Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2015) Volume 4, Issue 2
Background: Papillary thyroid cancer (PTC) generally occurs sporadically but about 5% of cases are familial in origin. Furthermore, family history has been established as an influential risk factor for PTC. This study determines whether patients with a family history of thyroid cancer harbor more aggressive variants of PTC.
Materials and Methods: A retrospective review of prospectively collected data of 1779 consecutive patients who underwent thyroidectomy was performed. Patients were divided into patients who had a history of PTC in first degree relatives (n=39) and those that did not (n=1740). Patients with PTC on final pathology were further subdivided into those with less aggressive (classic and follicular) and patients with more aggressive (diffuse sclerosing and tall cell) variants of PTC. A two tailed Z test at a significance level of p<0.05 was used to compare groups.
Results: Of 1779 patients included, 39 (2.2%) had a family history of PTC. Of patients with a positive family history, 20 (51.2%) had PTC on final pathology. Furthermore, these patients had a significantly increased incidence of more aggressive variants of PTC at 15.4% (6/39) compared to patients with no family history of PTC at 2.7% (47/1740) (p<0.05).
Conclusions: Patients with a positive family history of PTC have a significantly higher incidence of more
aggressive PTC variants. A positive PTC family history, therefore, should be considered a risk factor for its more aggressive variants
Thyroid cancer is the most prevalent endocrine malignancy of which its incidence has steadily increased over the past four decades. Although most papillary thyroid cancer (PTC) occurs sporadically, about 5% of cases may be familial in origin [1]. Of the various subtypes of thyroid carcinoma, PTC accounts for the vast majority, comprising 85% of new cases. While it has the best prognosis of all thyroid malignancies with a 10-year overall survival rate of >95%, not all forms of PTC have an indolent course. PTC can be further subdivided based on histologic appearance with some variants associated with a more aggressive clinical course of disease as defined by extravascular invasion, necrosis, and lymph node involvement at time of diagnosis. [2-4].
In addition to classification based on histological appearance and natural course of disease, PTC can be subdivided based on whether the disease exhibits an inheritance pattern. PTC generally occurs sporadically, but a small sub-population of 4-6% demonstrates a familial component to the disease. These sporadic and familial forms of PTC are histologically indistinguishable. As early as 1980, a positive family history of PTC was shown to correlate with a higher incidence of disease as compared to the general population. More significantly, family history seems to be associated with younger age at diagnosis and higher rates of metastases [5]. Familial PTC, however, remains to be a relatively rare entity.
Knowledge of the familial component of certain types of thyroid malignancy has been established; however, the factors underlying familial PTC have not yet been fully elucidated. Thyroid cancer can be broadly categorized as medullary or nonmedullary carcinoma based on the cells of origin. Medullary thyroid cancer (MTC) arises from the parafollicular cells and has a well-studied familial component, the genetics of which have been somewhat established. Nonmedullary thyroid cancer (NMTC) includes PTC, follicular, Hürthle cell and anaplastic subtypes. PTC is the most common, however, comprising 85% of all NMTC cases [6].
In general, positive family history of thyroid malignancy has been shown to be associated with a more aggressive course of disease as measured by rates of reoperation, distant metastases at the time of diagnosis and death secondary to malignancy [7]. While some evidence suggests that patients with familial NMTC have more aggressive disease, it remains unclear whether this is specifically true of patients with a family history of PTC [8]. Moreover, aggressive variants of PTC have been shown to correlate with higher rates of lymph node involvement, distant metastases and death [9]. The connection between family history of PTC and its more aggressive variants has not been explored. This study determines whether patients with a positive family history of PTC have a significantly greater predisposition to more aggressive variants of PTC.
A retrospective review of prospectively collected data of 1779 consecutive patients who underwent thyroidectomy at a single institution was performed. Patients were divided into two groups based upon family history of PTC. There were 39 patients with a positive family history of PTC compared to 1740 patients who did not have a familial component to the disease. Furthermore, patients with positive and negative family histories who displayed PTC on final pathology were further subdivided into less aggressive and more aggressive variants of PTC. Although the variants of PTC are defined histologically, the broader categories of “more aggressive” and “less aggressive” pertain to the clinical course of the disease. The variants associated with a relatively worse prognosis classified as “more aggressive” included diffuse sclerosing, tall cell, combined diffuse sclerosing and tall cell, solid cell, clear cell and oncocytic variants. Conversely, “less aggressive” variants associated with better clinical outcomes included classic, follicular, as well as combined classic and follicular variants [10].
