Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
Research Article - (2013) Volume 2, Issue 3
Aim: This study investigated the effect of L-thyroxine on clinical manifestations and EPO responses, and the approach to L-thyroxine dosage adjustment for HD patients with Incidental hypothyroidism.
Methods: Ten cases of Incidental hypothyroidism were diagnosed in 695 HD patients. In this study, L-thyroxine therapy was given only to hypothyroid HD patients with clinical symptoms, hematocrit <35%, and whose hypothyroidism was caused by medications which could not be discontinued. The initial dosage of L-thyroxine was 0.025 mg daily, and continuous adjustment was made according to clinical manifestations, patient’s tolerance of L-thyroxine, and hematocrit level rather than TSH, T4 or FT4 value.
Results: Of the 10 cases of Incidental hypothyroidism, 2 were autoimmune-induced, 5 were non-autoimmuneinduced, 2 were amiodarone-induced, and 1 was interferon-induced. Among them, 7 were treated with L-thyroxine and 3 were not. After L-thyroxine therapy, all 7 patients got symptoms improvement with 3 having EPO dosage reduced by more than 20%, 3 having hematocrit increased by more than 20%, and no patient requiring blood transfusion to keep hematocrit >30%. The clinical manifestations were found to improve after discontinuation of medications in two of those three patients with medication-induced hypothyroidism. L-thyroxine therapy may not be required for HD patients with hypothyroidism and hematocrit >35%.
Conclusions: Adjustment of L-thyroxine dosage according to clinical manifestations, rather than TSH, T4 or FT4 value, is a practical and effective treatment approach for HD patients with hypothyroidism. This approach of L-thyroxine therapy could reduce EPO dosage, and improve both anemia and clinical symptoms.
<Keywords: Hypothyroidism; L-thyroxine; Hypoxia-induced Erythropoietin (EPO); Hemodialysis (HD); Thyroidectomy; Parathyroidectomy
Thyroid hormone plays a crucial role in the metabolic activities of adults. Therefore, the compensation of decreased T3 production from T4 in hemodialysis (HD) patients may provide metabolic adaptation for energy conservation, as in patients with nonrenal nonthyroidal illnesses and caloric deprivation [1,2].
Thyroid hormone has also been demonstrated to enhance hypoxiainduced erythropoietin (EPO) production in addition to metabolic activities [3]. A euthyroid state is essential for the action of EPO on the bone marrow. Hypothyroidism could contribute to EPO resistance in patients with chronic renal failure [4-7].
The use of EPO in most HD patients to correct renal anemia [8,9] may also mask the similar symptoms and signs between hypothyroidism and uremia (i.e., anemia, lethargy, constipation, cold intolerance, and poor appetite) [10,11], thus making diagnosis of hypothyroidism difficult. Furthermore, the association of EPO with L-thyroxine therapy remains largely unknown [11-14]. Attempts to normalize circulating thyroid hormone for the EPO response may be harmful to HD patients with hypothyroidism, who may suffer excessive waste of protein nitrogen [1,2]. With hypothyroidism left untreated, the dosage of EPO can be increased to overcome the EPO resistance in HD patients. Whether the identified HD patients with hypothyroidism should be treated with L-thyroxine for the action of EPO on the bone marrow or left untreated for energy conservation is worth further investigation. The aim of this study is to investigate the effect of L-thyroxine on clinical manifestations and EPO responses, and the approach to L-thyroxine dosage adjustment for HD patients with Incidental hypothyroidism.
Thyroid function test, definitions of hypothyroidism and Incidental hypothyroidism
Venous blood samples were drawn immediately before HD and sent to the central laboratory at TVGH for measurement of serum thyroid stimulating hormone (TSH), antithyroid peroxidase antibodies (anti-TPO) and auto-antibodies against thyroglobulin (anti-TG) using chemiluminescent immunometric assay (DPC Immulite 2000; Seracon Diagnostic Co., Brownsville, TX, USA). Free thyroxine (FT4), total thyroxine (T4) and total triiodothyronine (T3) were measured by chemiluminescent, a competitive analogue immunoassay (DPC Immulite 2000).
Hypothyroidism not related to autoimmune mechanism was defined as TSH level >4 μIU/ml (normal range 0.4-4 μIU/ml) and FT4<0.80 ng/dL (normal range 0.80-1.90 ng/dL). Hypothyroidism of autoimmune etiology was defined as TSH level >4 μIU/ml, FT4 <0.80 ng/dL, and anti-TPO >35 IU/ml (normal range <35 IU/ml) or anti-TG >40 IU/ml (normal range<40 IU/ml) [15]. The patients with normal TSH normal FT4 and low T3, low TSH and normal FT4, low TSH and low FT4, normal TSH and low T4, and normal TSH and low T3 were defined as euthyroid sick syndrome and not recruited in this study.
