 | 31.34 ± 5.061 | |||
| FT4 (ng/dl) | Range | 0.65-5.9 | 0.8-1.5 | 0.221 | 0.826 |
| Mean ± SD | 1.087 ± 0.737 | 1.064 ± 0.134 | |||
| FT3 (pg/dl) | Range | 2.5-4.1 | 2.5-4 | 0.299 | 0.766 |
| Mean ± SD | 3.142 ± 0.419 | 3.119 ± 0.34 | |||
| TSH (µIU/ml) | Range | 0.1-5.5 | 1.09-4 | -4.804 | <0.001** |
| Mean ± SD | 1.661 ± 1.125 | 2.587 ± 0.769 | |||
| Anti TPO (IU/ml) | Range | 11-33 | 10-29 | 0.495 | 0.622 |
| Mean ± SD | 17.58 ± 4.982 | 17.04 ± 5.89 | |||
| Anti TG (IU/ml) | Range | 12-110 | 10-19 | 3.408 | 0.001* |
| Mean ± SD | 24.56 ± 20.101 | 14.8 ± 2.449 | |||
* means significant (p-value<0.05)
**means highly significant (p-value<0.001)
There was a highly significant difference between both groups in TSH (p-value< 0.001). There was a significant difference between both groups in anti TG (p-value=0.001). There was no significant difference between both groups in age, FT3, FT4 and anti TPO (p-value>0.05).
Table 1: Comparison between drug naïve patients before treatment with interferon beta and healthy volunteers regarding the different variants using t-test.
On comparing control group and drug naïve patients group before treatment with IFN β the following results were detected.
There was no statistical significant difference between the control group and the drug naïve patients group regarding age, FT4, FT3 and TPO (p- value>0.05) (Table 1). As regards TSH, there was a high statistical significant difference between the control group and the drug naïve patients group being higher in control (2.587 ± 0.769 μIU/ml) than drug naïve patients (1.661 ± 1.125 μIU/ml) with (pvalue< 0.001)but both were within normal range (Table 1). Regarding anti TG level there was a statistical significant difference between the control group and the patients group before treatment being higher in patients before treatment (24.560 ± 20.101 IU/ml) than in control group (14.800 ± 2.449 IU/ml) with (p-value=0.001) (Table 1).
On comparing drug naïve patients group before treatment and after 6 months of treatment with IFN β the following results were detected.
There was no statistical significant difference between drug naïve patients group and their follow up after treatment with interferon beta Regarding TSH, FT4, FT3, (p-value>0.05) (Table 2). While regarding anti TPO level there was a statistical significant difference between the drug naïve patients group and their follow up after treatment being higher after treatment with interferon beta (29.660 ± 28.755 IU/ml) than before treatment (17.580 ± 4.982 IU/ml) (p-value=0.004) . This increase in anti TPO antibodies level resulted in shifting of 12 patients from being anti TPO antibody negative before treatment with interferon beta to be positive after treatment (Figure 1). Regarding anti thyroglobulin antibodies, there was a statistical significant difference between the drug naïve patients group and their follow up after treatment with interferon beta being higher in patients after treatment (33.920 ± 32.553 IU/ml) than before treatment (24.560 ± 20.101 IU/ml) (p-value=0.01) with increase in number of patients with positive anti-thyroglobulin antibody after treatment from 15 to 27 (Figure 2).
| Time | Paired Differences | Paired Samples Test t |
P-value | ||||
|---|---|---|---|---|---|---|---|
| Before | After | Mean | SD | ||||
| FT4 (ng/dl) | Range | 0.65-5.9 | 0.2-2 | 0.07 | 0.743 | 0.665 | 0.509 |
| Mean ± SD | 1.087 ± 0.737 | 1.018 ± 0.341 | |||||
| FT3 (pg/dl) | Range | 2.5-4.1 | 2.5-5.6 | 0.06 | 0.648 | 0.655 | 0.516 |
| Mean ± SD | 3.142 ± 0.419 | 3.082 ± 0.537 | |||||
| TSH (µIU/ml) | Range | 0.1-5.5 | 0.037-5 | -0.311 | 1.463 | -1.501 | 0.14 |
| Mean ± SD | 1.661 ± 1.125 | 1.972 ± 1.127 | |||||
| EDSS | Range | 1-5.5 | 1-6.5 | 0.25 | 0.771 | 2.293 | 0.026* |
| Mean ± SD | 2.85 ± 1.546 | 2.6 ± 1.488 | |||||
| Anti TPO (IU/ml) | Range | 11-33 | 12-150 | -12.08 | 27.907 | -3.061 | 0.004* |
| Mean ± SD | 17.58 ± 4.982 | 29.66 ± 28.755 | |||||
| Anti TG (IU/ml) | Range | 12-110 | 10-130 | -9.36 | 24.774 | -2.672 | 0.010* |
| Mean ± SD | 24.56 ± 20.101 | 33.92 ± 32.553 | |||||
* means significant (p-value<0.05)
There was a significant difference between both groups in anti TG (p-value=0.01) and anti TPO (p-value=0.004) and EDSS (p-value=0.026). There was no significant difference between both groups in age, FT3, FT4 aTSH (p-value>0.05).
