Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Case Report - (2018) Volume 7, Issue 2
A 32-year-old female presented with complaints of recurrent urinary tract infections, tender vaginal swelling and painful intercourse. She underwent repeated aspirations of anterior vaginal wall swelling by gynecologist considering it as primary vaginal cyst but the swelling was recurrent after short course of time. MRI imaging of pelvis was performed after the opinion of urologist considering the possibility of the infected urethral diverticulum. MRI examination revealed multiloculated fluid containing lesion around urethra appearing like saddle bag and spoke wheel on axial images and mimicking like enlarged prostate on sagittal images with submucosal enhancement and diffusion restriction of contents suggesting infected urethral diverticulum.
Objective: We are discussing role of MRI imaging with the help of radiological signs in the accurate diagnosis of urethral diverticula in symptomatic patients to avoid painful and complicated interventional imaging procedures and narrow down the possibility of alternate diseases in the same territory.
Keywords: Urethral diverticulum; Female prostate; Saddle bag; Spoke wheel
The urethral diverticulum is a pathological condition of lower urinary tract characterized by the formation of single or multiple sacs like outpouchings encircling urethra. This condition is having female preponderance and considered as acquired disease secondary to burst of infected and dilated periurethral glands in urethra forming diverticulum. Few radiological signs of urethral diverticulum have been described in this article on MRI imaging referred as female prostate sign due to its appearances like enlarged male prostate on sagittal planes and saddle bag or spoke wheel appearance of multiloculated fluid-filled diverticulas wrapping around urethra on axial images.
A 32 year old female with normal menstrual cycles presented with complains of low-grade fever, recurrent urinary tract infections, vaginal swelling, and painful intercourse. Her laboratory investigation reports were showing raised titers of inflammatory markers. On clinical examination there was a tender cystic swelling in the anterior vaginal wall with some pus discharge, she previously underwent repeated aspirations of infected purulent material by the gynecologist considering it anterior vaginal cyst however the swelling was recurrent after the course of antibiotic therapy. MRI imaging of pelvis was requested after urological consultation considering the possibilities of an infected vaginal cyst or urethral diverticulum. MRI pelvis examination with contrast was performed on 1.5 Tesla scanner using four channel body coil with standard imaging protocol using T1, T2- weighted and fat saturation sequences using thin slices and the minimum interslice gap in axial, coronal, and sagittal planes with the special focus on urethra/periurethral, bladder base and perianal region (Figure 1). MRI study revealed well-defined round shaped T2- weighted hyperintense signal multiloculated fluid containing lesion wrapping around proximal urethra appearing like saddle bag and spoke wheel on axial T2 weighted images and mimicking like enlarged male prostate with mass effect on bladder base on T2 weighted sagittal planes (Figure 2).
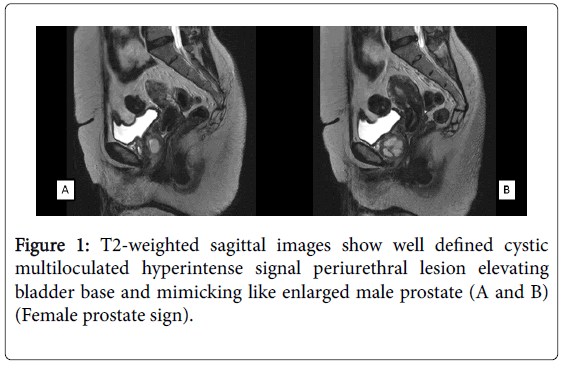
Figure 1: T2-weighted sagittal images show well defined cystic multiloculated hyperintense signal periurethral lesion elevating bladder base and mimicking like enlarged male prostate (A and B) (Female prostate sign).
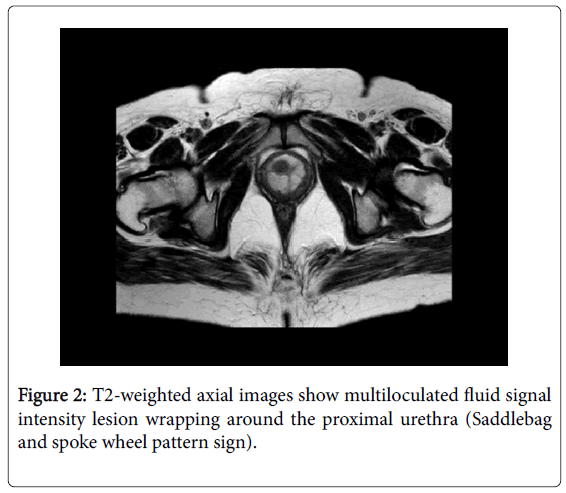
Figure 2: T2-weighted axial images show multiloculated fluid signal intensity lesion wrapping around the proximal urethra (Saddlebag and spoke wheel pattern sign).
There was diffusion restriction of contents and post contrast submucosal enhancement due to secondary infection and pus/infected contents. There was no evidence of any soft tissue enhancing lesion to suggest malignant transformation. On the basis of these radiological signs and imaging findings diagnosis of infected urethral diverticulum was made and confirmed on urethrocystoscopy (Figures 3 and 4).