In this study, Incidental hypothyroidism was defined as a fresh case of hypothyroidism not related to thyroidectomy or I131 therapy of hyperthyroidism discovered during thyroid function screening tests.
Participants
Ten HD patients (6 female, 4 male) that fulfilled the definition of Incidental hypothyroidism during thyroid function screening tests of 695 regular HD patients at 4 in-hospital dialysis units and 2 HD centers in Taiwan in January, 2009 agreed to participate in this study. The underlying etiologies of HD among these patients included diabetic nephropathy, chronic glomerulonephritis, polycystic kidney disease and end-stage renal disease (ESRD) (Table 1). None of the patients had malignancy, liver cirrhosis, thalassemia, iron deficiency, gastrointestinal bleeding, and major operation within 6 months prior to the thyroid function screening test. The study protocol was approved by the institutional review board of Taipei Veterans General Hospital (TVGH) (VGHIRB No.: 97-07-30A). All patients provided written informed consent.
| Group | NMT | NMNT | MT | MNT | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Case no. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Sex | F | F | M | M | F | F | M | F | F | M |
| Age (years) | 70 | 53 | 81 | 60 | 71 | 61 | 60 | 72 | 48 | 56 |
| Etiology of hemodialysis | DMN | CGN | CGN | PCKD | CGN | ESRD | ESRD | DMN | DMN | DMN |
| Diagnosis time of hypothyroidism (months after HD) | 10 | 11 | 11 | 178 | 144 | 186 | 234 | 29 | 138 | 78 |
| Parathyroidectomy (yes/no) | no | no | no | no | no | yes | no | no | no | no |
| CAD (yes/no) | no | no | no | yes | yes | no | yes | no | yes | no |
| CVA (yes/no) | no | no | no | yes | no | no | no | no | no | no |
| Thyroid function test before thyroxine treatment | ||||||||||
| TSH (0.4–4µIU/ml) | 145 | 9.3 | 7.7 | 6.9 | 75.1 | 44.2 | 29.2 | 7.3 | 7.2 | 12.3 |
| Free T4 (0.8 - 1.9 ng/dL) | 0.28 | 0.78 | 0.77 | 0.73 | 0.29 | 0.63 | 0.67 | 0.7 | 0.77 | 0.71 |
| T4 (4.5 - 12.5 ug/dL) | 4.8 | 4.2 | 2.9 | 4.2 | 1 | 3.1 | 3.4 | 4.3 | 3.5 | 3.7 |
| T3 (72 - 170 ng/dL) | 39 | 125 | 51.7 | 54.5 | 42.4 | 52.6 | 63.7 | 39 | 48.9 | 57.8 |
| anti-TPO (<35 IU/ml) | <10 | 141 | <10 | <10 | 11.4 | <10 | <10 | <10 | <10 | <10 |
| anti-TG(< 40 IU/ml) | 3001 | 1205 | <20 | <20 | <20 | <20 | <20 | <20 | <20 | <20 |
| Etiology of hypothyroidism | immune | immune | non-immune | non-immune | non-immune | non-immune | non-immune | amiodarone | amiodarone | interferon |
Group NMT, the immune induced hypothyroid patients who received L-thyroxine therapy; Group NMNT, the non-immune induced hypothyroid patients who received L-thyroxine therapy; Group MT, the patient with amiodarone induced hypothyroidism who could not discontinue the medication and received L-thyroxine therapy; Group MNT, the patients with amiodarone or interferon induced hypothyroidism who could discontinue the medications and not received L-thyroxine therapy. F, female; M, male; DMN, diabetic nephropathy; CGN, chronic glomerular nephritis; PCKD, polycystic kidney disease; ESRD, end stage renal disease; CAD, coronary artery disease; CVA, cerebrovascular accident; TSH, thyroid stimulating hormone; anti-TPO, antithyroid peroxidase antibodies; anti-TG, auto-antibodies against thyroglobulin; FT4, free thyroxine; T4, total thyroxine; T3, total triiodothyronine.
Table 1: The basic characteristics of hemodialysis patients with incidental hypothyroidism.
