Journal of Glycobiology
Open Access
ISSN: 2168-958X
ISSN: 2168-958X
Review Article - (2015) Volume 4, Issue 1
Multiple articles have been published describing the N-linked and O-linked oligosaccharide structures of hCG. All, however, have used purified preparation from pregnancy urine and from choriocarcinoma patient urine. This has told the scientific community that pregnancy and choriocarcinoma hCG-related molecules contain Type 1 and Type 2 O-linked oligosaccharides and biantennary and triantennary N-linked oligosaccharide. Recent years have seen the demonstration of two completely independent hCG molecules, hCG and hyperglycosylated hCG. hCG is a pregnancy hormone made by syncytiotrophoblast cell. Hyperglycosylated hCG is a TGFß receptor binding autocrine produced by cytotrophoblast cells. The two independent share a common amino acid sequence and just vary in carbohydrate structure. Unfortunately, all the carbohydrate structure reports are on a mixture of hCG and hyperglycosylated hCG, as present in pregnancy and choriocarcinoma. This does not all anyone to clearly see the carbohydrate structural differences between the two molecules. Here we carefully examine the carbohydrate structural differences between hCG and hyperglycosylated hCG using the B152 hyperglycosylated hCG-specific immunoassay. It is shown that hCG has only Type 1 O-linked oligosaccharides, while hyperglycosylated hCG only has Type 2 O-linked oligosaccharides. Type of O-linked oligosaccharide structure completely distinguishes hCG and hyperglycosylated hCG.
<Keywords: Oligosaccharides; Syncytiotrophoblast cell; Autocrine; Cytotrophoblast cells
The O-linked and N-linked oligosaccharide structures of human chorionic gonadotropin (hCG) has been studied very thoroughly by multiple groups [1-6]. It has been studied by glycosidase digestion methods [1-3], by gel filtration oligosaccharide separation [4], by Dionex oligosaccharide-specific HPLC [5], and by mass spectrometry methods [6]. All oligosaccharide structures found on hCG and hyperglycosylated hCG by these investigators are shown in Figure 1 (NM, NNF and NNF biantennary N-linked structures, NNM, NNN, NNNF triantennary N-linked structures, Bi, Tetra1, Tri1 and Tri2 Type 1 O-linked oligosaccharides, and Tetra2, Hexa, Penta1 and Penta 2 Type 2 O-linked oligosaccharides).
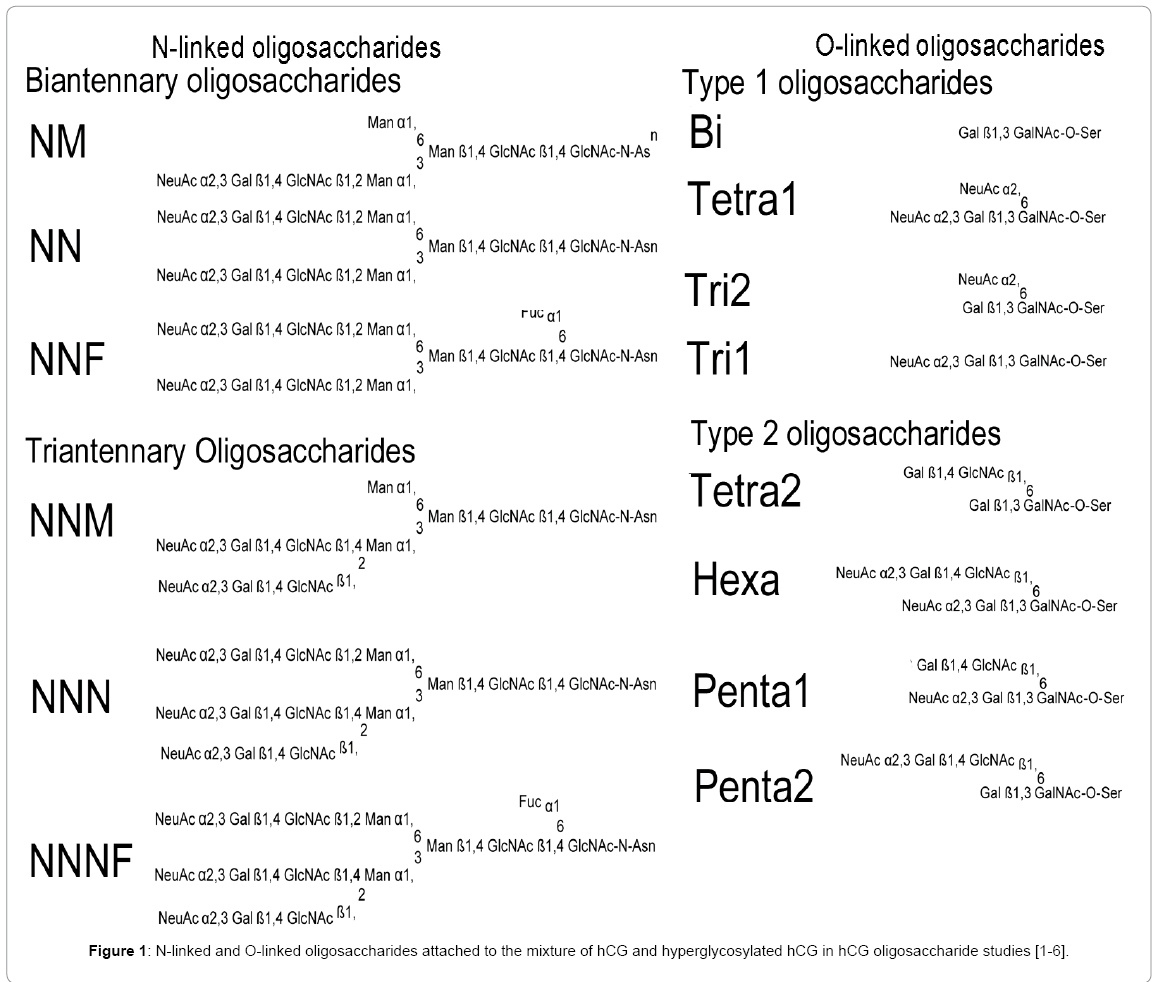
Figure 1: N-linked and O-linked oligosaccharides attached to the mixture of hCG and hyperglycosylated hCG in hCG oligosaccharide studies [1-6].
