Andrology-Open Access
Open Access
ISSN: 2167-0250
ISSN: 2167-0250
Research Article - (2015) Volume 4, Issue 1
Objective: The aim of this study was to test the association of CYP1A1 gene T6235C polymorphism with Polycystic Ovary Syndrome (PCOS). Methods: In a case control study, 100 women with PCOS (Rotterdam criteria) and 100 ages matched healthy controls were enrolled and compared with respect to CYP1A1 T6235C polymorphism. The clinical, biochemical and Sonographic parameters of wild type (TT), heterozygous (TC), and homozygous mutant (CC) genotypes in PCOS women were compared with that in controls. Results: The risk ratio of bearing TC genotype was 1.3327 (p=0.32), and CC genotype was 2.6084 (p=0.14) in women with PCOS on the whole. However in PCOS women with the Sonographic presence of Polycystic Ovaries (PCO), the risk ratio became significant for TC genotype (OR=1.872; p=0.04) but not for CC genotype (OR=4.05; p=0.08). There was also a significant association of TC and CC genotypes with ovarian volume (p=0.000) as well as with waist circumference (p=0.03). However, the Total Testosterone, Fasting Glucose: Insulin ratio, LH: FSH ratio and HDL were insignificantly altered. Conclusion: Both homozygous and heterozygous mutation of CYP1A1 confers an increased susceptibility to develop PCO. The abnormal folliculogenesis and hormone imbalance may be a result of CYP1A1 gene polymorphism due to toxin mediated endocrine disruption which along with other contributory factors may lead to full-fledged polycystic ovary syndrome.
<Keywords: Polycystic ovary syndrome; Polycystic ovaries; CYP1A1 T6235C polymorphism
PCOS: Polycystic Ovary Syndrome; PCO: Polycystic Ovary; OR: Odds Ratio; HDL: High Density Lipids; LDL: Low Density Lipids; TT: Wild Genotype; TC: Heterozygous Genotype; CC: Homozygous Genotype
Polycystic Ovary Syndrome (PCOS) is a heterogenous disorder [1] characterized by oligoanovulation with clinical or biochemical hyperandrogenemia [2]. 5-10% of women in reproductive age group are affected [3]. The estimated prevalence of polycystic ovaries as diagnosed by ultrasonography in normal population is more than 20% [4-6]. PCOS has been said to be a spectrum disease with asymptomatic polycystic ovaries lying at one end and full-fledged syndrome at the other end of the spectrum [7].
PCOS has a complex multifactorial etiology in which a number of predisposing genes interact with environmental factors to produce the disease [8,9]. CYP1A1 gene is located at 15q22-q24 and encodes cytochrome P450 enzymes involved in phase I of detoxification pathway. It is involved in oxidation of estradiol to 2-0H and 4-0H catechol estrogens in ovarian and extraovarian tissues [10,11]. Catechol estrogens are detrimental to granulosa cell replication and follicular growth [12]. Furthermore, many environmental procarcinogens like benzo[a]pyrene are activated to carcinogens by CYP1A1 enzymes [13].These carcinogens can affect folliculogenesis and oogenesis [14- 16]. Endocrine disrupters like organochlorines and dioxins cause induction of CYP1A1 enzymes [17,18] and oxidative stress [19], further aggravating the above changes. All these can lead to abnormal folliculogenesis and formation of cysts in ovaries by causing cell damage and cytotoxicity to the oocyte and supporting granulosa cells Moreover, obesity which is an important component of PCOS has been shown to induce hepatic CYP1A1 expression in animal models [20]. CYP1A1 T6235C polymorphism has been shown to be associated with hypertension and endometrial cancer [21,22], both having obesity as an important risk factor and both are found in women with PCOS in later life .Thus, a possible correlation may exist between PCOS, its late metabolic sequelae and CYP1A1 gene expression.
Three types of polymorphisms are known to affect CYP1A1 enzyme activity of which m1 (T6235C) and m2 (ile462val) are known to render the enzyme hyperinducible with increased activity [23-25]. Some studies have shown an association between these polymorphisms and PCOS [26-28] while some have not [29,30]. Since many of these studies have emphasized for further studies in different population groups, the present study was undertaken to find out the association of CYP1A1 polymorphism in women in North India and their susceptibility to develop PCOS.
This study was designed as a case control study and approved by the Ethical Committee of the institute. One hundred women with PCOS aged 18-30 years and a similar number of age matched healthy controls among North Indian women were enrolled for the study. Informed consent was taken from all the subjects.