According to the etiology of hypothyroidism and the administration of L-thyroxine therapy, the patients were classified into four types. Patients with non-medication-induced (immune-induced and non-immune-induced) hypothyroidism treated with L-thyroxine were classified as NMT while those with non-medication-induced hypothyroidism not treated with L-thyroxine were grouped under NMNT. Patients with medication-induced (i.e., amiodarone-induced or interferon-induced) hypothyroidism who could not discontinue medications and were treated with L-thyroxine were classified as MT while those with medication-induced hypothyroidism who could discontinue medications and were not treated with L-thyroxine were grouped under MNT. Finally, of the 10 cases of Incidental hypothyroidism, 7 received L-thyroxine therapy and 3 did not. Figure 1 summarizes the study design and classification of patients.
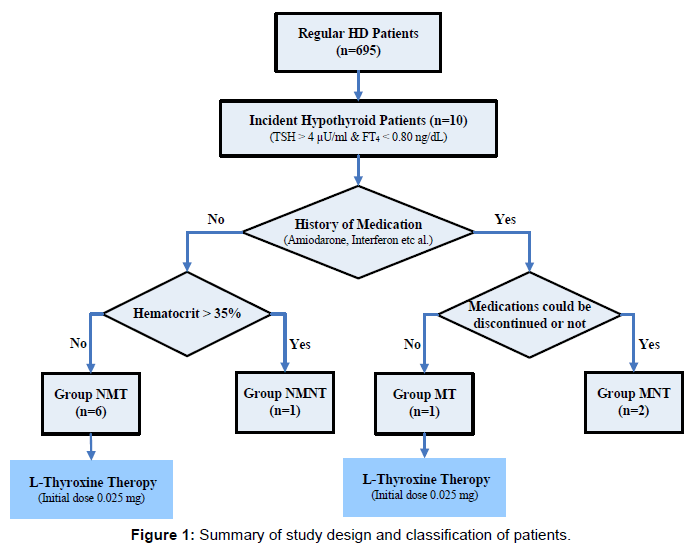
Figure 1: Summary of study design and classification of patients.
Personal and laboratory data
Personal data including age, sex, body weight, height, HD date, etiology of HD, history of parathyroidectomy, cerebral vascular accident (CVA) and coronary artery disease (CAD) were collected. Symptoms such as nausea, poor appetite, depression, constipation, decreased daily activity, and leg edema were recorded according to patient and family description.
In Taiwan, each HD patient is required to have his/her biochemistry profile checked monthly. Hence, biochemistry data including serum level of pre-dialysis BUN, creatinine, sodium, potassium, albumin, cholesterol, triglyceride, uric acid, calcium, phosphate, glucose, iPTH, hemoglobin, as well as efficacy of dialysis (demonstrated by Kt/V) over a 6-month period were obtained at the time of thyroid function tests. The mean monthly values of the above biochemistry data at the beginning and the end of first-year L-thyroxine therapy were used for evaluating the effect of L-thyroxine treatment.
L-thyroxine approach in hypothyroidism patients
Attempts to normalize circulating thyroid hormone for the EPO response may be harmful to HD patients with hypothyroidism, who may suffer excessive waste of protein nitrogen [1,2]. With hypothyroidism left untreated, the dosage of EPO can be increased to overcome the EPO resistance in HD patients. Whether the identified HD patients with hypothyroidism should be treated with L-thyroxine for the action of EPO on the bone marrow or left untreated for energy conservation is in a dilemma. On the other hand, the increased risk of fracture in patients taking long term thyroxine was reported in the previous literatures [16,17]. Therefore, L-thyroxine was given to the non-medication induced hypothyroid HD patients with higher dose of EPO and clinical symptoms not improved by dialysis in this study. The patients with subclinical hypothyroidism were not treated with L-thyroxine in this study. The initial dosage of L-thyroxine therapy was 0.025 mg daily, while the maintenance dosage was continuously adjusted in this study. Previous research has shown that increasing the L-thyroxine dosage until serum TSH values fall within the normal range may induce mild hyperthyroidism and precipitate cardiac events in some ESRD patients, particularly those with diabetes mellitus, the elderly, and those with subclinical or overt ischemic heart disease [11]. T4 and most FT4 estimates should not be taken as the only references when adjusting the L-thyroxine dosage since these values are frequently reduced in euthyroid ESRD patients [12]. Instead of referring to TSH, T4 or FT4 values as in previous research [11,12], adjustment in dosage was made according to clinical manifestations, patient’s tolerance of L-thyroxine, and hematocrit level in order to avoid hyperthyroidism and achieve better EPO response with energy conservation. Therefore, only hypothyroid HD patients with irreversible etiology, clinical symptoms or hematocrit (Hct) level <35% (the upper target of EPO therapy at most HD centers in Taiwan is 35%) were treated with L-thyroxine in this study. Whether there was improvement in symptoms or not was recorded according to patient and family description 6 months after L-thyroxine therapy.
