Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2012) Volume 2, Issue 1
Endocrine pancreatic tumors (EPTs) are rare entities with a low incidence (3-10 per million). A relatively frequent feature (15-53%) among this group of tumors is represented by the non-functioning endocrine pancreatic tumors (NFEPTs) whose peculiarity is due to the absent secrection of mature or active hormones, leaving the patient free from clinically evident hypersecrection syndromes, generally discovered when the mass effect becomes evident, the adjacent pancreatic structures (splenic, superior mesenteric and portal vein, celiac or superior mesenteric arteries, common bile duct, duodenum, etc.) are infiltrated or hepatic metastases are growing. A potentially malignant attitude is high and well related to the dimension of the tumor with inexorably fatal outcome if appropriate surgery is delayed. The size of the mass and an evident involvement of nearer vascular structures might rise some doubts about the decision to radically remove the tumor. An aggressive surgery should be balanced with the risk/benefit ratio for generally young patients with a reasonable long life expectancy. We parallel two clinical cases among the patients we observed through the years at our institution and operated on by the same surgeon, who were displaying the same tumoral histology and loco-regional invasiveness of portomesenteric axis, but differing one each other for the presence of metastatic disease to the liver the first case. Further aim of the present report is to support the evidence of the feasibility and safeness of extensive surgical demolition with prosthetic reconstruction of the porto-mesenteric axis.
<Endocrine pancreatic tumors (EPTs) are rare entities with a low incidence (3-10 per million) [1], being the 5% of all neoplastic variety of pancreas [2].
A relatively frequent feature (15-53%) among this group of tumors is represented by the non-functioning endocrine pancreatic tumors (NFEPTs) [3,4] with an absent secrection of mature or active hormones, and no clinically evident hypersecrection syndromes. The consequences are represented by indolent clinical courses and late diagnoses so they are generally discovered when the mass effect becomes evident, the adjacent pancreatic structures are infiltrated or hepatic metastases are growing. The size of the mass and an evident involvement of nearer vascular structures might raise some doubts about the decision to radically remove the tumor along with infiltred major vessels and the subsequent need of their reconstruction.
We considered of some interest to parallel two clinical cases operated on by the same surgeon, who were displaying the same tumoral histology and loco-regional invasiveness of porto-mesenteric axis, but differing one each other for the presence of metastatic disease to the liver in the first case. Further aim is to support the evidence of the feasibility and safeness of extensive surgical demolition with prosthetic reconstruction of the porto-mesenteric axis.
Clinical history and surgery
39 years old man who presented with intermittent mild epigastric pain not related with meals, with saltuary emission of unformed stools and a personal and familial negative past medical history. The routine blood tests resulted normal and abdominal US evidenced of a corporo-caudal pancreatic mass. A contrasted abdominal TC scan confirmed the presence of 4 cm. mass confined to the pancreatic body with partial thrombosis of the superior mesenteric vein (SMV), signs of portal hypertension and multiple bilateral liver metastases. Routine serological neoplastic markers were then tested and resulted normal, while NSE and CgA were significantly altered such as somatostatin (SS) and CCK, while PP and Glucagon were only slightly elevated. Basal Gastrin, VIP and Insulin were normal. An invasive NFEPT and an explorative laparotomy were performed. The intraoperative findings were consistent with the pre-operative imaging and in consideration of the young age of the patient, the need of providing symptoms relief and life-expectancy, the decision was taken to radically treat the primary lesion. The liver was left untouched. After gastro-epiploic dissection, lesser sac was opened to identify a hard, white mass within the pancreatic body. Spleno-pancreatic resection up to the pancreatic istmus was undertaken after middle colonic vessels were resected because not detachable by the tumor. Portal vein and superior mesenteric vein were then encircled with a vessel loop and after clamping, thrombectomy of the porto-mesenteric axis with partial resection of portal mesenteric wall was accomplished. Locoregional lymphadenectomy was also carried out. Reconstruction of the defect was made by mean of a PTFE patch. Hystology confirmed the islet cell carcinoma with 3 metastatic peripancreatic lymph-nodes.
