Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2015) Volume 5, Issue 2
Solid pseudopapillary neoplasm (SPN) is a rare but distinctive pancreatic neoplasm that typically affects young women. Rare cases of extrapancreatic SPN have been reported. Here; we present an unusual case of SPN in a 32- year-old woman who presented with vague abdominal pain. Computed tomography scan revealed a large solid mass in the subhepatic region; adjacent to the head of pancreas and second part of duodenum. The pancreatic gland parenchyma was not involved. Radiologic features were suggestive of a gastrointestinal stromal tumor. On microscopic examination, the lesion exhibited both solid and pseudopapillary pattern with prominent myxoid change in the stroma. Immunohistochemistry showed strong expression of vimentin, CD10, CD56 and alpha 1 antitrypsin. Synaptophysin was focally positive. β-catenin immunostain showed strong nuclear expression; while stain for Ecadherin was negative. Stains for cytokeratin;epithelial membrane antigen; chromogranin A; calretinin; carcinoembryonic antigen and S-100 protein were negative. These morphologic and immunohistochemical features were characteristic of SPN. We present this case to highlight the importance of recognizing SPN at an unusual location. Differentiation from neuroendocrine tumor can be particularly challenging due to their overlapping clinical; radiologic; morphologic and immunohistochemical features.
<Keywords: Solid pseudopapillary neoplasm of pancreas, Pancreatic endocrine tumor, Pancreatic neoplasm, Immunohistochemistry, ? Catenin, Differential diagnosis
Solid pseudopapillary neoplasm (SPN) is an enigmatic pancreatic tumor of uncertain histogenesis. The tumor is histologically characterized by a combination of solid and pseudopapillary growth pattern with tumor cells having abundant clear-to-eosinophilic cytoplasm [1]. It accounts for 1% to 2% of all pancreatic tumors and the overall mortality rate of the tumor has been estimated to be low [2]. The tumor is known to occur anywhere in the pancreas, without any specific site predilection but rare cases of extra pancreatic SPN have been reported [3-9]. SPNs occur as primary tumors outside the pancreas are exceedingly rare and only 13 cases were reported in the English literature. The tumor bears striking clinical, radiologic and histologic resemblance with neuroendocrine tumors (NET) of the pancreas. Immunohistochemical profiles are also sometimes overlapping [10]. In this report, we present a case to highlight the importance of diagnosing SPN when it occurs at unusual site and to emphasize the differentiating features from pancreatic NET.
A 32-year-old woman presented with vague upper abdominal pain for three months. On examination there was a nontender mass in the periumbilical region. Computed tomography scan revealed a well-defined mass lesion in the subhepatic region, in direct relation to the inferior surface of the head of the pancreas, and measured 8.0x7.0 x 6.0 cm (Figure 1).
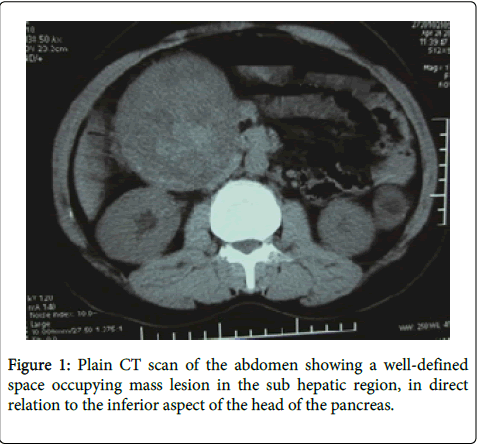
Figure 1: Plain CT scan of the abdomen showing a well-defined space occupying mass lesion in the sub hepatic region, in direct relation to the inferior aspect of the head of the pancreas.
The tumor was displacing the gallbladder upward, and the duodenum and inferior vena cava posteriorly. After contrast administration, the tumor displayed heterogenous contrast enhancement with areas of breakdown, suggestive of degenerative changes (Figure 2).