Basic characteristics of HD patients with incidental hypothyroidism
The time for diagnosis of hypothyroidism ranged from 10 to 234 months (mean, 101.9 months) after HD in these 10 patients. Of the 10 cases of Incidental hypothyroidism, 2 were autoimmune-induced (anti-TPO>35 IU/ml or anti-TG>40 IU/ml), 5 were non-autoimmuneinduced, 2 were amiodarone-induced, and 1 was interferon-induced (Table 1). The mean age of NMT (66 years), NMNT (60 years) and MT (72 years) patients were higher than that of MNT patients (52 years).
Clinical manifestations of patients treated with L-thyroxine
Of the 7 patients treated with L-thyroxine, 3 patients (2 NMT, 1 MT) had mean monthly EPO dosage reduced by more than 20%. Three patients (2 NMT, 1 MT) had hematocrit level increased by more than 20%, and all 7 patients had hematocrit level >30% after L-thyroxine therapy (Table 2). Three patients (2 NMT, 1 MT) no longer required blood transfusion after L-thyroxine therapy to maintain hematocrit level >30%. There was an increase in overall serum albumin level of 0.1 to 0.4 g/L in 5 NMT patients, but no change in serum albumin level was observed in the other 2 (1 NMT and 1 MT) patients after L-thyroxine therapy (Table 2).
| Group | NMT | NMNT | MNT | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Case no. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Thyroxin treatment | yes | yes | yes | yes | yes | yes | no | yes | no | no |
| starting dose (mg) | 0.025 | 0.025 | 0.025 | 0.025 | 0.025 | 0.025 | 0 | 0.025 | 0 | 0 |
| maintenance dose (mg) | 0.05 | 0.05 | 0.05 | 0.1 | 0.1 | 0.075 | 0 | 0.05 | 0 | 0 |
| Thyroid function test (before / after thyroxine treatment) | ||||||||||
| TSH (0.4–4µIU/ml) | 145/27.2 | 9.3/17.1 | 7.7/22.4 | 6.9/0.7 | 75.1/3.6 | 44.2/6.1 | 29.2/18.1 | 7.3/16.5 | 7.2/6.3 | 12.3/3.9 |
| Free T4 (0.8 - 1.9 ng/dL) | 0.28/0.98 | 0.78/0.73 | 0.77/0.75 | 0.73/0.98 | 0.29/0.68 | 0.63/1.29 | 0.67/0.56 | 0.70/0.87 | 0.77/0.88 | 0.71/0.83 |
| T4 (4.5 - 12.5 ug/dL) | 4.8/2.6 | 4.2/4.2 | 2.9/3.0 | 4.2/5.6 | 1.0/2.4 | 3.1/4.9 | 3.4/3.4 | 4.3/5.0 | 3.5/5.0 | 3.7/4.3 |
| T3 (72 - 170 ng/dL) | 39.0/39.0 | 125/80.7 | 51.7/58.0 | 54.5/47.9 | 42.4/39.9 | 52.6/41.2 | 63.7/73.0 | 39.0/52.9 | 48.9/39.9 | 57.8/53.6 |
| Thyroid status after treatment | sub. hypo | hypo | hypo | euthy | euthy | sub. hypo | hypo | sub. hypo | sub. hypo | euthy |
| Clinical manifestation (before / after thyroxine treatment) | ||||||||||
| nausea | yes/no | no/no | no/no | yes/no | yes/no | yes/no | no/no | yes/no | no/no | yes/no |
| poor appetite | yes/no | no/no | no/no | yes/no | yes/no | yes/no | no/no | yes/no | no/no | yes/no |
| depression | yes/no | no/no | no/no | no/no | no/no | no/no | no/no | yes/no | no/no | yes/no |
| general weakness | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no | no/no | yes/no | no/no | yes/no |
| constipation | yes/no | no/no | no/no | yes/no | no/no | no/no | no/no | no/no | no/no | no/no |
| decreased daily activity | yes/no | no/no | no/no | no/no | yes/no | yes/no | no/no | no/no | no/no | no/no |
| leg edema | yes/no | no/no | no/no | no/no | no/no | no/no | no/no | no/no | no/no | no/no |
| blood transfusion | yes/no | no/no | no/no | no/no | no/no | yes/no | no/no | yes/no | no/no | no/no |
| Laboratory data (before / after thyroxine treatment) | ||||||||||
| mean monthly EPO (1000IU) | 28/10.4 | 11.5/11.5 | 26/26 | 0.8/1.0 | 43.3/43.8 | 25.7/20 | 0/0 | 31.4/21.3 | 18.7/16.5 | 28.2/22.7 |
