Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 4
Objective: To report a unique case of fluoxetine overdose leading to serotonin syndrome with auditory and complex visual hallucinations. This case also demonstrates serotonin syndrome may mimic a Parkinsonian syndrome, which is poorly described in the literature.
Case Summary: A 65-year-old gentleman, undergoing evaluation for possible Parkinsonian syndrome with bradykinesia and rigidity presented to the emergency department with additional complaints of weakness, fatigue, flushing, and complex visual and auditory hallucinations. Chart review revealed he was unintentionally overdosed with fluoxetine to a total daily dose of 160 mg. Examination revealed tachycardia, diaphoresis, significant mydriasis, and visual hallucinations. Initial workup was unremarkable. Poison control recommended discontinuation of the fluoxetine and in follow up he reported resolution of all symptoms.
Discussion: This case describes serotonin syndrome as the result of chronic fluoxetine overdose masquerading as a Parkinsonian syndrome. This patient also experienced auditory and visual hallucinations that resolved with cessation of fluoxetine, adverse effects which are relatively uncommon. The likelihood the patient’s symptoms were the result of fluoxetine intoxication is probable, as assessed by the Naranjo Adverse Drug Reaction (ADR) probability scale.
Conclusions: Chronic fluoxetine overdose can lead to serotonin syndrome, as well as, several rare adverse effects including a Parkinsonian syndrome, complex visual, and auditory hallucinations. A high index of suspicion is necessary for diagnosis of serotonin syndrome, particularly in mild cases. Most cases can be prevented with careful medication reconciliation.
<Keywords: Fluoxetine; Selective Serotonin Reuptake Inhibitor (SSRI); Serotonin syndrome; Complex visual hallucination; Auditory hallucination; Parkinsonian; Adverse Drug Reaction (ADR)
Serotonin Syndrome (SS) is characterized by a spectrum of changes in mental status, neuromuscular dysfunction, and autonomic instability. It is associated with increased serotonergic activity in the central nervous system and is a potentially life threatening condition. It is largely preventable by responsible prescribing practices and proper patient education. A number of drugs from different classes are implicated in the development of SS, including antidepressants such as fluoxetine. Most cases are reported in patients taking more than one serotonergic medication, however, overdose on a single agent can lead to SS [1].
A 65-year-old gentleman, undergoing outpatient neurology evaluation for possible Parkinsonian syndrome for symptoms of rigidity and bradykinesia presented to the emergency department with additional complaints of six weeks of weakness, fatigue, flushing, and complex visual and auditory hallucinations. His past medical history was notable for depression. He received his medications for a mail order pharmacy. Chart review revealed he was originally prescribed 20 mg fluoxetine tablets, taken as two tablets by mouth twice daily, which was changed to 40 mg tablets unbeknownst to him. This resulted in unintentional overdose with a total daily dose of 160 mg. The patient denied deliberate overdose or suicidal ideation. He had no known history of substance abuse.
Physical and mental status examination at the time of admission revealed tachycardia, diaphoresis, significant mydriasis, and visual hallucinations. His blood pressure was slightly elevated but stable. Laboratory studies showed normal CBC, TSH, BMP, and LFTs. An ECG was unchanged from prior exams with a QTc at the upper limit of normal. Urine drug screen and serum ethanol levels were negative. Serum fluoxetine or nor-fluoxetine levels were not obtained. Poison control recommended discontinuation of the fluoxetine and observation. With improving symptoms, he was discharged following several days of observation. In follow up four weeks later, he reported resolution of all symptoms, including rigidity and bradykinesia. He was not restarted on any antidepressant medications. The likelihood of the patient’s symptoms being the result of fluoxetine intoxication is probable, as assessed by the Naranjo Adverse Drug Reaction (ADR) probability scale.