Inclusion criteria
Diagnosis of PCOS was made on presence of any 2 of the following 3 features {The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Working Group, 2004 (revised 2003) consensus criteria}
1. Oligomenorrhoea (menstrual cycles ≥ 45 days or <8 cycles per year) and/or Amenorrhoea (more than 3 months),
2. Clinical hyperandrogenism (presence of acne, hirsuitism, Ferriman Gallwey Score ≥ 8 or alopecia) [31,32],
3. Polycystic ovaries on sonography (≥12 follicles in one or both ovaries, 2-9 mm in diameter and/or increased ovarian volume >10 ml).
Exclusion criteria
All patients with diabetes mellitus, hypertension, hyperprolactinemia, thyroid disorder, Cushing’s syndrome, acromegaly, premature ovarian failure, virilising adrenal or ovarian tumors and oral contraceptive pill use within last 6 months were excluded from the study. None of the subjects were alcoholic or smoker. Controls were defined as healthy age matched fertile women with regular cycles, absence of clinically apparent hyperandrogenism, obesity, any chronic illness and who were not taking oral contraceptives pills in last six months.
Biochemical and hormone analysis
The blood samples were drawn on day 2 of normal menstrual cycle or progesterone induced bleeding after an overnight fast. Plasma glucose was measured by glucose oxidase peroxidise method (Selectra XL analyser, Vital Scientifics, Holland). Serum cholesterol, triglycerides, LDL and HDL levels were measured using kits by ERBA Diagnostic, Mannheim, Germany. Plasma Insulin, LH, FSH, Porlactin and total Testosterone were measured by chemiluminiscence method (Immulite 1000 System, Siemens) and TSH by IRMA kit (BARC, Mumbai, India).
Sonography
Pelvic sonography (Nemio30, Toshiba, Japan) was crried out in the department of Radiodiagnosis and Imaging on day 2 of the menstrual cycle in cases and controls both.
Genetic analysis
The genetic analysis was carried out in the department of Molecular and Human Genetics. The blood samples were collected in tubes containing EDTA and stored at 40C. Genomic DNA was extracted from peripheral leukocytes by salting out procedure [33]. T6235C variant of CYP1A1 gene was amplified using forward primer 5’CAGTGAAGAGGTGTAGCCGCT3’ and reverse primer 5’TAGGGAGTCTTGTCTCATGCC3’ by polymerase chain reaction (Bio-Rad laboratories Inc., Berkeley, California). Initial denaturation at 94°C for 5 minutes was followed by 35 cycles at 94°C for 60 seconds, at 63°C for 60 seconds and extension at 72°C for 60 seconds followed by final extension at 72°C for 10 minutes. PCR product was digested with msp1 restriction enzyme (Fermentas Life Sciences, Burlington, Canada) and left overnight at 37°C. Subsequently, the PCR products were separated using 2% agarose gel electrophoresis followed by visualization under UV illuminator after ethidium staining (Gel Documentation System, Alphalmager, USA).
Genotypes were expressed as TT for homozygous wild type (Normal), TC for heterozygous and CC for homozygous mutant genotypes. In normal TT genotype, a single band of 340 bp was produced. The two bands of 200 bp and 140 bp indicate homozygosity for C allele and presence of 3 bands of 340 bp, 200 bp and 140 bp indicate heterozygosity (TC, Figure 1).
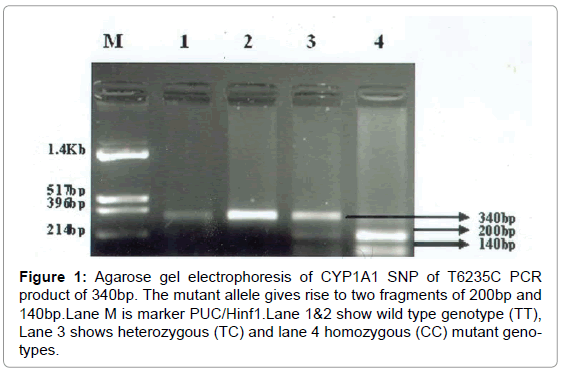
Figure 1: Agarose gel electrophoresis of CYP1A1 SNP of T6235C PCR product of 340bp. The mutant allele gives rise to two fragments of 200bp and 140bp.Lane M is marker PUC/Hinf1.Lane 1&2 show wild type genotype (TT), Lane 3 shows heterozygous (TC) and lane 4 homozygous (CC) mutant genotypes.