Table 2: Comparison between drug naïve patients before treatment with interferon beta and after treatment with interferon regarding the different variants using t-test.
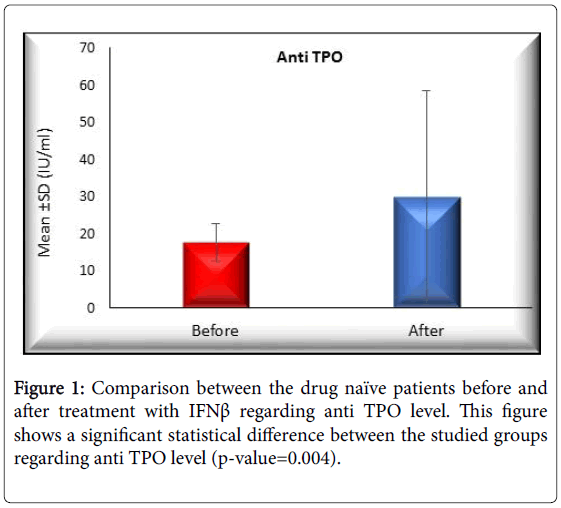
Figure 1: Comparison between the drug naïve patients before and after treatment with IFNβ regarding anti TPO level. This figure shows a significant statistical difference between the studied groups regarding anti TPO level (p-value=0.004).
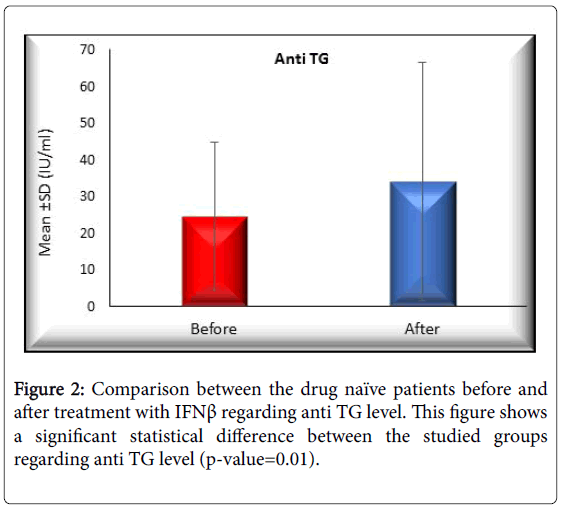
Figure 2: Comparison between the drug naïve patients before and after treatment with IFNβ regarding anti TG level. This figure shows a significant statistical difference between the studied groups regarding anti TG level (p-value=0.01).
Regarding EDSS, there was a statistical significant difference between the drug naïve patients group and their follow up after treatment being less after treatment with interferon beta (2.600 ± 1.488) than before treatment (2.850 ± 1.546) (p-value=0.026) (Table 2).
Regarding neck U/S findings there was no statistical significant difference between the drug naïve patients group and their follow up after treatment with interferon beta (p-value>0.05).
On correlating between anti TG, TPO and other parameters in drug naïve patients group before treatment with interferon beta and 6 months after treatment, There was a highly significant positive correlation between anti TPO level and anti TG level in drug naïve patients before treatment with interferon beta (r=0.648) (p<0.01) and 6 months after treatment (r=0.725), (p<0.001) (Figures 3 and 4), whereas There was no statistical significant correlation between each of anti TG and anti TPO and other parameters before or after treatment including age, free T4, FT3, TSH, EDSS and duration with (p-value>0.05).