Serotonin Syndrome is typically an iatrogenic phenomenon caused by medications that affect serotonin transport, signaling, and metabolism [1]. A high level of suspicion is necessary for diagnosis, especially in mild cases [2,3]. The incidence of SS appears to be increase in, [4-7] which may reflect increased use or availability of drugs that affect serotonin or increasing provider awareness. Still, many cases go unrecognized, and there is no national reporting mechanism making the true incidence difficult to determine [4]. The committee on identifying and preventing medication errors estimates that adverse drug events cost at least $3.5 billion annually, many of which are thought to be preventable in the ambulatory setting [8].
The clinical presentation of SS is highly variable. However, the diagnosis is suggested by the constellation of autonomic instability, neuromuscular signs, and mental status changes in the setting of serotonergic medications (Figure 1). Several diagnostic criteria have been developed for use in clinical practice including sternbach’s criteria and the hunter serotonin toxicity criteria. Diagnosis via the Hunter criteria is based on decision rules requiring the presence of a feature or group of features, such as inducible clonus with agitation or tremor with hyperreflexia (Figure 2) [10]. Sternbach’s requires at least three of ten clinical features with a recent addition or increase in an offending medication (Figure 3) [11]. Hunter’s Criteria may be a more useful diagnostic tool, as it is both more sensitive and specific than Sternbach’s [4].
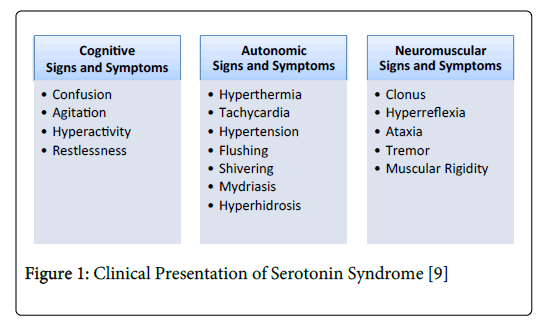
Figure 1: Clinical Presentation of Serotonin Syndrome [9]
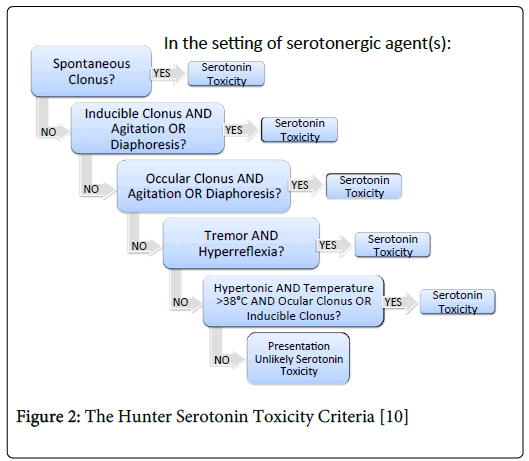
Figure 2: The Hunter Serotonin Toxicity Criteria [10]
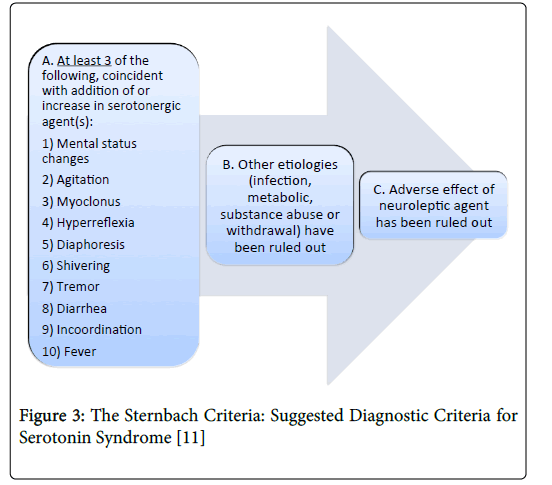
Figure 3: The Sternbach Criteria: Suggested Diagnostic Criteria for Serotonin Syndrome [11]
Onset of SS is usually rapid, often within six hours of medication ingestion or dose changes. However, patients with mild serotonin syndrome may present with subacute or chronic symptoms [2]. Medications from many classes can cause SS when taken in combination [4,12]. Selective Serotonin Reuptake Inhibitors (SSRIs) are known to cause serotonin syndrome when taken alone in large overdoses [13]. However, this case highlights that relatively mild, chronic overdose with fluoxetine may also lead to SS. Fluoxetine alone leading to SS at therapeutic or slightly supra-therapeutic doses is reported in only a few cases in the literature [14,15]. Patient specific factors can also increase risk for developing the syndrome. Endothelial damage mediated by hypertension, diabetes, and atherosclerosis, may lead to decreased production of MAO-A [2] or nitrous oxide [16] increasing the risk of SS through up regulation of serotonin signaling. Medications that inhibit the cytochrome P450-2D6 or 3A4 enzymes used in combination with an SSRI can increase the risk for SS [4]. Fluoxetine, in particular, has a long half-life and is a potent inhibitor of the CYP2D6 enzyme, which can increase the production of serotonin metabolites [2]. Interestingly, our patient was on long-term oxy codone therapy, which has been shown to increase release of serotonin in the forebrain and may increase the risk of SS [17,18].