Statistical analysis
SPSS 16.0 for Windows (SPSS Inc, Chicago, IL, USA) was used for statistical analysis. All quantitative variables (Continuous, interval– scaled or ratio scaled) were expressed as mean ± standard deviation while for qualitative variables; a frequency along with their respective percentage was given .The distribution for each variable was tested for normality. The comparison of means was done by Student “t” test and Analysis of Variance (ANOVA) as required. For nominal (categorical) variables, Chi-square (χ2) test was used .For calculation of risk, Odds Ratio (OR) and 95% Confidence Interval (CI) were calculated. A p-value less than 5% (p<0.05) was considered statistically significant.
The demographic, anthropometric, biochemical, hormonal, and sonographic parameters of women with PCOS were compared with that of controls as shown in Table 1.
| Parameters | PCOS (n=100) | Control (n=100) | p-value |
|---|---|---|---|
| Age (yrs) | 23.99 ± 4.20 | 24.32 ± 2.43 | 0.50 |
| Age at menarche (yrs) | 12.73 ± 0.89 | 12.55 ± 0.74 | 0.12 |
| BMI (kg/m2) | 27.70 ± 2.42 | 23.35 ± 1.82 | <0.001 |
| Waist circumference (inches) | 35.91 ± 2.58 | 31.20 ± 1.76 | <0.001 |
| Waist : hip ratio | 0.86 ± 0.06 | 0.81 ± 0.03 | <0.001 |
| LH (mIU/ml) | 8.55 ± 5.03 | 2.71 ± 0.78 | <0.001 |
| FSH (mIU/ml) | 4.84 ± 1.55 | 4.59 ± 0.88 | 0.16 |
| LH/FSH ratio | 1.87 ± 1.05 | 0.59 ± 0.15 | <0.001 |
| TSH (IU/ml) | 1.49 ± 0.81 | 1.52 ± 0.78 | 0.84 |
| Prolactin (ng/ml) | 10.39 ± 6.03 | 9.37 ± 3.87 | 0.79 |
| Total testosterone (ng/dl) | 32.39 ± 26.21 | 12.16 ± 6.77 | <0.001 |
| Fasting glucose (mg/dl) | 92.81 ± 3.72 | 79.39 ± 4.25 | <0.001 |
| Fasting insulin (mU/ml) | 19.20 ± 2.45 | 11.72 ± 1.65 | <0.001 |
| Glucose insulin ratio | 4.90 ± 0.65 | 6.88 ± 0.93 | <0.001 |
| Cholesterol (mg/dl) | 204.87 ± 18.55 | 181.55 ± 22.93 | <0.001 |
| Triglyceride (mg/dl) | 83.76 ± 24.53 | 68.97 ± 17.72 | <0.001 |
| LDL (mg/dl) | 71.85 ± 24.42 | 48.62 ± 7.86 | <0.001 |
| HDL (mg/dl) | 48.61 ± 7.86 | 71.85 ± 24.42 | <0.001 |
Table 1: Demographic, anthropometric, biochemical, hormonal and sonographic parameters of the study population: PCOS women and controls (mean ± SD).
Genotype distribution and allele frequency of CYP1A1 T6235C polymorphism were compared between women with PCOS and controls (Table 2a).TC genotype was 1.3327 times more (p=0.32) and CC genotype was 2.6084 times more (p=0.14 ) in women with PCOS.
| Polymorphism | PCOS (n=100) | Control (n=100) | OR | 95% CI | P value | ||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | ||||
| TT | 50 | 50.0 | 59 | 59.0 | 1.0 | - | - |
| TC | 43 | 43.0 | 38 | 38.0 | 1.3327 | 0.7509-2.3652 | 0.32 |
| CC | 7 | 7.0 | 3 | 3.0 | 2.6084 | 0.7173-9.4843 | 0.14 |
| TC+CC | 50 | 50.0 | 41 | 41.0 | 1.434 | 0.8236-2.5002 | 0.20 |
| T | 143 | 71.5 | 156 | 78.0 | 1.4 | 0.8985-2.2125 | 0.14 |
| C | 57 | 28.5 | 44 | 22.0 | |||
Table 2A: Distribution of genotypes and allele frequencies of CYP1A1 T6235C polymorphism in study population: PCOS women and controls.
