Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2013) Volume 2, Issue 1
Background: Chronic kidney disease (CKD) results in complex endocrine and metabolism alterations including thyroid dysfunction. There is many mechanisms explained the link between thyroid and kidney disease, both of them affect each other, plus both consider as an independent factor for cardiovascular disease.
Aims: We investigate the prevalence of morphological and functional discarder in CKD maintained on hemodialysis and it relation to dialysis duration.
Study design and method: A cross section study included 60 CKD patient maintained on HD and 40 control subjects. All subject investigated with thyroid ultrasound and thyroid hormone screen including serum thyroxine (T4), Triiodothyronin (T3), Thyroid stimulating hormone (TSH), free T3, free T4, Thyroglobulin antibodies (TG Ab) and Thyroid peroxidase antibodies (TPO Ab).
Results: HD patients had a higher prevalence of diffuse goiter than control subjects (26.7% versus 10%, p=0.045), we compared the prevalence of thyroid function disorders between the two group which showed significant high frequency of low T3 syndrome in HD group. The mean duration of hemodilaysis was not significantly correlated with mean thyroid volume and TSH level (r=-0.06, r=0.13) respectively. While there was positive correlation between TSH level and mean thyroid volume among HD patients (r=0.25 p<0.05).
Conclusions: We concluded that CKD patients maintained on HD were associated with higher prevalent thyroid function and morphology disorders in compared with healthy subjects.
<Keywords: Chronic kidney disease; Hemodialysis; Thyroid hormone
It is common that chronic kidney disease (CKD) exhibits multiple endocrinal and metabolic disorders. One of the most important endocrinal disorders which occur in CKD patients are thyroid dysfunction. As a matter of fact, the diagnosis and treatment of patients with clinical thyroid disorders are not difficult for physician, while diagnosis of subclinical presentation of thyroid disorders are not always an easy task especially in patients with CKD which may be complicated by renal replacement therapy modality and comorbidity.
For many decades, it has been known that there is an interaction between kidney and thyroid gland. Thyroid hormones (TH) are essential for the development and growth of kidney, water and electrolyte homeostasis and maintenance of renal blood flow. While, kidney is included in thyroid hormones metabolism and elimination [1,2].
Deterioration of renal function leads to disturbance in synthesis, secretion, metabolism and degradation of thyroid hormones which are presented with different clinical syndromes of thyroid dysfunction [3]. The Level of serum thyroid stimulating hormone (TSH) is usually normal or elevated in CKD, but there is reduced response to its releasing hormone (TRH) [4]. In addition, there is a disturbed circadian rhythm of TSH and TSH glycosylation [5].
Impaired kidney function is not only has an effect on thyroid gland function but also alters thyroid structure. A higher prevalence of goiter is recorded in CKD patients specially women [6]. In addition, Miki et al. [7] reported that thyroid nodules and cancer are more common in CKD and after kidney transplantation of patients who had hyperparathyroidism compared with general population; this might be due to disturbed cellular immunity during dialysis and influence of the immunosuppressive drugs.
The decline in the glomerular filtration leads to disturbance of iodine clearance with elevation of serum inorganic iodine that may potentially block synthesis of thyroid hormones (Wolf-Chaikoff effect), which explain the higher prevalence of diffuse goiter and hypothyroidism in hemodialysis patients [8].
We investigated the prevalence of thyroid morphological changes and hormonal dysfunction in hemodialysis patients and if there is an association between the dialysis duration and thyroid disorders.
A Cross section observational single center study was carried out in Nephrology Unit of Internal Medicine, Zagazig University Hospital from June 2012 to September 2012.
One hundred subjects were enrolled in this study. They included 60 stable CKD patients on chronic hemodialysis treatment with different primary causes of renal failure, with mean duration of hemodialysis therapy 74.25 ± 38.13 months. All patients were clinically stable and free of active infections, autoimmune diseases and previous thyroid disorders and were not taking drugs that could affect thyroid hormones level. Hemodialysis was performed thrice weekly, four hours per session, with standard bicarbonate dialysis using a single-used low-flux polysulfide hemodialyzer with a membrane surface area of 1.3 m2-1.6 m2. Forty healthy subjects (healthcare workers) volunteered as control subjects. All were on a regular diet and did not have any history of hypertension, diabetes mellitus, renal disease or thyroid disorders.