Outcome and follow-up
The early post-operative outcome was uneventful and the patient discharged on post-operative day 8. The follow-up (24 months) was programmed every three months. No surgical related complications, iatrogenic diabetes and portal vein occlusion were observed along the follow-up period. The patient was submitted to a chronic long-release therapy with somatostatin analogs.
Four months later an urgent open cholecistectomy was required for acute lithiasic cholecistitis. Three chemotherapy courses with streptozocin were then started after 6 months from surgery up to 1 year according to tumoral progression’s status. Nevertheless liver metastatic disease could not be controlled by medical therapy, no loco-regional recurrence was radiologically observed. Serological markers were within the normal range along the whole follow-up period, with the exception of NSE and CA 19-9. A second reoperation was undertaken at 24 months after the first surgery and 6 months after the last course of systemic chemotherapy, with cytoreductive intent over the hepatic lesions which remained stable along the neoadjuvant period. All the 10 metastases were treated with a combination of modalities including metastasectomies (4), cryo-ablation (4) and alcoolization (2). Unfortunately few months later the patient showed recurrent disease confined to the residual liver and he eventually died with liver tumoral progression after eight months.
Clinical history and surgery
30 years old woman complaining the occurrence in the last months of a mild post-prandial epigastric pain with gastric fullness. Her past personal and familial medical histories were negative. EGDS failed to display any abnormality and subsequent abdominal US evidenced a pancreatic mass. An abdominal enhanced-CT scan revealed the presence of 11x5 cm. disomogeneous and hypodense bulky mass of the pancreatic body-tail, bulging the posterior gastric wall without infiltrating it and widely encompassing the celiac trunk (Figure 1). Portal thrombosis with portal hypertesion and colloteral venous circulation could also be evidencied (Figure 2). Blood tests at the admittance were normal also including endocrine biochemical markers with the exception of serum SS which resulted slightly elevated. Even if not fully supported by radiological and biochemical evidences the patient was diagnosed with suspected invasive NFEPT on a clinical/radiological basis and a SS receptor scintigraphy was planned. This latter examination did not contribute to preoperatively clear the diagnosis, but in consideration of the high clinical suspicion, the age of the patient, the ongoing symptomatology and the clear invasive attitude of the mass, the patient was scheduled for an explorative staging laparoscopy and, if permissive, to a laparotomic radical surgery with a curative intent.
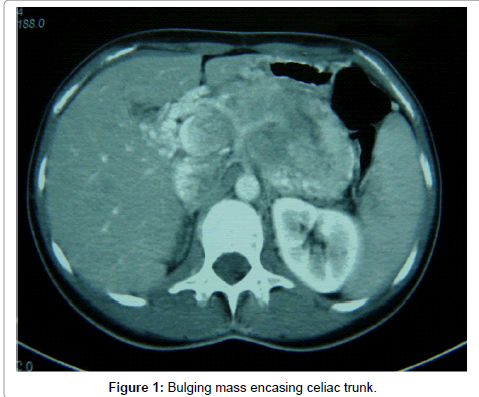
Figure 1: Bulging mass encasing celiac trunk.
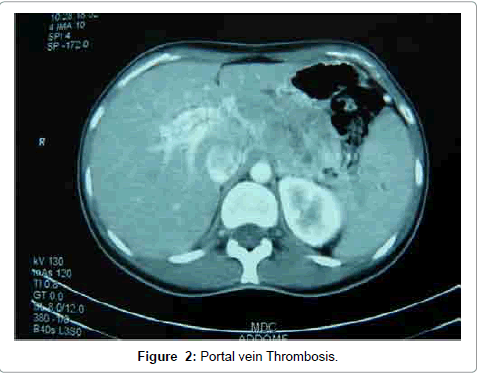
Figure 2: Portal vein Thrombosis.
