Journal of Bone Research
Open Access
ISSN: 2572-4916
ISSN: 2572-4916
Case Report - (2018) Volume 6, Issue 2
Fibrous Dysplasia is a very rare, but debilitating condition. Symptomatic corrective surgical interventions like bone graft have a lifespan and need revision surgeries after 30-36 months. We propose the possible use of autologous cultured osteoblast cell therapy; proven effective in our experience. We present a case report of successful treatment of monostotic fibrous dysplasia in a young male with autologous cultured osteoblast cell therapy and follow up for 60 months.
Keywords: Fibrous dysplasia; Osteoblast; Cell therapy; Osseous tissue integration; Bone qualityÂ
Fibrous Dysplasia (FD) is a result of a non-hereditary, non-sense, spontaneous mutation, leading to an abnormal proliferation of fibroblasts and increased bone resorption by osteoclasts. The genetic reason may also be associated with hormonal imbalance.
The genetic theory of FD postulates that somatic mutation early in embryonic life causes gene mosaicism. This spontaneous mutation in the gene (GNAS I) results in a cascade which may lead to alteration in cellular differentiation and osteoblastic proliferation [1]. Mutated cells proliferate and replace the normal bone marrow with a generally under-mineralized and abnormal fibro-osseous tissue [2,3]. Though the pathology is benign, the medullary bone is replaced by immature bone and fibrous stroma. Most often, the disease is detected by the third decade of life and may be silent until then.
There is either single bone involvement (monostotic)) constituting >70% of diagnosed cases [4] or more than one bone involvement (polyostotic). Monostotic lesions tend to remain active only until skeletal maturity, whereas polyostotic lesions may progress during adulthood warding off the need for early surgical intervention in younger patients with monostotic lesions [5]. The overall prevalence is rare, with one identified case in about 30,000 people [6].
Signs and symptoms
Patients generally present with significant disability due to bone deformity and neurologic compression. The clinical presentation includes pain and swelling with an antalgic gait. Patients may also present with limb length discrepancies and also pathologic fractures in some cases. Tibial bowing, bossing of skull, prominent jaws, rib and chest masses are few other symptoms.
• Patients tend to see the physician if they repeatedly suffer from conditions like
• Bone pain that increases with weight-bearing activity or does not go away with rest
• Bone pain that interrupts sleep
• Difficulty in walking or limping
• Unexplained swelling
• Changes in bone shape
• The difference in limb length
Regardless of the type of FD, associated lifetime risk of malignant transformation is about 1 to 4% [7,8]. Other possible complications reported are bone deformity and fractures due to bone weakening, vision/hearing impairment (nerves getting compressed due to affected bone), and arthritis (leg/pelvic bone affected) [5].
Diagnosis
Primary diagnosis can be based on X-ray that identifies a typical FD lesion as “ground-glass” appearance [9]. This also gives a clear idea of the size of the lesion.
A CT and/or MRI scan can support and confirm the diagnosis. Imaging also indicates any other pathology in the same region. Nuclear imaging for diagnosing or for ruling out the involvement of multiple bones/lesions is also performed. Histopathology is recommended for final confirmed diagnosis.
Treatment
The aim is to relieve pain, discomfort. Until confirmed diagnosis, the patient can be managed with NSAIDs and other pain relieving approaches like restricted activity, etc.
After confirmed diagnosis, surgery for excision of injured/lesioned bone and/or correction of bone length discrepancy is planned. The lost/excised bone is generally replaced with either autologous or allogenic/ cadaver donor bone graft.
Bisphosphonates (Alendronic acid/Zolendronic acid) are prescribed for strengthening bone [10]. Along with the inhibitory effect on osteoclasts, some studies suggest that these drugs may also have a stimulating effect on osteoblasts [9].
The major limiting factor in the use of bone grafts, regardless of whether it is autologous or allogenic, is that the life of the graft is relatively short. It gets absorbed, probably by the surrounding mutated cells; and patients again start having typical symptoms of FD. Thus, in most of the patients, the surgery and grafting are required to be repeated after 30-36 months [11].
The cellular pathology of FD
Marie, et al [12] in their work on the molecular basis of the alterations in bone cells and bone matrix in FD, found the mutations affecting the stimulatory alpha subunit of G protein (Gsalpha) in dysplastic bone lesions. The histological analysis of dysplastic lesions revealed that the mutations in Gsalpha cause abnormalities in the osteoblastic lineage cells and therefore in the bone matrix. Further in vitro analyses of bone cells from mutant dysplastic bone lesions revealed that the abnormal deposition of the immature bone matrix was the result of decreased differentiation and increased proliferation of osteoblastic cells. In turn, the signaling pathway involved in these osteoblastic abnormalities affects the transcription and expression of downstream genes and results in the alterations of osteoblast recruitment and function. Considering this fact, the reabsorption and/or disappearance of the bone graft used as a treatment for FD is perpetual [11]. The continued hyperplastic osteoblastic activity, despite the healthy graft, will lead to continuous osteoclastic absorption of bone. This necessitates repeated grafting within 30-36 months.