The etiology of end stage renal disease (ESRD) in hemodialysis patients was as follow: ESRD of unknown etiology (n=27), diabetic nephropathy (n=14), hypertensive kidney disease (n= 9), chronic GN (n=3), polycystic kidney disease (n=1), lupus nephritis (n=2), obstructive uropathy (n=3) and graft dysfunction (n=1). The Creatinine Clearance (CrCl) (ml/min) was calculated by the Cockcroft-Gault formula as (140 − age) × body weight/plasma creatinine × 72 (× 0.85 if female) [9].
In all hemodialysis (HD) patients, blood was drawn in the morning before the onset of the dialysis session (and heparin administration). Samples were aliquot, and serum was stored at -40°C before assay. Tri-iodothyronin (T3), thyroxin (T4), free T3, free T4, Thyroid peroxidase antibodies (TPO Ab) and Thyroglobulin antibodies (TG Ab) were assessed by radioimmunoassay (RIA). TSH was measured by chemiluminescence immunometric assay (IRMA).
Ultrasound examination of the Thyroid gland was performed, with 7.5 MHz probe and 50 mm linear transducer, in the same day or the day after which blood samples were taken for hormonal assay. The total thyroid volume was measured by the sum of lobes volumes. The volume for each lobe was calculated by the following formula; V=a × b × c × n/6. In this formula n/6 represents the correction factor measuring 0.479 [9]. After that we evaluated the thyroid as a regard the echogenicity, vascularity and the presence of nodules.
According to laboratory and ultrasonography results, we defined subclinical hypothyroidism as a mild TSH elevation >4.4 mIU/L in patients with normal serum thyroxin level [10]. Hypothyroidism is an elevation in TSH>10 mIU/L with reduced T3 and T4 levels [10]. Low T3 syndrome is a reduced T3 level<0.89 nmol/L [4]. Diffuse goiter is an elevated thyroid volume >20 ml [11], and nodular goiter is the presence of one node in any of thyroid lobe, while multinodular goiter is the presence of two or more nodules in thyroid lobes [10]. Lastly, Hashimoto thyroiditis characterized by heterogeneous hypoechoic gland with echogenic septa and increased vascularity associated with elevated thyroid antibodies (TG Ab, TPO Ab) [12].
The study protocol was approved by the ethical committee of zagazig university hospital. The study was conducted according to the Declaration of Helsinki 1975, and informed consent was taken from all patients prior to participation in the study.
Mean standard ± deviation (SD) and percentages were used for summarizing the data. Statistical differences in the variables were tested using Student’s t-test for comparing mean values of the two groups. The relationship between tested variables was assessed using Spearman correlation coefficients. All analyses were conducted using the Statistical Processing Package for Social Science (SPSS) version 16 for Windows.
Basic laboratory characteristics of the HD group (60 subjects) and Control group (40 subjects) are shown in Table 1. The mean age did not significantly differ between the two groups, while BMI, GFR and Hgb level showed highly significant difference between the two groups. There were no statistically significant differences between these groups in mean values of T4, TSH, free thyroid hormones, TG Ab and TPO Ab (p>0.05).