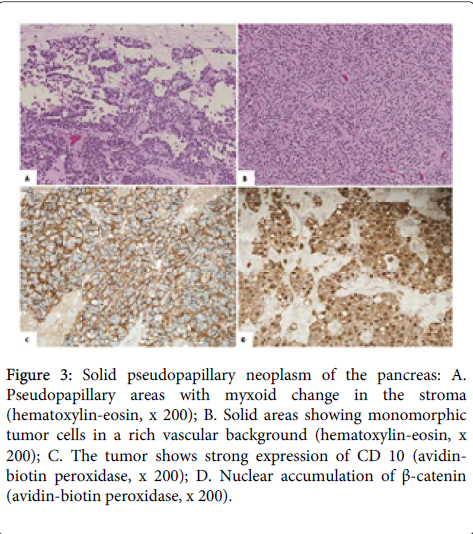
Figure 2: Contrast enhanced CT scan shows heterogeneous contrast enhancement and bizarre shaped breakdown areas denoting degeneration.
The pancreas showed normal CT density. There was no regional lymphadenopathy or hepatic mass lesion. Abdominal radiograph was suggestive of a gastrointestinal stromal tumor of duodenum. The tumor was subsequently excised under general anesthesia.
At operation, it appeared to be closely adherent to the inferior surface of the head of the pancreas. However, it could be easily separated from the pancreas. Macroscopically, the tumor was well circumscribed and measured 10.0×8.0×3.0 cm. The cut surface was solid and grayish brown with areas of hemorrhage. On microscopy, the tumor was encapsulated and showed large areas of hemorrhage and necrosis. Cellular areas exhibited both solid and pseudopapillary pattern with prominent myxoid change in the stroma (Figure 3A).
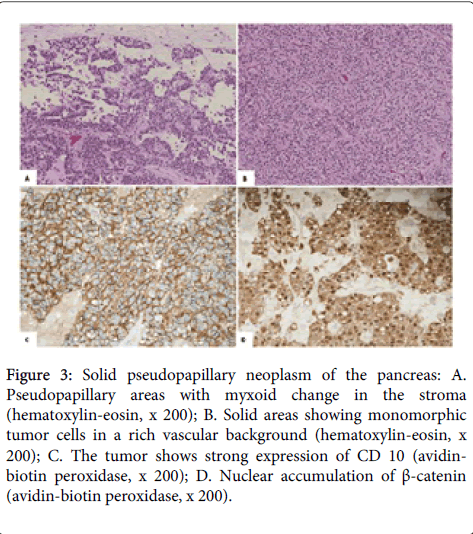
Figure 3: Solid pseudopapillary neoplasm of the pancreas: A. Pseudopapillary areas with myxoid change in the stroma (hematoxylin-eosin, x 200); B. Solid areas showing monomorphic tumor cells in a rich vascular background (hematoxylin-eosin, x 200); C. The tumor shows strong expression of CD 10 (avidinbiotin peroxidase, x 200); D. Nuclear accumulation of β-catenin (avidin-biotin peroxidase, x 200).
The tumor cells were polygonal with abundant eosinophilic to clear cytoplasm, round to oval nuclei with fine nuclear chromatin and inconspicuous nucleoli (Figure 3B). Immunohistochemistry showed strong expression of CD10 (Figure 3C), vimentin, CD56 and α1-antitrypsin. β-catenin immunostain showed both nuclear and cytoplasmic positivity (Figure 3D). Stains for cytokeratin AE1/AE3, epithelial membrane antigen (EMA), E-cadherin, chromogranin A, calretinin, CEA and S-100 protein were negative. Based on the morphologic and immunophenotypic features, a diagnosis of solid pseudopapillary neoplasm was made. The patient had an uneventful postoperative period and there was no recurrence 3 years after the initial surgery.
SPN is an uncommon pancreatic tumor of unknown histogenesis, which was first described in 1959 by Frantz as a distinctive entity [11]. Since then, it has been given many different names such as Frantz tumor, solid and papillary tumor, papillary epithelial neoplasm, solid and cystic acinar tumor, solid and papillary epithelial neoplasm, and papillay-cystic carcinoma [12]. Current WHO Classification retains the most widely accepted terminology “solid pseudopapillary neoplasm”, which designates the two most conspicuous histological features of the neoplasm: solid and pseudopapillary areas [13].