Cell-based Regenerative approach hypothesizes that if a large number of cultured and characterized osteoblast cells replace the excised fibrous dysplastic bone, then the fresh healthy cells will outgrow the diseased cell population. Depending on the size of the fibrous bone, antigen negative cadaver bone can be used simultaneously, if needed.
A 20 male, with all normal activities, started complaining of pain and limp while walking and eventually abnormal gait became obvious. The patient was traveling 25 km daily for his work.
Upon radiology and CT, a provisional diagnosis of FD was made. Excision surgery and bone autograft were suggested, with an assumption of complete relief within 6 months. The patient underwent the procedure and resumed normal activity and work within 15 months.
By the end of three years from the first presentation, the patient returned with the same symptoms, i.e., pain while walking, limping and abnormal gait. Patient approached the same team of treating orthopedicians who performed the earlier graft surgery. Radiology revealed recurrence of the lesion of similar size as before, with a pathological fracture in the inferior cortex of the neck. The physician suggested a repeat of bone autograft, the need of which was not clearly mentioned to the patient during the earlier surgery. Despite repeat counseling, the patient was not willing to undergo autograft as he was not convinced of losing another part of the bone from the donor site. The patient wanted to seek a second opinion and approached our hospital team.
The CT scan revealed fairly well-defined, multi-locular cystic, mildly expansile lesions measuring about 2.6×4.7×8.2 cm3 in AP, TR and vertical dimensions at the right femoral neck, intertrochanteric region, and adjacent proximal shaft (Figure 1). The lesion had a thick sclerotic rim. There is a cortical break along the inferior right femoral neck suggestive of a non-displaced fracture.
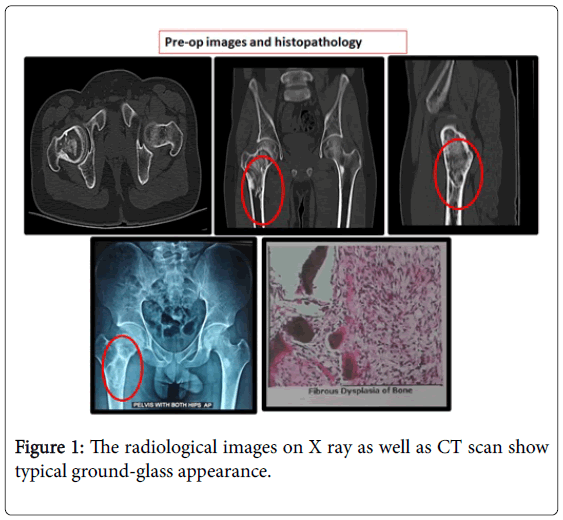
Figure 1: The radiological images on X ray as well as CT scan show typical ground-glass appearance.
Our team also suggested bone graft, maybe an allograft or cadaver. But, the patient was quite apprehensive, now knowing the limitation of this procedure.
After a lot of discussion and deliberation, and patient’s full informed consent, we decided to perform a cadaver bone graft (antigen-free) along with implant of autologous, live, cultured osteoblast cells (OSSGROWTM; Regrow Biosciences Pvt Ltd, India, RBPL).
OSSGROWTM biopsy, culture and implant procedure
• Around 4 ml bone marrow was aspirated from the iliac crest.
• It was shipped to RBPL’s Cell Processing Centre (CPC) under specified conditions.
• The bone marrow was processed at RBPL’s CPC to obtain a live culture of osteoblast, not less than 12 million per vial. Cultured osteoblast cells were characterized to ascertain the specificity and purity along with other quality checks. The culture process involved isolation of mesenchymal stem cells from bone marrow as adherent cells, followed by differentiation into osteoblast lineage in the presence of L-ascorbic acid and M Dexamethasone. The medium was changed every 4th day. On day 35, the activation of alkaline phosphatase in the culture was confirmed following the standard staining method. Once confirmed, the cells were washed and incubated in 0.02% Trypsin-EDTA for 5 minutes. This activity was stopped using culture medium, all contents collected in the conical tube to obtain a pellet of desired cells. Four vials, each containing not less than 12 million osteoblast cells, were prepared.
• This patient-specific, personalized cell therapy product was received at our Hospital.