A bilateral subcostal laparotomy was performed. After coloepiploic division the lesser sac was entered to expose the pancreatic tumor. In order to completely mobilize the pancreas en bloc with the tumor, ligation and division of the left gastric artery was necessary. At this point cautional dissection of the tumor by the vascular structures and the gastric wall could be safely accomplished after preliminary division of splenic artery and vein at their origin to better mobilize the specimen avoiding any vascular injury. The pancreatic neck was freed and divided and the superior mesenteric-portal vein encircled and clamped for a complete thrombectomy. Loco-regional lymphFigure 1: Bulging mass encasing celiac trunk. adenectomy was accomplished along hepatic artery, celiac trunk and peripanceatic fat, while left gastric artery was divided at its origin as abovementioned. After resection of the portal vein from the confluence up to the bifurcation, the spleno-pancreatic specimen was removed, and the flow restored by the mean of a 10 mm PTFE prosthesis with optimal reperfusion as confirmed by full decongestion of pathological venous collaterals and intraoperative power-doppler (Figure 3).
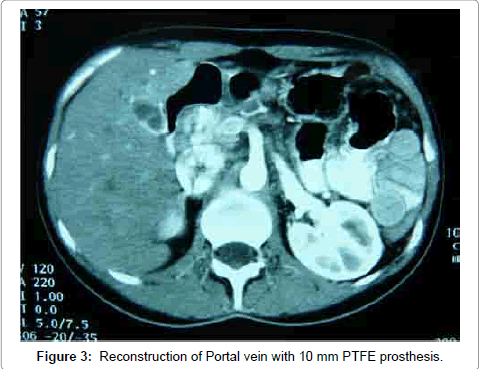
Figure 3: Reconstruction of Portal vein with 10 mm PTFE prosthesis.
The pathologist’s evaluation hystologically confirmed the well differentiated pancreatic endocrine carcinoma with lymph-haematic invasion of the peripancreatic small vessels and neoplastic portal vein thrombosis.
Outcome and follow-up
The early post-operative course was uneventful and the patient was discharged at post-operative day 18. At discharge a long-life substitutive therapy with pancreatic enzymes and a six-month long adjuvant therapy with long-release somatostatin analogs were started. After one month an abdominal CT scan was done along with serological endocrine markers determination. After this preliminary evaluation, negative for oncologic progression and prosthetic occlusion, a trimestral follow-up was established for the first six months and then semestrally for the next first year. Afterwords a yearly visit at the outpatient clinic with abdominal CT and porto-mesenteric power-doppler with a semestral determination of endocrine markers were planned.
At present, after a 27 months follow-up neither local tumoral progression nor metastatic disease could be evidenced either radiologically and biochemically, PTFE prosthesis is well patent with no signs of portal hypertension.
The natural history of the sporadic NFPETs has been poorly studied because of the rarity of the disease and the absence until a few years ago, of an effective and proper classification with consideration of their real malignant potential and progression. Most of the informations could be derived by the study of their familial genetic counterparts. Differently from the sporadic form, these familial tumors are multiple, of various dimension and accompanied by multiple islet cell microadenomas and often associated to functioning EPTs [5,6].
A recent prospective study showed that the rate of NFPETs in MEN1 patients is higher than 55% when endoscopic ultrasound (EUS) is performed to detect them [7]. Since the number and size of the NFPETs tend to increase in time and the affected population is relatively young (median age is 39 years), this rate is certainly going to grow as time passes by.