For this study, a positive family history was defined as a patient having at least one first degree relative with PTC. Patients with a positive family history and aggressive forms of PTC were compared to patients with no affected family members. When family history proved positive for PTC, and the affected family member had undergone thyroidectomy, tumor pathology was re-reviewed from final pathology reports. Family history and patient demographics including radiation exposure and other familial cancer syndromes were confirmed by review of patient clinic notes. The presence of a positive family history was recorded along with number of family members.
In total, there were 734 patients who underwent thyroidectomy for PTC as confirmed by final pathology. Of this study group, 20 patients were in the positive family history group, while the remaining 714 patients were in the negative family history group. PTC was defined as thyroid malignancy of follicular cell origin, which included the less aggressive classic and follicular variants as well as the more aggressive diffuse sclerosing, tall cell, solid cell, clear cell and oncocytic variants. Additionally, patients with combined classical and follicular variants as well as combined diffuse sclerosing and tall cell variants were considered to be two distinct subtypes of PTC. The remainder of the patients that did not exhibit PTC on final pathology had benign disease or other malignancies.
All patient charts and information were reviewed in accordance with the Institutional Review Board guidelines at the University of Miami Leonard Miller School of Medicine. All statistical analyses were performed using SPSS (IBM, version 21; SPSS Inc., Chicago, IL). Aggressive and indolent variants were examined in the positive family history as compared to the negative family history group using a two tailed Z-test. A P<0.05 was considered statistically significant.
Of the 1779 patients, there were 39 patients with a positive family history of PTC in at least one first degree relative, and 1740 patients with no family history of PTC. Overall, 2.2% (39/1779) had a family history of PTC in first degree relatives. Of these patients with a positive family history, 51.3% (20/39) had PTC on final pathology whereas 41.0% (714/1740) of patients with a negative family history had PTC on final pathology. Of patients with a positive family history, 48.7% (19/39) had benign disease. Of patients with a negative family history, 55.5% (965/1740) had benign disease and 3.5% (61/1740) had malignancies other than PTC (Figure 1). Group characteristics of patients revealed that women were predominant in both groups. Although other studies have shown patients with familial history of thyroid cancer present with this malignancy at a younger age, there was no significant difference for both groups (Table 1).
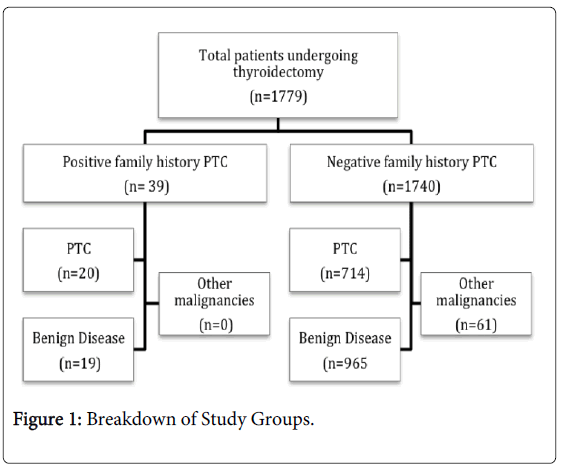
Figure 1: Breakdown of Study Groups.
| Study group | Positive family history | Positive family history and PTC | Negative family history | Negative family history and PTC | |
|---|---|---|---|---|---|
| n | 1779 | 39 | 20/39 | 1740 | 714/1740 |
| Gender | |||||
| Female | 1491 (83.8%) | 34 (87.2%) | 16 (80.0%) | 1457 (83.7%) | 580 (81.2%) |
| Male | 288 (16.2%) | 5 (12.8%) | 4 (20.0%) | 283 (16.3%) | 134 (18.8%) |
| Age | |||||
| Mean age | 50 ±14.0 | 46 ±15.1 | 47 ±14.4 | 49 ±14.4 | 48 ±14.8 |
| <45 y/o | 663 (37%) | 17 (43.6%) | 9 (45.0%) | 647 (37.2%) | 293 (41.0%) |
| >45 y/o | 1116 (63%) | 22 (56.4%) | 11 (55.0%) | 1093 (62.8%) | 421 (59.0%) |
Table 1: Group Characteristics
The breakdown of the variants according to family history of PTC indicated that a larger proportion of patients with a positive family history harbored more aggressive variants as opposed to patients with a negative family history. Patients with a family history of PTC had a significantly higher rate of combined aggressive variants (diffuse sclerosing, tall cell, combined diffuse sclerosing and tall cell, solid cell, clear cell and oncocytic variants) of PTC (6/39; 15.4%) when compared to patients without a family history (47/1740; 2.7%) (p<0.05). Only 5 patients harbored the latter 3 aggressive variants and they were all in the negative family history for PTC group (Figure 2). When PTC variants were examined individually, patients in the positive family history group had significantly greater proportions of diffuse sclerosing variant as well as combined classic and follicular variants: 7.7% (3/39) and 10.3% (4/39) as opposed to 2.4% (27/1740) and 1.0% (17/1740) in the negative family history group, respectively (Table 2).