Among the 100 women with PCOS, 82 had sonographic presence of Polycystic Ovaries (PCO). When genotype distribution and allele frequency were compared in these PCOS women with PCO (n=82) and controls (n=100, Table 2b), the risk ratio of bearing TC genotype was 1.872 (p=0.04) and CC genotype was 4.05 (p=0.08). The combined relative risk of TC and CC was also significantly high (OR=2.032, p=0.02).
| Polymorphism | PCOS with polycystic ovaries (n=82) | Control (n=100) | OR | 95% CI | p value | ||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | ||||
| TT | 34 | 41.4 | 59 | 59.0 | 1.0 | - | - |
| TC | 41 | 50.0 | 38 | 38.0 | 1.872 | 1.02-3.45 | 0.04 |
| CC | 7 | 8.5 | 3 | 3.0 | 4.05 | 0.98-16.70 | 0.08 |
| TC + CC | 48 | 58.0 | 41 | 41.0 | 2.032 | 1.22-3.677 | 0.02 |
| T | 109 | 66.5 | 156 | 78.0 | 1.789 | 1.123-2.851 | 0.01 |
| C | 57 | 28.5 | 44 | 22.0 | |||
Table 2B: Distribution of genotypes and allele frequencies of CYP1A1 T6235C polymorphism in study population: PCOS with polycystic ovaries and controls
The demographic, anthropometric, biochemical, hormonal and Sonographic parameters of PCOS women with PCO were compared in relation to the three genotypes, TT, TC, CC (Table 3). We found non-significant difference among clinical parameters (age, age at menarche, and body mass index except waist circumference). The waist circumference was significantly more (p=0.03) in CC genotype as compared to TT and TC genotypes. The hormonal and biochemical parameters (LH, FSH, LH: FSH ratio, Total Testosterone, LDL, HDL and Fasting glucose: Insulin ratio) also did not reveal any significant alteration. On ultrasonography, the mean ovarian volume was significantly more in both TC and CC genotypes as compared to TT genotype in women with PCOS (p=0.000).
| Parameters | TT (n=34) | TC (n=41) | CC (n=7) | p-value |
|---|---|---|---|---|
| Age (yrs) | 23.76 ± 3.86 | 23.90 ± 4.12 | 24.14 ± 5.64 | 0.97 |
| Age at menarche (years) | 12.52 ± 1.02 | 12.63 ± 0.73 | 13.28 ± 1.11 | 0.132 |
| BMI (kg/m2) | 29.08 ± 1.36 | 27.36 ± 2.47 | 29.08 ± 1.36 | 0.07 |
| Waist circumference (inches) | 36.63 ± 2.37 | 35.38 ± 2.72 | 37.57 ± 1.71 | 0.03 |
| LH (mIU/ml) | 8.20 ± 5.65 | 8.90 ± 4.57 | 9.60 ± 2.11 | 0.73 |
| FSH (mIU/ml) | 4.79 ± 1.28 | 5.14 ± 1.67 | 4.67 ± 1.75 | 0.54 |
| LH:FSH ratio | 1.75 ± 1.09 | 1.85 ± 0.96 | 2.25 ± 0.79 | 0.49 |
| TSH (IU/ml) | 1.64 ± 0.86 | 1.38 ± 0.71 | 1.74 ± 1.30 | 0.33 |
| Prolactin (ng/ml) | 10.59 ± 7.31 | 10.17 ± 4.67 | 10.12 ± 8.62 | 0.95 |
| Total Testosterone (ng/dl) | 33.70 ± 29.31 | 28.50 ± 18.01 | 20.87 ± 9.72 | 0.34 |
| Fasting blood glucose (mg/dl) | 92.26 ± 3.86 | 93.47 ± 4.15 | 91.92 ± 1.90 | 0.33 |
| Fasting insulin (mU/ml) | 19.26 ± 2.27 | 19.06 ± 2.43 | 20.31 ± 3.43 | 0.46 |
| Glucose insulin ratio | 4.83 ± 0.45 | 4.98 ± 0.72 | 4.63 ± 0.76 | 0.32 |
| Cholesterol (mg/dl) | 205.76 ± 15.39 | 204.0 ± 15.73 | 209.0 ± 17.65 | 0.67 |
| Triglyceride (mg/dl) | 84.99 ± 27.27 | 78.56 ± 16.72 | 97.37 ± 38.99 | 0.13 |
| LDL (mg/dl) | 73.78 ± 26.08 | 66.90 ± 10.59 | 88.14 ± 48.44 | 0.06 |
| HDL (mg/dl) | 48.85 ± 8.78 | 48.64 ± 6.27 | 43.12 ± 7.85 | 0.17 |
| Ovarian volume (ml) | 11.11 ± 0.86 | 13.72 ± 1.34 | 15.84 ± 1.79 | 0.000 |
Table 3: Demographic, anthropometric, biochemical, hormonal and sonographic profile of PCOS patients with polycystic ovaries according to the genotypes TT, TC and CC of CYP1A1 gene T6235C polymorphism.