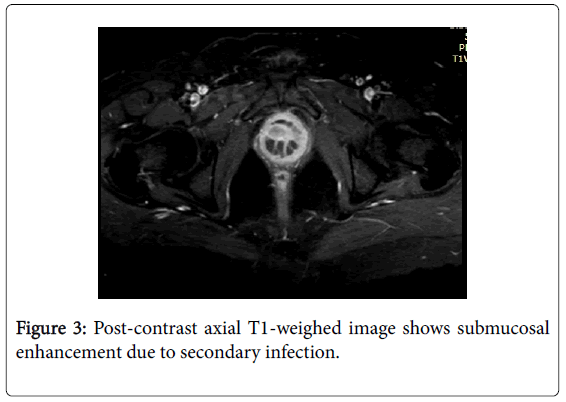
Figure 3: Post-contrast axial T1-weighed image shows submucosal enhancement due to secondary infection.
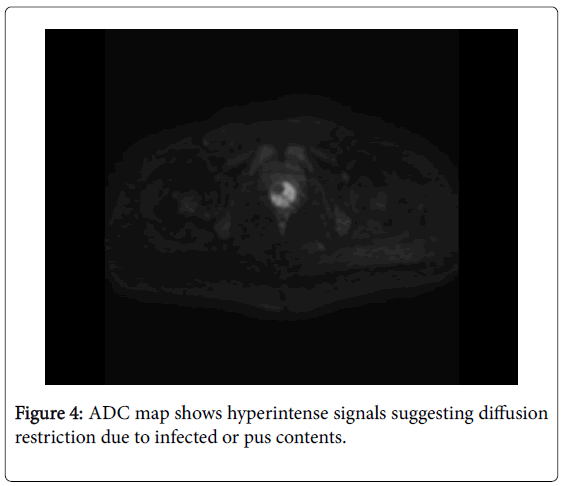
Figure 4: ADC map shows hyperintense signals suggesting diffusion restriction due to infected or pus contents.
Urethral diverticulum was historically described by William Hey in 1805 since then there is increasing trend of this condition in last few decades has been identified due to raised awareness among patients and physicians as well as increasing role of MRI in diagnosis of pelvic pathologies. A urethral diverticulum also known as urethrocele is described as single or multiple sacs like focal outpouching (s) arising from urethra as a result of paraurethral gland infection followed by obstruction of the duct, accumulation of pus and secretions in the gland that eventually ruptures the abscess into the urethral lumen [1]. Other less common causes are iatrogenic, birth process-related injuries to urethra and congenital origin from cloacogenic rests, Gartner duct, and müllerian duct cysts [2]. The urethral diverticulum is more common in the female population with an incidence of 1%-6% predominantly during 3rd to 5th decades of life due to an acquired course of disease with aging but they are also seen in children’s and neonates rarely [3].
The urethral diverticulum is well-defined and round to oval in shape, usually located in posterolateral mid or distal urethra and occasionally they are found at bladder base and neck region as in our case. The patient generally presents with non-specific lower urinary tract symptoms like frequency, urgency, recurrent infections and stress incontinence [3,4], earlier described as the triad of three D's e.g. Dysuria, Dyspareunia, and Dribbling. On clinical examination, they appear like cystic swelling arising from the anterior vaginal wall in few patients with discharging pus and hard/bleed on touch in case of complications. The urethral diverticulum is frequently complicated by infection, stone formation and foreign body, less commonly by malignant degeneration usually adenocarcinoma but also squamous cell and transitional cell carcinoma due to chronic irritation [5,6]. The differential diagnosis of a urethral diverticulum includes vaginal cyst, ectopic ureterocele, endometrioma, and neoplastic lesions [7]. This condition is treated with surgery and cannot be left alone due to increased morbidity especially among female patients. Excision is required and at times urethral construction may be needed in cases of a large diverticulum.
This condition is cumbersome to diagnose by conventional imaging techniques. Ultrasound, CT, and MRI are helpful diagnostic modalities for evaluation of urethral diverticulum, however, role of MRI is considered superior in making the accurate diagnosis, distinguishing it with other diagnostic differentials, assess the extent of disease and as a roadmap to surgery with information about location, number, size, configuration, and communication of the urethral diverticula [3]. MRI is more sensitive imaging technique over the complicated interventional procedures like voiding cystourethrography and doubleballoon urethrography for making the diagnosis of urethral diverticulum. MRI provides excellent soft tissue contrast and multiplanar details in presurgical evaluation of urethral diverticulum, particularly in the detection of narrow-neck obstructed urethral diverticula [8,9] and aid to diagnose other associated conditions like pelvic floor weakness on sagittal plane imaging without any radiation exposure to female pelvis in childbearing age, children and neonates with near 100% sensitivity [10,11].
Asymptomatic patients are evaluated on regular intervals and treated with antibiotics and anticholinergics to relieve the minimal symptoms [3]. Patients with progressive symptoms are managed surgically, the most common procedure is transvaginal diverticulectomy with good outcomes. Patients with symptomatic stress urinary incontinence are evaluated by uroflowmetry studies prior to surgery because of associated urinary retention in few cases [12]. Limitation of MRI is restricted to define multiple urethral diverticula from a septated urethral diverticulum and ultrasonography is particularly helpful in such condition [2,3].
We are redefining the importance and role of MRI imaging and sharing few helpful radiological signs of urethral diverticulum on MRI imaging solely in this article that are easy to identify, permits a confident diagnosis on the basis of imaging findings alone and helps to narrow down the differential diagnosis. The female prostate sign is described as fluid containing multiloculated female urethral diverticula in proximal urethra elevating the bladder base in similar manner to enlarged male prostate on T2-weighted sagittal planes and multiloculated diverticulum wrapping urethra like water bags called as saddle bag and spoke wheel signs in axial T2-weighted planes.