The problem is that none of these reports show the separate carbohydrate structure of the hormone hCG. All reports show structure of a invariable mixture of the hormone hCG and a completely independent molecule, the autocrine hyperglycosylated hCG. Yes, it is only in recent years, after most of these carbohydrate structure projects were completed [1-5], that the presence of two separate molecules in pregnancy, a hormone and an autocrine, has been demonstrated [7-9].
It is just in the last 8 years that separate research has shown that two molecules both sharing a common a- and ß-subunit amino acid sequence, are produced in pregnancy [7,8]. hCG the hormone promotes hemochorial placentation, promotes maternal ovarian progesterone production, suppresses macrophage destruction of the feto-placenta unit, and suppresses myometrial contractions during pregnancy. Hyperglycosylated hCG, the second molecule is an autocrine acting on TGFß-II receptor [9,10]. This controls invasion of the uterus during implantation of the blastocyst in pregnancy, growth of cytotrophoblast cells and villous trophoblast tissue during pregnancy [11-14]. The problem is that the hormone hCG and the autocrine hyperglycosylated hCG are not readily separable by gel filtration methods, ion exchange chromatography methods, reverse phase methods or other HPLC methods.
The problem is that all hCG carbohydrate structure studies have been completed with first trimester pregnancy urine and choriocarcinoma (cancer of trophoblast cells) patient urines, both are a mixture of hCG and hyperglycosylated hCG. Today scientists simply assume that the hormone hCG has the wide mixture of carbohydrate side chains, including triantennary N-linked and Type 2 O-linked (Figure 1: Tetra2, Hexa, Penta1 and Penta2), and do not consider the possibility of two independent molecules. What has worsened this situation are the claims by Valmu et al. [6] that one sugar attachment site, Ser 121, may be only Type 2 sugars site on all hCG and hyperglycosylated hCG molecules and a second attachment site, Ser 138, may be all Type 1 sugars (Figure 1: Tetra1, Tr1, Tr2, and Bi). Affirming that the hormone hCG contains some large hyperglycosylated sugars. Together this data has wrongly led to the impression that the hormone hCG contains Type 1 and Type 2 O-linked oligosaccharides, and that hyperglycosylated hCG contains the both Type 1 and Type 2 structures also.