The revision of the NFPETs in MEN1 has clearly shown an association between large primary tumor size, the presence of distant metastases and the mortality due to tumoral progression [7-9]. EPTs have been recently stratified, on the basis of the WHO classification, in 3 categories: benign tumors, well-differentiated carcinomas with low-grade malignant behaviour and poorly-differentiated carcinomas with high grade malignant behaviour [10]. Malignancy is assessed by the presence of invasiveness of adjacent structures or viscera and/ or metastases or, in their absence, by the following criteria: vascular or perineural microinvasion, tumor size >4 cm., Ki 67 proliferative index >2%, presence of necrosis and/or clear cellular atypia, capsular penetration, mitotic rate >2, loss of chromogranin A (CgA) and calcitonin immunoreactivity, argyrophilia and nuclear p53 protein accumulation [11]. Surgeons approaching EPTs must firstly address the problem of a correct diagnosis that could be uncertain when facing a bulky pancreatic mass with charachteristics resembling the more common pancreatic adenocarcinoma. When clinical history and pattern may rise doubts about the real nature of the pancreatic mass, dosage of biomarkers and SSRs scintigraphy (Octreoscan) should be ruled out. In case of positivity of one of these tests the diagnosis of EPT can be suspected. In case both the tests were negative and a strong clinical doubt persists about final diagnosis, biopsies should be taken from the lesion to definitively assess the correct diagnosis since adjuvant and surgical therapies and prognosis are radically different.
Curative surgery of NFEPTs is warranted by a radical R0 removal of the primary tumors along with regional lymphadenectomy in M0 patients with reported 5 years survivals of more than 70% [12,13]. The evidence of a surprisingly high 5 years survival rate of untouched locally advanced primaries in M0 patients (46%), rises many doubts about the need or radically treat these patients considering the potentially life-threatening complications [12-14]. Despite combined resection of primary tumor and metastases seems rational when complete removal is achieved, debulking surgery has no role in case of NFEPTs and such indication is generally reserved to treat hormonal syndromes in case of functioning endocrine tumors [3].
In the 1st case, multiple hepatic metastases had been detected preoperatively, but we resected only the main pancreatic NET to avoid an excessive aggressiveness of the surgical approach. We try not to associate resection of a pancreatic tumor with an extended procedure on the liver, so we delayed major liver resections in case of multiple and bilateral hepatic metastases.
The condition of a major vascular invasion with a neoplastic thrombosis is not a rarity with a 26% of the cases in the experience of Chung et al. [13]. This circumstance can occur either because of direct tumor infiltration or because of neoplastic thrombosis in the splenic vein. In this last case an “en bloc” resection of the left pancreas and the spleen along with the involved tract of mesenteric and portal vein is the treatment of choice. Differently from the case of the pancreatic adenocarcinoma, when an endocrine carcinoma involves a vascular structure, the prognosis is not affected if a R0 resection is accomplished. Even if there have been few reports of vascular resection and reconstruction after removal of endocrine carcinoma [2,15] this aggressive surgery is well described and derived by the experience on pancreatic adenocarcinoma. Resection and reconstruction of the portal vein can be accomplished by an end to end anastomosis if less than 4 cm. in lenght are sacrificed. When a vein replacement is necessary, autologouses veins, homologouses veins or a synthetic prosthesis can be used. Even if an autologous graft is generally preferred for its lower thrombogenic property, polytetrafluoroethylene (PTFE ) is largely used for these purposes with good results. NFPETs are surgically treatable diseases with curative intent in M0 patients with a resectable primary tumor with no microscopic residual (R0). If major vascular structures, such as splenic vein and porto-mesenteric axis are invaded also with neoplastic thrombosis, resection and reconstruction of the involved vessels is recommended to warrant cure. Aggressive surgery including vascular resection is still debated in case of locally advanced nonfunctioning tumors with metastatic disease to the liver or distant metastases. If all the tumoral deposits cannot be excised R0, the survival doesn’t change when compared to that of untouched patients, while the complications of such aggressive surgery are present.
We recommend that patients be evaluated preoperatively by surgeons in concert with their oncologist to assess preoperative optimization, timing, and extent of resection. The technique of vascular dissection and decompression, although established, is sometimes extremely difficult. Nearly 80% of patients explored elsewhere were successfully radically operated in experienced Centers familiar with the technique of vascular resection and reconstruction, with improvements in symptoms and survival. An en bloc resection of invasive main pancreatic NET with vascular invasion should be reserved for patients with young age, low comorbility and potentially long life-expectancy.