SPN predominantly occurs in adolescent girls and young women, with a reported frequency of 87% to 90% (mean age of 22 to 25 years) [14]. Most patients present with nonspecific symptoms, while the remainder are asymptomatic. In the latter, the tumor is commonly detected incidentally on imaging studies for other reasons. On computed tomography and magnetic resonance imaging, the tumor is often well-circumscribed, encapsulated, and heterogeneous with hemorrhage and cystic degeneration. In the proper clinical context, imaging features can be highly suggestive of the diagnosis [15]. The present case posed a diagnostic challenge to the radiologist due to its unusual location. The lesion was seen outside the pancreatic glandular parenchyma, abutting the head of the pancreas and the second part of duodenum. At this juncture, it is important to know that, though extremely rare, SPN is known to occur at various extrapancreatic sites, such as omentum [3], retroperitoneum [4,5], mesocolon [6], ovary [7], duodenum [8], stomach [8], and liver [9]. Certain SPNs may arise from the ectopic pancreas [5,6]. In the present case, pancreatic rest was not found histologically within resected tissue.
On microscopic examination SPN demonstrates distinctive morphology, with an admixture of varying proportions of solid, cystic, and pseudopapillary patterns [1,12]. Solid areas are formed by cords of small to medium sized, polygonal, monomorphous cells, separated by small vessels. These features are often indistinguishable from a pancreatic NET [1,10]. In such instances, especially when the tumor occurs at an unusual site, attention to morphologic details is particularly important in differentiating the two entities. Pseudoppillary areas with myxoid change in the stroma favor SPN. The cells in SPN have an ample eosinophilic cytoplasm that can be vacuolated. The nuclei are usually uniform, round to oval, harbor frequent nuclear grooves, and usually lack the salt-and-pepper chromatin of NET [12]. Another characteristic feature of SPN is the presence of intracytoplasmic, PAS positive diastase resistant hyaline globules [1,12]. Both the tumors share overlapping immunophenotype, which often complicates the task. SPN often exhibits variable expression of several neuroendocrine markers, such as synaptophysin, neuron specific enolase, and CD 56 [1,10,12]. In the current case, all these markers were positive. However, SPN is consistently negative for the neuroendocrine marker chromogranin A [12], which was also observed in the present case. Similar to NET, epithelial markers like cytokeratin and epithelial membrane antigen are often negative in SPN. In this regard, immunostatining for E-cadherin and β-catenin has been found to be particularly helpful. Recent reports have shown that most SPNs demonstrate nuclear localization of β-catenin and loss of membrane expression of E- cadherin [10,12,16,17]. On the contrary, NET shows cytoplasmic and membrane expression of β-catenin and strong expression of E-cadherin [10]. In our case, the tumor cells also demonstrated strong nuclear expression of β-catenin and were negative for E-cadherin. Recently, there has been a lot of interest regarding involvement of β-catenin gene in the histogenesis of SPN. Most SPNs have been found to harbor mutation in exon 3 of the β-catenin gene [10,18]. This results in abnormal nuclear translocation of β-catenin which can be detected by immunohistochemistry. Hence, β-catenin has emerged as a very useful marker in establishing the diagnosis of SPN.
The prognosis of SPN is excellent after local excision. When the tumor is confined to the pancreas, up to 95% of patients are cured by complete surgical excision [19]. Local recurrence is less than 10% and usually occurs within 4 years [14]. Overall 5-year survival of patients with SPN has been reported to be about 95% [19]. Recently, there are 2 reported cases of death, in which the tumor demonstrated malignant histology at diagnosis [20].
In summary, SPN is an uncommon pancreatic tumor of low malignant potential. It is important to recognize this entity when it occurs at unusual location, as happened in the present case. Differentiation from pancreatic NET is often difficult, owing to overlapping clinicopathologic presentations. Attention to morphologic details and judicious utilization of immunohistochemical markers is helpful in distinguishing the two. β-catenin has emerged as a very useful marker, considering its high degree of sensitivity and specificity in diagnosing SPN.