Here for the first time we examine all published carbohydrate data and use an immunoassays to specifically measure hyperglycosylated hCG separate to hCG. We examine for the first time the real structures of oligosaccharides attached to the autocrine hyperglycosylated hCG and the hormone hCG.
In order to investigate carbohydrate structure reports [1-6], and the proportion of pregnancy hCG preparations which is in pregnancy and choriocarcinoma urine preparations, pregnancy urine was collected. Volunteers were sought eager to achieve pregnancy. A total of 243 volunteers were accumulated. In these cases, urine was collected daily over as many as 5 menstrual cycles. A total of 175 volunteers eventually achieved pregnancy. Woman received a small financial sum for their cooperation and collection of daily urines. Retrospectively, after all pregnancies had completed, 93 had normal term pregnancies with baby delivery, 38 had spontaneous abortion in pregnancy during the first or second trimester, 4 had ectopic pregnancies, and 40 had early biochemical pregnancies. Daily urines were tested for total hCG and hyperglycosylated hCG and frozen. Those achieving pregnancy collected daily urines up to 10 weeks of gestation. Multiple volunteers terminated the program before 10 weeks of gestation. A total of 2390 pregnancy urines were collected. Collection of urines was overseen by University of New Mexico Human Research Review Committee, license 04-132.
In this volunteer program care was taken to record in study records the first day of menstrual bleeding for each menstrual cycle. Care was taken not to confuse this event with other vaginal bleeding events. In every case, the day of the LH peak was recorded, along with the day of implantation. The day of implantation was recorded as the first day of significant urine total hCG detection (≥ 1 mIU/ml). As shown by Wilcox et al. this marks pregnancy implantation [15,16].
Total hCG was determined in urine using the Siemens Immulite 1000 automated assay in the 2390 pregnancy urines. Values were recorded in mIU/ml. LH was also determined using the Immulite 1000 assay. Hyperglycosylated hCG was determined as described previously [17,18]. Briefly, microtiter plates were coated with B152 antibody, an antibody against C5 hCG preparation [5,19]. Samples were incubated four hours in washed microtiter plates. Enzyme-labeled core antibody to hCG ß-subunit was added and incubation continued a further two hours. Plates were washed and enzyme activity recorded. The hyperglycosylated hCG assay used C5 hyperglycosylated hCG standard [5]. The hyperglycosylated hCG assay results were recorded in ng/ml. The assay had a sensitivity of 0.02 ng/ml.
The specificity of the B152 hyperglycosylated hCG test was examined using urine samples from the USA hCG Reference Service from patients with normal pregnancy, patients with choriocarcinoma and case with quiescent gestational trophoblastic disease. All USA hCG Reference Service samples are submitted along with completed consent to use serum or urine results for research.
Term placenta primary cytotrophoblast cultures were conducted by Harvey Kliman MD, PhD using the published procedures [20]. Term placenta was dissected and separated and placed in cell culture as described previously [20]. Day 1 culture fluids were sent to Cole’s laboratory. JEG-3 choriocarcinoma cytotrophoblast cells were cultured three days in a T75 flask in Dulbecco’s Modified Eagles Medium. Culture fluid was changed daily.
All total hCG (Siemens Immulite 1000), LH and hyperglycosylated hCG data for the 243 volunteers was recorded on separate worksheets of a Microsoft Excel (Redmont WA) spreadsheet. In every case the percentage hyperglycosylated hCG was calculated, hyperglycosylated hCG×100/total hCG. The percentage hyperglycosylated hCG in USA hCG Reference Service urine was also calculated. Total hCG results (mIU/ml) were converted into ng/ml by dividing by 11 [17,18]. Hyperglycosylated hCG results (ng/ml) were divided by total hCG results (ng/ml) to yield the proportion hyperglycosylated hCG.