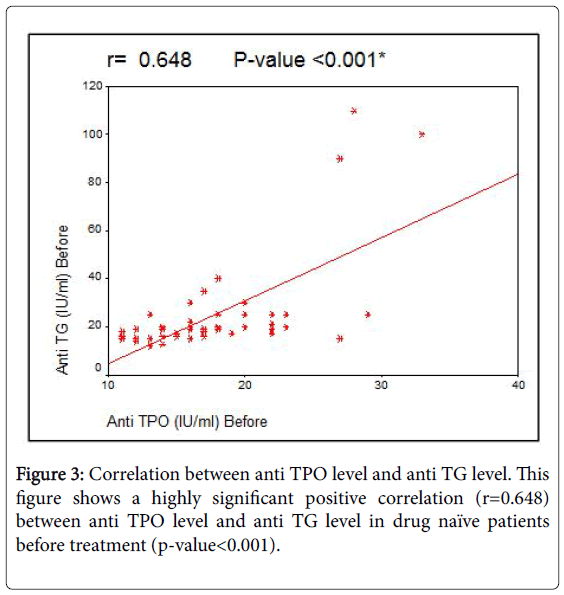
Figure 3: Correlation between anti TPO level and anti TG level. This figure shows a highly significant positive correlation (r=0.648) between anti TPO level and anti TG level in drug naïve patients before treatment (p-value<0.001).
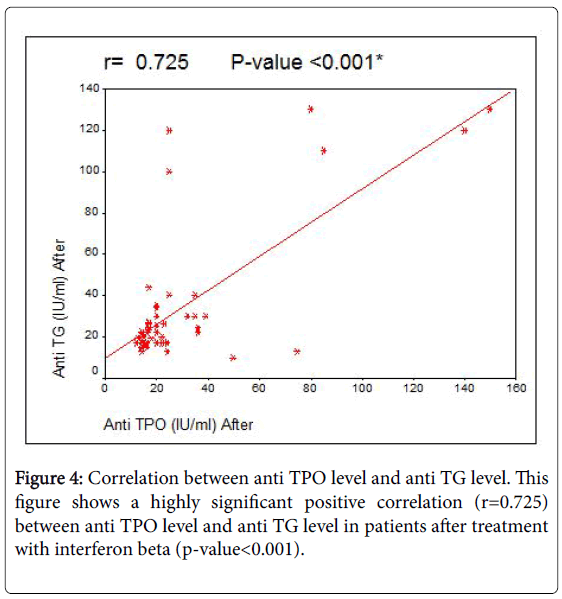
Figure 4: Correlation between anti TPO level and anti TG level. This figure shows a highly significant positive correlation (r=0.725) between anti TPO level and anti TG level in patients after treatment with interferon beta (p-value<0.001).
Multiple sclerosis is a human chronic inflammatory disease of the central nervous system supposed to be a Th1/Th17 type cell-mediated autoimmune disorder [10]. Several studies assessed the presence of thyroid dysfunction and anti-thyroid antibodies in MS patients, finding a prevalence of 2.5-10% of hormonal dysfunction and 4-21% of specific auto-antibodies [11]. In addition to studies aimed at evaluating the prevalence of AITD in drug naive patients with MS, the occurrence of AITD, as a side effect of immune-modulatory treatments for MS, was extensively reported [12].
This study is a prospective study, held to evaluate thyroid function and autoimmunity in newly diagnosed patients with multiple sclerosis before and after treatment with IFN-β, it was conducted on a hundred (100) subjects; their ages ranges from 20 to 50 years, They were divided into 2 groups, Group I included 50 patients recently diagnosed with multiple sclerosis according to MacDonald’s criteria before and after 6 months of medical treatment with IFN-β and group II which included healthy volunteers.
This study showed that there was a statistically significant difference between the control group and the drug naive MS patients group as regards anti TG level being higher in patients before treatment than in control group with (p-value=0.001). While there was a non-statistical significant difference between the control group and the drug naïve patients group as regards anti TPO level (p- value>0.05), in addition , This study showed normal thyroid profile including TSH, FT3 and FT4 in both groups.
In agreement with this study, Seyfert et al. Conducted a prospective study on 100 drug naïve multiple sclerosis patients and 97 healthy volunteers and results showed a significant difference between both groups as regard thyroid antibodies with no change in thyroid profile [13].