| Variables | HD group (No.:60) | Control group (No.:40) | P values |
|---|---|---|---|
| Age (yr) | 51.88 ± 11.75 | 48.54 ± 7.63 | 0.111 |
| Gender (Male/female) | 27/33 (45% /55%) | 20/20 (50% /50%) | 0.685 |
| BMI (kg/m2) | 22.68 ± 2.19 | 25.83 ± 3.95 | <0.001 |
| HD duration(mo) | 74.25 ± 38.13 | - | - |
| S. Creatinine (mg/dl) | 7.9 ± 2.42 | 0.9 ± 0.25 | <0.001 |
| CrCl (ml/min) | 11.36 ± 1.89 | 68.14 ± 42.50 | <0.001 |
| S. Albumin (g/dl) | 3.72 ± 0.95 | 4.65 ±0.72 | <0.001 |
| Total Protein (g/dl) | 5.9 ± 1.2 | 7.2 ± 0.6 | <0.001 |
| Hgb (g/L) | 93.1 ± 15.2 | 134.8 ± 9.7 | <0.001 |
| T3( nmol/L) | 1.28 ± 0.55 | 1.65 ± 0.35 | < 0.001 |
| T4 (nmol/L) | 80.61 ± 15.58 | 86.12 ± 24.73 | 0.174 |
| TSH (mIU/ml) | 3.01 ± 2.73 | 2.77 ± 1.84 | 0.627 |
| Free T3 (pmol/L) | 5.14 ± 2.49 | 5.90 ± 1.37 | 0.081 |
| Free T4 (pmol/L) | 14.25 ± 3.96 | 14.38 ± 4.01 | 0.873 |
| TG Ab (IU/ml) | 20.74 ± 28.03 | 15.24 ±10.78 | 0.239 |
| TPO Ab (IU/ml) | 18.67 ± 12.49 | 18.11 ± 12.67 | 0.827 |
Table 1: Characteristic parameters of study Subjects.
HD patients had a higher prevalence of diffuse goiter than control subjects (26.7% versus 10%, p= 0.045), Also there was high frequency of nodular goiter and Hashimoto thyroiditis among HD patients (Table 2; Figure 1).
| Morphology disorders | HD group (No:60) | Control group (No:40) | p values | ||
|---|---|---|---|---|---|
| No | % | No | % | ||
| Without disorders | 29 | 48.3 | 33 | 82.5 | <0.001 |
| Nodular goiter | 9 | 15 | 2 | 5 | 0.191 |
| Diffuse goiter | 16 | 26.7 | 4 | 10 | 0.045 |
| Hashimoto | 6 | 10 | 1 | 2.5 | 0.237 |
Table 2: Frequency of thyroid morphology disorders among the groups.
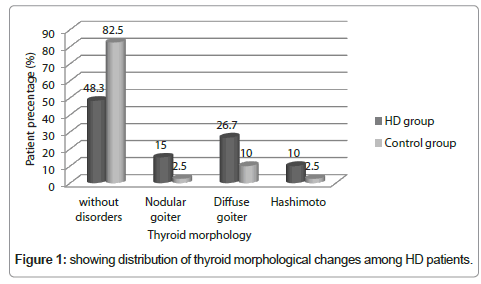
Figure 1: showing distribution of thyroid morphological changes among HD patients.
We compared the prevalence of thyroid function disorders between the two groups (Table 3) which showed significant high frequency of low T3 syndrome in HD group, moreover Subclinical hypothyroidism and low T4 syndrome were more frequent in HD patients; but nonsignificant.
| Thyroid function disorder | HD group (No:60) | Control group (No:40) | p values | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Without disorder | 35 | 58.4 | 34 | 85 | 0.007 |
| Low T3 syndrome | 8 | 13.3 | 0 | 0 | 0.020 |
| High T4 syndrome | 0 | 0.0 | 1 | 2.5 | 0.400 |
| Low T4 syndrome | 2 | 3.3 | 0 | 0.0 | 0.515 |
| Subclinical hypothyroidism | 11 | 18.3 | 2 | 5 | 0.069 |
| Clinical hypothyroidism | 3 | 5 | 1 | 2.5 | 0.647 |
| Subclinical hyperthyroidism | 1 | 1.7 | 2 | 5 | 0.562 |
Table 3: Frequency of thyroid functional disorders among the groups.
The mean duration of hemodilaysis was not significantly correlated with mean thyroid volume and TSH level (r= -0.06, r= 0.13) respectively. While there was positive correlation between TSH level and mean thyroid volume among HD patients (r=0.25, p<0.05).
For many decades, it has been known that there is an interaction between kidney and thyroid. In addition, the varieties of renal replacement therapy have a profound effect on thyroid function, which is very important to be known by both nephrologist and endocrinologist for optimal early diagnosis and perfect patient management.