B152 antibody was raised against preparation C5 hCG, a molecule with 103% Type 2 oligosaccharides, or 4 of 4 O-linked oligosaccharides containing Type 2 structures [5,19]. The specificity of this antibody is for hyperglycosylated hCG [7,8]. As published, this antibody detects an O-linked oligosaccharide on hCG at Ser 132 and segments of ß-subunit and a-subunit peptide [21]. The specificity of the assay using antibody B152 is confirmed here. The assay was tested here with the only pure hCG and hyperglycosylated hCG preparations (Sigma, St Louis, recombinant hCG) and pure hyperglycosylated hCG preparations (C5 hCG and cytotrophoblast cell hCG). As published [7,8,22], the hormone hCG is produced exclusively by syncytiotrophoblast cells and the autocrine hyperglycosylated hCG by cytotrophoblast cells.
Two cultures of pure cytotrophoblast cells were examined, primary term placenta cytotrophoblast cell cultures, and JEG-3 choriocarcinoma cytotrophoblast cell cultures (Table 1). Both of these cultures only produce hyperglycosylated hCG and not hCG [7,8]. In both of these cultures the fluids were 100% detected by the B152 hyperglycosylated hCG assay, consistent with just pure hyperglycosylated hCG (100% hyperglycosylated hCG). It was also demonstrated that the B152 assay also detects C5 hCG, 100% pure hyperglycosylated hCG, with 100% accuracy (Table 1).
| Sample | Description | B152 test, ng/ml | Immulite total hCG test, ng/ml | B152, % total hCG |
Identity |
|---|---|---|---|---|---|
| Pregnancy cyto-trophoblast cells | Pregnancy primary culture, day 1 | 2.3 | 2.3 | 100% | hyperglycosylatedhCG only |
| JEG-3 cyto-trophoblast cells | Choriocarcinoma cells, day 3 culture, | 27.5 | 25.0 | 100% | hyperglycosylatedhCG only |
| Choriocarcinoma C5 hCG | Pure preparation, 100% Type 2 O-linked sugars | 4.00 | 4.33 | 100% | hyperglycosylatedhCG only |
| Recombinant hCG, Sigma | Pure preparation, made in hamster ovary cells | <0.02 | 313 | <0.0064% | hCG only |
| hCG Reference Service Case 81 | Quiescent gestational trophoblastic disease | <0.02 | 18.8 | <0.1% | hCG only |
| hCG Reference Service Case 560 | Quiescent gestational trophoblastic disease | <0.02 | 18.9 | <0.1% | hCG only |
| hCG Reference Service Case 107 | Quiescent gestational trophoblastic disease | <0.02 | 12.7 | <0.1% | hCG only |
| hCG Reference Service Case 390 | Quiescent gestational trophoblastic disease | <0.02 | 10.9 | <0.1% | hCG only |
| hCG Reference Service Case 777 | 5 week 3 day normal pregnancy | 11.9 | 23.7 | 50% | Mix |
| hCG Reference Service Case 831 | 9 week 4 day normal pregnancy | 851 | 10500 | 8.1% | Mix |
| hCG Reference Service Case 750 | 11 week 4 day normal pregnancy | 199 | 4164 | 4.8% | Mix |
| hCG Reference Service Case 198 | Choriocarcinoma, resistant to therapy | 148 | 325 | 46% | Mix |
| hCG Reference Service Case 218 | Choriocarcinoma, pre-therapy | 11034 | 12875 | 86% | Mix |
| hCG Reference Service Case 265 | Choriocarcinoma, resistant to therapy | 3400 | 4090 | 83% | Mix |
Table 1: Specificity of B152 test.
The only known example of the pure hormone hCG, with no hyperglycosylated hCG, is recombinant hCG, made in Chinese hamster ovary cells (sold by Sigma, St Louis). This was detected by the total hCG test and not at all by the B152 assay (<0.0064% cross-reactivity) (Table 1), consistent with it being absolutely pure hCG.