• During Implant, multiple cavities and the fibrous, dysplastic bone tissue was completely debrided until a bleeding bone was exposed.
• The cadaver-graft was placed in three layers with the cell dose instilled in between the layers.
• Then the area was covered with a sufficient quantity of fibrin glue and gravity dependent position was maintained for 8-10 min.
• The wound was closed following routine techniques and procedures.
Post-op care
The patient was advised to rest for a week with routine physiotherapy sessions. Then for 6 weeks of minimum activity, use of a walker and self-administered exercise were advised. Non-weightbearing mobilization was allowed after 6 weeks. The affected leg was supported, and gradual weight-bearing was allowed by week 10 depending on periodic X-ray findings.
Follow-up
12-months post-implantation, the patient is totally active, working on the farm, riding a two-wheeler, with no complaint (Figure 2). Radiology data and clinical evidence over a period of 24 months clearly showed the integration of osseous tissue.
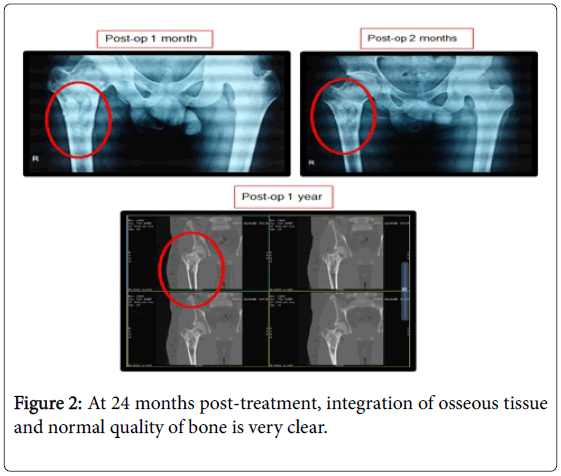
Figure 2: At 24 months post-treatment, integration of osseous tissue and normal quality of bone is very clear.
At 60 months, we report complete integration of bone graft, satisfactory bone quality in the metaphyseal neck of femur and no evidence of an osteolytic lesion (Figure 3).
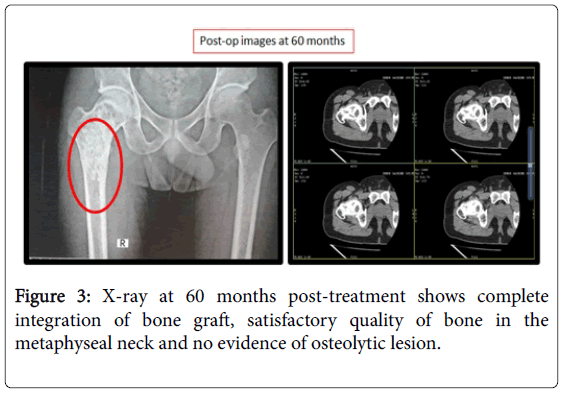
Figure 3: X-ray at 60 months post-treatment shows complete integration of bone graft, satisfactory quality of bone in the metaphyseal neck and no evidence of osteolytic lesion.
The major limiting factors associated with the autologous or allogenic bone grafting were studied by Leet et al. [11] in a cohort of patient with polyostotic FD. On the other hand, the use of synthetic biomaterial can produce adverse events like inflammation and foreign body reaction, thereby, affecting osseointegration and bone formation. Autologous osteoblast lineage cells implanted directly or seeded on to the allograft or biomaterial prior to implantation proved to be efficient for various bone defects [13,14]. In a randomized trial, autologous osteoblastic cells proved to have a phenomenal effect in the treatment of non-traumatic osteonecrosis of the femoral head compared to implantation of bone marrow concentrate containing mesenchymal stem cells [15]. However, the application of osteoblast cells in FD treatment has not been proved clinically yet. However, in a pre-clinical study, the over-activity of Gsα in osteoblasts appears to be a marked increase in bone mass [16]. Hence, the treatment with live osteoblast cells of autologous origin seems to be a promising option to overcome the challenges involved in FD treatment. To the best of our knowledge, our study is first of its kind where we have successfully used autologous live osteoblast cells in the treatment of FD. After complete debridement of the lesion, we have carefully grafted the osteoblast cells and observed no recurrence of FD over a period of five years. An augmented quality of bone with no evidence of osteolytic lesion was found in this study. However, multi-centric clinical trials involving more number of patients are required to validate the safety and efficacy of this method.
The Medical Team of Ranka Hospital acknowledges RBPL for making the personalized autologous cultured live osteoblast (not less than 48 million) for treatment.
Authors have no conflict of interest to declare.