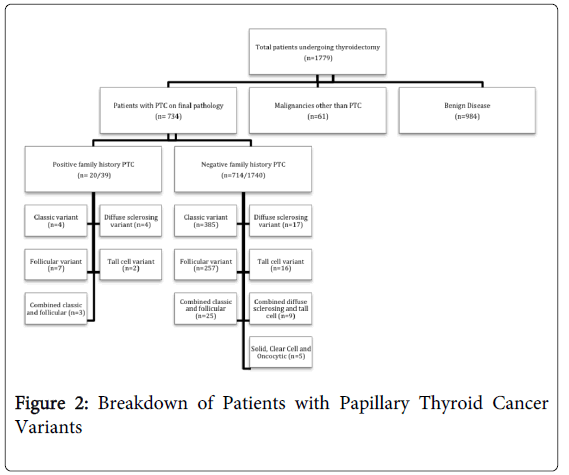
Figure 2: Breakdown of Patients with Papillary Thyroid Cancer Variants
| Total (n=1779) | Positive Family History of PTC (n= 39) | Negative Family History of PTC (n=1740) | P value | |
|---|---|---|---|---|
| Papillary thyroid cancer | 714 (40.1%) | 20 (51.3%) | 714 (41.0%) | 0.197 |
| Less aggressive variants | 681 (38.3%) | 14 (35.9%) | 667 (38.3%) | 0.757 |
| Classic variant | 389 (21.9%) | 4 (10.3%) | 385 (22.3%) | 0.077 |
| Follicular variant | 264 (14.8%) | 7 (17.9%) | 257 (14.8%) | 0.582 |
| Combined classic,follicular | 28 (1.6%) | 3 (7.7%) | 25 (1.4%) | 0.002 |
| More aggressive variants | 53 (3.0%) | 6 (15.4%) | 47 (2.7%) | <0.001 |
| Diffuse sclerosing variant | 21 (1.2%) | 4 (10.3%) | 17 (1.0%) | <0.001 |
| Tall cell variant | 18 (1.0%) | 2 (5.3%) | 16 (0.9%) | 0.009 |
| Combined diffuse sclerosing, tall cell | 9 (0.5%) | N/A | 9 (0.5%) | N/A |
| Solid cell, clear cell, oncocytic | 5 (0.3%) | N/A | 5 (0.3%) | N/A |
Table 2: Patients with PTC Grouped According to Variant by Final Pathology
Although it has been established that family history is a critical factor to consider in the diagnosis of patients with thyroid cancer in general, there remains ambiguity regarding whether patients specifically with a family history of PTC harbor more of its aggressive variants. The familial component of PTC has been suspected since the early 1980s, but rarity of the disease has limited the research elucidating the particulars regarding genetics, histological subtypes, course of disease progression and demographics of the affected patient population. As separate factors, however, both its aggressive histologic variants and family history of PTC have been demonstrated in this current study to correlate with more aggressive course of disease.