The USA hCG Reference Service sees quiescent gestational trophoblastic disease cases. These are women with a history of gestational trophoblastic disease. In this disease a pin head of trophoblast tissue remains. All cytotrophoblast cells have apoptosed so that only nongrowing syncytiotrophoblast (produce hormone hCG only) remain [23,24]. This is the only know disorder that produced only hCG. Urines from four patients with quiescent gestational trophoblastic disease were investigated (Table 1). As shown, these four cases were detected by the total hCG test and not by the B152 assay (<0.1%), consistent with them containing only the hormone hCG (Table 1)
Finally in this study, three pregnancy urines and three urines from patients with choriocarcinoma were investigated (Table 1). As shown, these all contain a mixture of hCG and hyperglycosylated hCG and yield intermediate results (8.1%-86% hyperglycosylated hCG) with the B152 assay. These findings confirm that the B152 assay is a specific test for only hyperglycosylated hCG, with an unmeasurably small crossreactivity with hCG, <0.0064%.
In the published examples where purified pregnancy urine samples were used for investigating the carbohydrate structure of hCG, none of the articles provide any information about the hCG content or hyperglycosylated hCG content of the samples [1-6]. In some cases the gestational age of the urine collection is given (weeks post date of start of last menstrual bleeding). Here we use the very specific B152 hyperglycosylated hCG assay (<0.0064% hCG cross-reactivity) to examine pregnancy urines at 2½ week of gestation to 10 weeks of gestation, we then use this data to determine the likely hyperglycosylated hCG content of the published examples.
As described under Materials and Methods, daily urines were collected from 243 women eager to achieve pregnancy. Of the 243 women 175 achieved over 5 gestation periods pregnancy. Of these 175, 93 had normal delivery term outcomes. These 93 are monitored for day of first menstrual bleeding and serial urines collected from 2½ weeks of gestation until 10 weeks of gestation. As shown in Table 2, the mean concentration of total hCG and B152 hyperglycosylated hCG was calculated for 2½, 3, 3½, 4, 4½, 5, 5½, 6, 6½ 7, 7½, 8, 8½, 9, 9½ and 10 weeks of gestation and the proportions hyperglycosylated hCG exactly calculated. A total of 2390 pregnancy urines were tested. Many volunteers chose to stop daily urine collection prior to 10 weeks of pregnancy. As shown in Table 2 the hyperglycosylated hCG proportion ranged from 77.6% ± 16.1% at day of implantation down to 7.4 ± 2.18% at 10 weeks of pregnancy. Table 2 shows the most comprehensive report ever completed (2390 urines) with proportion hyperglycosylated hCG in pregnancy urines.
| Weeks +LMP | # Urines | Mean % | Standard Deviation |
|---|---|---|---|
| 2½ weeks (2wk 2d – 2wk 5d) | 15 | 77.6% | 16.1% |
| 3 weeks (2wk 5d - 3wk 2d) | 88 | 69.7% | 26.4% |
| 3½ weeks (3wk 2d – 3wk 5d) | 199 | 62.7% | 29.4% |
| 4 weeks (3wk 5d - 4wk 2d) | 378 | 62.0% | 32.7% |
| 4½ weeks (4wk 2d – 3wk 5d) | 114 | 60.9% | 38.1% |
| 5 weeks (4wk 5d - 5wk 2d) | 439 | 54.7% | 27.2% |
| 5½ weeks (5wk 2d – 3wk 5d) | 327 | 48.6% | 28.0% |
| 6 weeks (5wk 5d - 6wk 2d) | 384 | 40.5% | 26.9% |
| 6½ weeks (6wk 2d – 3wk 5d) | 243 | 35.3% | 27.6% |
| 7 weeks (6wk 5d - 7wk 2d) | 236 | 29.2% | 25.8% |
| 7½ weeks (7wk 2d – 3wk 5d) | 141 | 22.8% | 22.6% |
| 8 weeks (7wk 5d - 8wk 2d) | 122 | 17.5% | 16.9% |
| 8½ weeks (8wk 2d – 3wk 5d) | 53 | 12.7% | 8.8% |
| 9 weeks (8wk 5d - 9wk 2d) | 34 | 9.9% | 6.8% |
| 9½ weeks (9wk 2d – 3wk 5d) | 21 | 8.4% | 3.8% |
| 10 weeks (9wk 5d - 10wk 2d) | 16 | 7.4% | 2.18% |
Table 2: Mean hyperglycosylated hCG proportions, B152 assay, in 93 serial pregnancies (2390 urines total).