Niederwieser et al. also demonstrated an increased incidence of thyroid autoimmunity in men compared with healthy controls [14]. Similarly, Edwards and Constantinescu performed a prospective study on 658 drug naïve MS patients and found an increased thyroid autoimmunity in MS patients compared to general population [15]. Another study done by Petek-Balci reported an association between drug naïve MS patients and thyroid autoimmunity among 106 MS patients by comparing them with healthy volunteers where there was a significant difference between both groups regarding thyroid antibodies with no significant difference regarding thyroid profile between both groups as was found in this study [16].
In contrast to this study, Kreiss et al. [17] and Canaris et al. [18] results showed no significant difference between drug naïve MS patients and control groups as regards thyroid autoantibodies. Similarly, Nielsen et al. found no statistical difference between MS patients and healthy population regarding anti-thyroid antibodies, choosing control members in that study from the first degree relatives of the MS patients upon whom the study was conducted increasing the probability of autoantibodies existence in those subjects resulting in insignificant difference between both groups as regards autoimmunity [19], which may explain the conflicting results between that study and ours. Marrie et al. also performed a prospective study and results found no significant difference regarding anti-thyroid antibodies between MS patients and the healthy group, These discordant results were due to some limitations where thyroid antibodies were measured only in the unrecognizable number of patients who were found to have overt thyroid disease ignoring other MS patients in the study with intact thyroid profile [3].
On comparing drug naïve patients group before treatment and after their treatment with IFN β, regarding anti TPO and anti TG antibodies level, there was a statistical significant difference between the drug naïve patients group and their follow up after treatment being higher after treatment with interferon beta than before treatment (pvalue= 0.004, 0.01) respectively. In similarity to these findings, Karni and Abramsky, [20] Rotondi et al. [21], and Monzani et al. [22] showed that IFN-β therapy has also been associated with a relatively high risk of developing thyroid autoimmunity, Also Monzani et al. underwent a prospective study on 31 MS patients and found that after 1 year of treatment with interferon beta there was a significant increase of thyroid antibodies ( anti TPO and anti TG) being higher after starting interferon beta than before treatment but in contrast to this study it showed increased incidence of overt hypothyroidism which can be explained by the longer duration after which thyroid profile was followed up in that study than this one [23].
On correlating between anti TG, TPO and other parameters in drug naïve patients group before and then after treatment with interferon beta, there was a highly significant positive correlation between anti TPO level and anti TG level in drug naïve patients before and after treatment with interferon beta (r=0.648) and (r=0.725) respectively. There was no statistical significant correlation between anti TG or anti TPO antibodies and other parameters; age, free T4, FT3, TSH and EDSS before and after treatment with interferon beta. In similarity to this study, Annunziata et al. [24] showed that there was no correlation between anti-thyroid antibody titres and other variants as disease duration and thyroid profile, Also with agreement to this study, Karni and Abramsky, found no correlation between thyroid antibodies and age, duration of MS, or proportion of clinical courses [20].
In contrast to this study, Annunziata et al. showed a significant inverse correlation between anti-thyroglobulin antibody titers and EDSS score [24]. Another study done by Nonchev, demonstrated that autoimmune antibodies emerge significantly more commonly in women than in men and correlates directly with age [25]. Also Marazuela et al. reported a significant correlation between thyroid antibodies with both age and gender which do not agree with our results that shows a non-significant correlation between thyroid antibodies (anti TPO and anti TG) with age [26] which may be due to the small sample size of participants whereas correlation between these antibodies with gender was not done in this study as the majority of subjects were females.
This study showed a statistical difference between drug naïve MS patients and healthy controls as regards anti TG antibodies being higher in MS patients with no change in thyroid profile indicating that thyroid autoimmunity occurs more frequently in drug naïve MS patients than healthy controls, Also there was significant difference between drug naïve patients before and after 6 months treatment with interferon beta as regards anti TG antibodies levels as well as anti TPO antibodies levels being higher after treatment with interferon beta with no change in thyroid profile, indicating that thyroid autoimmunity occurs more frequently in MS patients treated with IFN-β than untreated MS patients taking into consideration that anti TPO levels independently correlates with free T3 level.
Routine screening of thyroid functions may be recommended for patients with MS on interferon-beta because some clinical features of thyroid disorders might be difficult to distinguish from interferonrelated side effects as well as multiple sclerosis symptoms. More studies are needed to evaluate thyroid function and auto-immunity after longer time of starting interferon beta.