We observed high prevalence of thyroid morphology abnormalities (51.7%) in HD patients. Moreover, Mean values of thyroid volume in HD group was significantly higher than control group (19.36 ± 4.03 vs. 11.17 ± 3.98 ml, p<0.0001). Therefore, diffuse goiter was highly frequent in HD patients compared with control group (26.7% vs. 10%, p=0.045). But Nodular goiter in our results was not significantly higher in HD group compared with control group (15% vs. 5%, p=0191). The explanation of high prevalence of diffuse and nodular goiter is unclear; it might be a result of presence and/or retention of goitrogens by kidney or disturbance in iodine metabolism that lead to excessive accumulation of iodine which subsequent increased TSH stimulation. These findings are in agreement with Jusufovic and Hodzic [13], who reported that 35% of patients on HD have diffuse goiter while multinodular goiter was more frequent in patient with duration of hemodialysis therapy less than 72 months.
There was no significant correlation between thyroid morphology, function disorders and duration of dialysis, sex nor age in HD patients. This is concurrent with Kutlay et al. [14] and Lebkowska et al. [15] who observed that there is no relationship between duration of dialysis treatment and abnormalities in the morphology of the thyroid gland. In contrast, Kaptein [16] found a higher incidence of diffuse goiter with increased length of hemodialysis treatment. Also Lin et al. [17] in their study examined the effect of the duration of peritoneal dialysis on thyroid nodules, they recorded that there was an increased incidence of nodular goiter among patients with longer duration of continuous ambulatory peritoneal dialysis (CAPD) (51.6 ± 42.9 months).
Regarding thyroid function disorders, we observed significant decrease in mean level of serum T3 in HD patients compared with healthy control subjects. Low T3 syndrome and subclinical hypothyroidism are the most frequently observed thyroid dysfunction in our HD patients which represented (13.3% and 18.3% respectively). Moreover, there was a high level of mean values of thyroid antibodies among hemodilaysis patients but not significant. These findings are consistent with those of Jusufovic et al. [18] who studied the effect of anemia of uremia on thyroid gland function and morphology, they observed high prevalence of low T3 syndrome especially in HD patients whose hemoglobulin level <125 g/L.
The relationship between low T3 and cardiovascular mortality in euthyroid CKD patients has been proven [19]. In addition, it has been observed that low T3 syndrome in uremic patient before kidney transplantation is associated with decrease in graft survival [20]. Saito et al. [21] observed that low T3 syndrome in HD patients was associated with body volume disturbance which increases the risk of pulmonary edema and cardiovascular complications. Moreover, total and free T3 behave as survival markers in patients with CKD both in HD [22,23] and in peritoneal dialysis (PD) [24]. Therefore, some authors recommended measuring Total T3 level in uremic patients to decrease risk of mortality and graft failure.
There are various factors that may contribute to the reduction in T3 level in uremic patients, including malnutrition and reduction in peripheral production of T3 by inflammatory mediators like TNFα and interleukin-1 which inhibit the expression of type 1 5’-deiodinase, the enzyme responsible for T4 to T3 conversion in peripheral tissues. This could explain how chronic inflammation and vascular damage associated with CKD interfere with the normal process of T3 synthesis from T4 [19,22,24].
Our study has some limitations which have to be discussed before drawing conclusions. First, the cross-sectional design of the study in which diagnosis of thyroid dysfunction has been depended on one blood sample that lacking thyroid function tests follow up. Second, limited sample size enrolled in our study, so the relationship between thyroid gland and CKD should be further examined in a prospective study with a large number of subjects. However, to our knowledge, this is the first study conducted among Egyptian HD patients regarding thyroid dysfunction and morphological changes.
One of the more significant findings to emerge from this study is the presence of high prevalence of low T3 syndrome and subclinical hypothyroidism among HD patients, which may be a significant contributing factor in the early development of cardiovascular complications occurring in HD patients and raise the mortality rate among them. So, we recommend a periodic screening of thyroid function and structure in CKD patients especially who maintained on HD therapy.