Table 3 summarizes all reported pregnancy urine carbohydrate data in which the gestational age of sample is reported. Table 3 lists the percent triantennary N-linked oligosaccharides reported on the hCG preparation, and the percent Type 2 O-linked oligosaccharides (Figure 1: Tetra 2, Hexa, Penta1 and Penta2) as reported. The percent hyperglycosylated hCG is listed from Table 2 for the corresponding week of gestation. As such, each reported percent triantennary N-linked oligosaccharides reported, and the percent Type 2 O-linked oligosaccharides is presented with the corresponding percent hyperglycosylated hCG from B152 immunoassay.
| Carbohydrate structure data | B152 assay data | |||||
|---|---|---|---|---|---|---|
| Authors | Sample | Triantennary N-linked oligos, % oligos, % |
Type 2 O-linked oligos, % |
Ratio | Gestational age sample | HyperglycosylatedhCG (Table 2) fogestational age |
| Bahl 1969 [1] | 12% | - | 8½ weeks | 12.7% | ||
| Cole 1987 [4] | Laferla-1 | - | 9.0% 1 | 9 weeks | 9.9%1 | |
| Cole 1987 [4] | Laferla-2 | - | 7.7% 1 | 10 weeks | 7.4%1 | |
| Cole 1987 [4] | Laferla-3 | - | 7.8% 1 | 10 weeks | 7.4%1 | |
| Elliott et al. 1997 [5] | P3 | 6.5% | 12% 1 | 0.54 | 9 weeks | 9.9% 1 |
| Elliott et al. 1997 [5] | P7 | 16.0% | 19% 1 | 0.89 | 8 weeks | 17.5% 1 |
| Elliott et al. 1997 [5] | P8 | 15.9% | 13% 1 | 1.22 | 8½ weeks | 12.7% 1 |
| Elliott et al. 1997 [5] | P9 | 8.3% | 15% 1 | 0.55 | 8 weeks | 17.5% 1 |
| Valmu et al. 2006 [6] | P 5 wk | 18% | 37% 1 | 0.51 | 5 weeks | 54.7%1 |
| Valmu et al. 2006 [6] | P 7 wk | 9.8% | 26% 1 | 0.38 | 7 weeks | 29.2%1 |
1The percentage Type 2 O-linked oligosaccharides significantly correlates with the percentage hyperglycosylated hCG (O-linked oligosaccharide specific antibody) using the B152 assay, r2=0.95.
Table 3: Published carbohydrate data for pregnancy urine mixtures [1-6]. In some cases carbohydrate structures determined on separate subunits, or at separate sites. In this case all data proportionately included and proportion oligosaccharides are calculated for hCG dimer. Ratio is triantennary N-linked oligosaccharides as a proportion of Type 2 O-linked oligosaccharides. Oligos is oligosaccharides.
As shown, in Table 3 in the article by Cole 1987, 9.0%, 7.7% and 7.8% Type 2 O-linked oligosaccharide is observed. These were 9 weeks, 10 weeks and 10 weeks gestational age, and corresponded to 9.9%, 7.4% and 7.4% hyperglycosylated hCG in the B152 immunoassay. As shown in Table 3, a close significant correlation (r2=0.95) was observed between the percent Type 2 O-linked oligosaccharides, and the percent hyperglycosylated hCG as shown by the B152 immunoassay. It was inferred that this proportion Type 2 O-linked oligosaccharide actually derided from hyperglycosylated hCG. A variable proportion triantennary N-linked oligosaccharides was observed, not correlating with the proportion hyperglycosylated hCG. It was concluded that this sugar’s side chains occurrence was random on hCG and hyperglycosylated hCG and did not correlate with percent hyperglycosylated hCG.