The poor prognosis associated with aggressive variants of PTC is well established. Epidemiological studies have underscored the association between diffuse sclerosing and tall cell variants of PTC with poor prognostic factors including higher rates of lymph node involvement, multifocality, distant metastases, and death. Patients with follicular and Hurtle cell microcarcinoma subtypes of PTC were also shown to have increased rates of distant metastases and reduced survival [9,11,12]
When determining patient risk for aggressive disease, family history should be considered in addition to histologic variant of the cancer. Current guidelines, as determined by the American Thyroid Association (ATA), indicate that positive family history of thyroid malignancy constitutes an independent risk factor necessitating more aggressive work-up and treatment of thyroid nodules and known malignancies [13]. The basis of such guidelines rests on research that has shown positive family history of thyroid malignancy to be associated with higher rates of reoperation, distant metastases at the time of diagnosis and death secondary to malignancy [7]. Family history is a crucial factor for assessing patient risk and prognosis. In fact, traditional staging systems have been shown to be less accurate for patients with a family history of thyroid cancer unless the staging accounted for positive family history [14]. Although the correlation between family history and aggressive disease has been established, the reasons underlying this connection have not yet been determined. Perhaps one factor behind this phenomenon is that patients with a family history of thyroid cancer tend to harbor the histologically more aggressive variants of PTC.
In the literature, however, studies examining whether patients with family history of PTC have more advanced disease due to a higher incidence of harboring aggressive variants are lacking. To date, two previous studies have approached this question, albeit indirectly. One study examined 93 patients that had less aggressive classical and follicular variants as well as a positive family history of PTC. This published report assessed whether family history alone correlated with more aggressive disease. The results indicated that despite exhibiting conventional PTC variants, patients with a family history of PTC were younger at the age of diagnosis with decreased disease-free survival time and higher rates of lymph node involvement compared to patients with sporadic PTC [15]. Another study conducted a multivariate analysis to determine whether aggressive variant alone was predictive of poor prognosis after adjusting for tumor size and distant metastases. The study findings indicated that variant alone was not necessarily predictive, but rather, features associated with aggressive variants conferred more advanced stage of disease and, in turn, poor prognosis [16]. Both studies underscored the fact that family history as well as aggressive variants of PTC correlated to more aggressive clinical course of disease separately. The latter study suggests that variant alone may not be predictive but, again, did not examine whether patients with family history of PTC tend to possess more aggressive forms of PTC.
Current ATA guidelines indicate that positive family history necessitates comprehensive work-up and evaluation [13]. The authors’ study shows that more aggressive variants of PTC are one of many potential reasons why patients with a positive family history tend to have poorer prognoses. Until other factors are determined, knowledge of the correlation between positive family history and aggressive disease course can guide the clinical approach. Patients with a positive family history of PTC should be referred to surgeons earlier for possible management. Surgeons presented with this subpopulation of patients may need to perform more extensive procedures including lymph node dissection since such patients have higher rates of multifocality, lymph node involvement and lymphovascular invasion. Additionally, radioactive iodine therapy should be considered for all such patients since they are at a particularly high risk of disease recurrence.
The limitations of this study may be attributed to the retrospective design, referral bias, patient self-report, and unknown environmental and genetic factors. The patients included were referred specifically for surgical evaluation and, for this reason, represent a highly-selected group. In addition, family history of cancer of PTC was confirmed by chart review and final pathology report when possible. Other studies, however, have indicated that a positive patient history can have an accurate association with thyroid cancer. Perhaps most significant is the fact that the genetics of familial PTC are, as of yet, unknown. Due to the limited number of cases, genetic studies have examined only the broader category of NMTC rather than PTC specifically. The studies to date have looked only at a handful of families that seem to carry a predisposition to the disease. It remains to be seen whether these different families all share the same underlying genetic factors. The heritable basis of NMTC appears to be multifactorial and some loci that confer a predisposition to NMTC have been potentially identified, but the environmental factors remain unknown [17-19]. Further research will eventually uncover the genetics and environmental factors that underlie the disease process.
In conclusion, while family history and histologic variant of PTC are independently correlated to degree of disease aggressiveness, it is clear that patients with a family history of PTC tend to harbor more aggressive variants of the disease. This study, to the best of the authors’ knowledge, is the first to examine the correlation between family history and proportion of aggressive variants of PTC. Although patients with a positive family history of PTC that have more conventional forms may also have a more aggressive course of disease as compared to sporadic counterparts, there is still value in assessing both factors when formulating a treatment plan. Treatment for all PTC patients with a positive family history, regardless of variant, should entail a workup and evaluation including FNA of subcentimeter nodules, screening at a younger age, and earlier surgical intervention. As more research uncovers the biological mechanisms underlying the development of familial PTC, the evaluation of these patients will become straightforward more likely with genetic testing. Until then, surgeons must rely on assessment of the associated risk factors including family history and histologic variant of PTC to determine treatment. Presence of either family history or aggressive variant in PTC should indicate more aggressive work up separately and certainly, even more so, when combined.