The differential diagnosis includes infection, metabolic disorders, anticholinergic toxicity, dopaminergic or sympathomimetic overdose, malignant hyperthermia, neuroleptic malignant syndrome, heat stroke, serotonin-secreting tumor, and substance use or withdrawal [2,4]. The initial evaluation should focus on investigating these possibilities. A complete medication history that includes all non prescription medications, supplements, and illicit drugs should be obtained. Laboratory and imaging studies may be necessary to evaluate for infection or endogenous sources of hormone or neuropeptide excess. First-line treatment includes discontinuation of the suspected agent and supportive care. Most mild cases resolve in one to three days and do not require hospitalization. Patients with more severe symptoms should be monitored in an inpatient setting. Agitation and tremor can be treated with benzodiazepines. Patients with life threatening symptoms may require critical care including sedation, neuromuscular paralysis, and intubation. Cyprohepatidine, a serotonin 2A antagonist, is often widely used despite a lack of strong evidence for its effectiveness in SS [4].
This case also illustrates an uncommon side effect of SSRI medications. Though SSRIs are known to improve psychotic features in some patients with schizophrenia and psychotic depression, this case highlights paradoxical development of hallucinations with fluoxetine [19]. Auditory and Complex Visual Hallucinations (CVH) are rare adverse effects with ingestion of SSRIs, including fluoxetine, sertraline, fluvoxamine, paroxetine, and citalopram that are most often presented as case reports in the literature [19-23]. Several mechanisms have been proposed to explain the development of hallucinations in this setting. Postsynaptic 5-HT2 and 5-HT3 receptor signaling may play a role in the ventral striate and mesolimbic regions of the brain, with signaling mediated by dopamine and serotonin [19,22]. In the setting of CVH, another proposed mechanism is an imbalance between serotonin and acetylcholine signaling, with relative serotonin excess and acetylcholine deficit [20,22]. Finally, stimulation of high affinity sigma receptors in the hippocampus may be involved. Interestingly, CVH have also been reported upon discontinuation of fluoxetine therapy [18].
Additionally, this case suggests serotonin syndrome may masquerade as a Parkinsonian syndrome. Our patient’s Parkinsonian symptoms coincided with increased fluoxetine dose and resolved following its discontinuation. Parkinsonism in the setting of serotonin syndrome is poorly described in the literature.
Serotonin syndrome is a potentially life threatening condition with a highly variable clinical presentation, which may include hallucinations and mimic a Parkinsoninan syndrome. The increasing number of patients taking serotonergic medications makes provider recognition important to avoid unnecessary testing and potential morbidity and mortality. Most cases can be prevented with careful medication reconciliation.