Table 4 shows the proportion hyperglycosylated hCG as determined by B152 immunoreactivity as observed on choriocarcinoma molecules listed. Shown is strictly the data published by Elliot et al. [5] because I was able to obtain the B152 immunoreactivity data or percent hyperglycosylated hCG content in these samples. The data was not available from any other reports [1-4,6]. As shown again the percent hyperglycosylated hCG data using the B152 assay exactly correlated with the published percent Type 2 O-linked oligosaccharides (r2=0.97). It was concluded again that these O-linked oligosaccharides were located on a hyperglycosylated hCG component of samples. Once more, no correlation was observed with triantennary N-linked oligosaccharides indicating once again that this type of sugar may randomly exist on pregnancy and choriocarcinoma preparations.
| Carbohydrate structure data | B152 assay data | |||||
|---|---|---|---|---|---|---|
| Authors | Sample | Triantennary N-linked oligos, % | Type 2 O-linked oligos, % |
Ratio | Hyperglycosylated hCG, hCG conc. | Hyperglycosylated hCG percentage |
| Elliott et al. 1997 [5] | C1 | 45% | 67% 1 | 0.67 | 50269, 70866 ng/ml | 70%1 |
| Elliott et al. 1997 [5] | C2 | 31% | 48% 1 | 0.65 | 791, 2450 ng/ml | 32%1hyperglycosylatedhCG |
| Elliott et al. 1997 [5] | C3 | 27% | 88% 1 | 0.31 | 6083, 7874 ng/ml | 87%1hyperglycosylatedhCG |
| Elliott et al. 1997 [5] | C5 | 25% | 103% 1 | 0.24 | 40730, 37500 ng/ml | 108%1 |
| Elliott et al. 1997[5] | C7 | 30% | 68% 1 | 0.44 | 2500, 3937 ng/ml | 64%1 |
1The percentage Type 2 O-linked oligosaccharides significantly correlates with the percentage hyperglycosylated hCG (O-linked oligosaccharide specific antibody) using the B152 assay, r2=0.97.
Table 4: Published carbohydrate data for choriocarcinoma urine mixtures [1-6]. In some cases carbohydrate structures determined on separate subunits, or at separate sites. In this case all data proportionately included and proportion oligosaccharides are calculated for hCG dimer. Oligos is oligosaccharides.
In conclusion, these studies show a tight correlation between B152 hyperglycosylated hCG immunoreactivity and the concentration of Type 2 O-linked oligosaccharide on both pregnancy and choriocarcinoma samples. It is inferred that Type 2 O-linked oligosaccharides may only exist on hyperglycosylated hCG. The hormone hCG seeming is composed of just Type 1 O-linked oligosaccharides. No correlation was observed between B152 immunoreactivity and structure of N-linked oligosaccharide concentration.
From this inference it was calculated that Cole 1987 pregnancy urine preparations [4], Laferla 1, Laferla 2, and Laferla 3 contained 91%, 92.3% and 92.2% hCG 9.0%, 7.7% and 7.8% hyperglycosylated hCG. That Elliott 1997 pregnancy urines, P3, P7, P8 and P9 [5] contained 88%, 81%, 87% and 85% hCG, and 12%, 19%, 13% and 15% hyperglycosylated hCG. That the two Valmu 2006 pregnancy urines from 5 weeks and 7 weeks pregnancy [6] contained. 63% and 74% hCG, and 37% and 26% hyperglycosylated hCG. Finally, that the Elliott 1997 choriocarcinoma specimens [5], C1, C2, C3, C4 and C7 contained 33%, 52%, 12%, 0%, and 32% hCG, and 67%, 48%, 88%, 103% and 68% hyperglycosylated hCG.
From the summary of these results it is concluded that the average pregnancy urine preparation contains 84% hCG and 16% hyperglycosylated hCG. While the average choriocarcinoma urine preparation contains 25% hCG and 75% hyperglycosylated hCG.
Data presented here indicate that the published results for hCG carbohydrate data are for a mixture of molecule containing the hormone hCG and the autocrine hyperglycosylated hCG [1-6]. Analysis of this data, and examination of results here showing the percent hyperglycosylated hCG in pregnancy and choriocarcinoma urines indicate that the Type 1 O-linked oligosaccharides (Bi, Tetra1, Tri1, Tri2) shown in Figure 1 belong to the hormone hCG, and that the Type 2 O-linked oligosaccharides (Tetra2, Hexa, Penta1 and Penta2) shown in Figure 1 belong to the autocrine hyperglycosylated hCG. The results presented here indicate that separated hyperglycosylated hCG contains 100% Type 2 O-linked oligosaccharides, but that the hormone hCG contained no Type 2 oligosaccharides.