A small sample size could be responsible for some insignificantly altered values of certain metabolic and hormonal parameters such as fasting Glucose:Insulin ratio, cholesterol, triglycerides, LH: FSH ratio, and total testosterone levels.
We found an increased risk of CYP1A1 T6235C polymorphism (both homozygous and heterozygous) in women with PCOS. In PCOS women with sonographic presence of Polycystic Ovaries (PCO), this risk ratio was statistically significant (p<0.05). Moreover we also found the ovarian volume to be significantly more in both homozygous (CC) and heterozygous (TC) mutants as compared to normal genotype (TT) in PCOS women with polycystic ovaries. Interestingly, the waist circumference was also significantly more in CC genotype as compared to TT and TC genotypes. It might be possible that obesity is playing a contributory role in CYP1A1 gene expression as found in animal models [20]. Thus our results suggest that both homozygous and heterozygous mutations of CYP1A1 have a significant association with polycyst formation in the ovaries and confer an increased susceptibility to develop Polycystic Ovary Syndrome. The abnormal folliculogenesis and hormone imbalance may be a result of CYP1A1 gene polymorphism which along with other contributory factors may play an important role in the development of full-fledged polycystic ovary syndrome.
Babu et al. [26] were the first to study a relation between CYP1A1 T6235C polymorphism and polycystic ovaries in South Indian women. They found a significant association of CC genotype (OR=3.764, 95% CI=1.308-10.838, p=0.0139) with PCO while we found an OR of 2.6084 (p=0.14) between CC genotype and PCOS. Whereas they took sonographic presence of polycystic ovaries as essential criteria to diagnose PCOS, we used Rotterdem criteria to select such women for the study. When we considered Sonographic presence of polycystic ovaries as an essential criteria, our results were similar (OR=4.05; 95% CI=0.98-16.70) but not significant (p=0.08). In terms of TC genotype Babu et al. [26] found an OR of 1.3729 (p=0.2824) while our results on the contrary showed a significant association between TC genotype and PCOS with PCO (OR=1.872, 95% CI=1.02-3.45, p=0.04). The differences between these two studies may be due to different environment, ethnicity and diet between south and north Indian population.
Unsal et al. [29] did not find a statistically significant difference between PCOS cases and controls (p>0.05) in Turkish population in terms of CYP1A1 T6235C polymorphism. However, they found that TC genotype was 1.78 times more in women with PCOS (p=0.088) as compared to controls but TT genotype was more in controls. They did not find any CC genotype in the study population. Thus ethnicity seems to play an important role in genotype expression.
Although Esinler et al. [27] and Akgül et al. [29] showed a significant association of CYP1A1 gene polymorphism with PCOS in Turkish population, Wang et al. [30] showed lack of such association in Chinese population. However, these studies cannot be compared with the present study as they studied ile462val polymorphism of CYP1A1 gene. Shen et al. [34-36] also found definite risk of developing PCOS in association with polymorphism of C variant of CYP1A1 rs4646903 (T>C) in Turkish and Indian population on the basis of meta-analysis.
There are some limitations in such population based genetic association studies due to small sample size, difference in criteria of defining PCOS, inclusion of PCOS/PCO, narrowed down effect estimates, multiple testing and variation in selection of controls. A metaanalysis of individual studies is another way to deal with the genetic –association data. However, polymorphism of CYP1A1 gene might be used as a biomarker in future for the diagnosis of this heterogenous and metabolic disorder.
Since none of the earlier studies compared clinical and biochemical parameters of PCOS with CYP1A1 genotypes, the results of our study are novel in that they point towards a possible relation between PCOS, PCO, environment and CYP1A1 gene expression. The importance of further research involving larger groups of women and incorporating the clinical and biochemical parameters of PCOS in the study design cannot be over emphasized.
We are thankful to the Department of Molecular and Human Genetics, Banaras Hindu University for genetic analysis of blood samples.
The authors have no conflict of interest.