It is inferred from these finding that the average pregnancy urine preparation contains 84% hCG and 16% hyperglycosylated hCG. While the average choriocarcinoma urine preparation contains 25% hCG and 75% hyperglycosylated hCG.
The inferences presented here are very much substantiated by the data of Butler et al. and Iles et al. [25,26]. Using matrix assisted laser desorption ionization mass spectrometry. Butler and Iles have been able to demonstrate the Type 2 O-linked oligosaccharides only on hyperglycosylated hCG molecules, and the small Type 1 O-linked oligosaccharides only on hCG, confirming the evidence presented here [25-27].
Further substantiation comes from the proposed three dimensional structures of hCG and hyperglycosylated hCG based on the thermodynamic three dimensional modelling studies of Butler et al. (manuscript in preparation)(27). As found, the entire difference between these two molecules, an autocrine and a hormone, lies in the O-glycosylated C-terminal peptide. This confirms the findings present here, that hCG has Type1 and hyperglycosylated hCG has Type 2 O-linked oligosaccharides, their principal distinction, on the C-terminal peptide.
This proves that 4 of 4 O-linked oligosaccharides (Ser 121, Ser 127, Ser 132 and Ser 138) are Type 2 oligosaccharides on hyperglycosylated hCG and that none of 4 O-linked oligosaccharide are Type 2 oligosaccharides on hCG. Four of 4 O-linked structures are type 1 oligosaccharides on hCG. Results suggest that Type 1 and Type 2 O-linked oligosaccharides are the principal difference between hCG and hyperglycosylated hCG.
The recent studies of Valmu and colleagues [6], examined the hCG oligosaccharide structures by mass spectrometry. This study very much disagrees with the conclusions presented in this article and infers that the Ser 121 site on both hCG and hyperglycosylated hCG contains just Type 2 O-linked oligosaccharides, and that the Ser 138 site on both hCG and hyperglycosylated hCG contains only Type 1 O-linked oligosaccharides. This infers that the finding reported here are wrong.
Valmu and colleagues [6] conduct a small study with just two first trimester pregnancy urine hCG samples and just one choriocarcinoma patient. They conclude that Ser 121 is only Type 2 oligosaccharide (Figure 1) and that Ser 133 is only Type 1 oligosaccharides from this small study. When considering the abundance of evidence from Elliott et al. [5], Cole LA [4], Amano et al. [2] and Kessler et al. [28], they all show that the conclusion of Valmu et al. cannot be possible. Elliott et al. [5] examined four, not two first trimester pregnancy individual samples, and 5 choriocarcinoma, not one choriocarcinoma samples sample. They show that the first trimester of pregnancy contains 12%, 19%, 15.9%, and 8.3% Type 2 O-linked oligosaccharides. This is inconsistent with the concept that Ser 121 contain only O-linked oligosaccharides or 25%, a much larger concentration of O-linked oligosaccharides (Table 3). The research of Elliott et al. examines O-linked oligosaccharides on choriocarcinoma. It shows that choriocarcinoma samples contain 67%, 48%, 88%, 103% and 58% Type 2 structures. This indicates that 2.7, 1.9, 3.5, 4.0 and 2.3 of 4.0 sites contain Type 2 structures (Table 4). This is very much contrary to the Valmu et al. finding that one site always contains just these oligosaccharides.
Similarly, the findings of Cole [4] examine 3 first trimester pregnancy samples. These contain 9.0%, 7.7% and 7.8% Type 2 oligosaccharides. This is very inconsistent with the concept that Ser 121 always has 1.0 of 4.0 or 25% Type 2 oligosaccharides (Table 3). Similar contradictory findings are shown by Amano et al. [2] and Kessler et al. [28]. Kessler et al. even claim [28], that all four sites contain similar oligosaccharides. The findings of Valmu et al. [6] are challenged here, challenged by four publication and this article and a very much larger abundance of samples. It is concluded again that Type 2 oligosaccharides are seemingly unique to hyperglycosylated hCG. It appears that cytotrophoblast, the cells which make hyperglycosylated hCG contain the N-acetylyglucosaminyl transferase VI critical to making Type 2 oligosaccharides, but that this N-acetylglucosaminyl transferase VI is seemingly missing in syncytiotrophoblast cells, the cells which make hCG.