| EPO dosage reduced >20% | yes | no | no | no | no | yes | no | yes | no | no |
| Hct (%) | 27.6/35.1 | 29.2/35.8 | 28.5/33.2 | 31/35 | 31.1/34.3 | 28.9/33.3 | 35.8/41 | 25.4/31.7 | 28.7/30.8 | 30.6/30.3 |
| Hct increase >20% | yes | yes | no | no | no | no | no | yes | no | no |
| Albumin (3.7-5.3 g/dL) | 3.8/4.0 | 3.6/4.0 | 3.5/3.7 | 4/4.3 | 3.9/4 | 4.1/4.1 | 4/4.2 | 3.7/3.7 | 3.5/3.5 | 3.6/4.1 |
| Cholesterol (125-240 mg/dL) | 133/155 | 161/179 | 206/159 | 116/111 | 198/221 | 179/175 | 220/195 | 191/131 | 199/219 | 186/210 |
| Triglyceride (20-200 mg/dL) | 155/109 | 198/212 | 127/216 | 30/71 | 185/359 | 99/137 | 82/85 | 421/189 | 130/125 | 108/139 |
| iPTH (pg/ml) | 164/143 | 127/96 | 21/59 | 308/582 | 266/37 | 176/278 | 711/443 | 141/109 | 134/246 | 47/62 |
| KtV(D) | 1.4/1.6 | 1.6/1.6 | 1.6/1.72 | 1.8/1.7 | 2.1/2.1 | 1.5/1.6 | 2.2/2.1 | 1.9/1.7 | 1.3/1.4 | 1.8/1.95 |
HD, hemodialysis; NMT, non-medication-induced hypothyroid patients treated with L-thyroxine; NMNT, non-medication-induced hypothyroid patients not treated with L-thyroxine; MT, medication-induced hypothyroid patients who could not discontinue the medication and were treated with L-thyroxine; MNT, medication-induced hypothyroid patients who could discontinue the medication and were not treated with L-thyroxine; TSH, thyroid stimulating hormone; FT4, free thyroxine; T4, total thyroxine; T3, total triiodothyronine; sub. hypo, subclinical hypothyroidism; .hypo, hypothyroidism; euthy, euthyroidism.
Table 2: Thyroid function, clinical manifestation and laboratory data before and after L-thyroxine therapy in HD patients with incidental hypothyroidism.
There was no case of hyperthyroidism found after L-thyroxine therapy in this study. Two NMT patients became euthyroid, 2 NMT and 1 MT patients became subclinical hypothyroid and 2 NMT patients remained hypothyroid. The dosage of L-thyroxine was maintained at 0.05 mg in 4 patients (3 NMT, 1 MT), 0.075 mg in 1 NMT patient, and 0.1 mg in 2 NMT patients (Table 2). All patients treated with L-thyroxine had clinical symptoms subsided (Table 2).
Clinical manifestations of patients not treated with L-thyroxine
In those 3 patients not treated with L-thyroxine, 2 of them had no clinical symptoms. The clinical symptoms of the interferon-induced hypothyroid patient also subsided after interferon discontinuation. During this one-year study, the NMNT patient maintained hematocrit level >35% without EPO supplement while the 2 MNT patients had hematocrit level >30% after amiodarone and interferon discontinuation without increase in EPO dosage (Table 2). The hypothyroid status of the NMNT patient remained hypothyroidism, while that of the MNT patients shifted to subclinical hypothyroidism and euthyroidism after discontinuation of amiodarone and interferon, respectively (Table 2).
Although the exact onset and duration of hypothyroidism of our participants could not be known from thyroid function screening test, the board range of diagnosis time of hypothyroidism from 10 to 234 months after HD in this study further supported previous findings that clinical unawareness of hypothyroidism in HD patients was attributed to the insidious onset of hypothyroidism and the similarity between its nonspecific symptoms and signs of uremia including anemia, lethargy, constipation, cold intolerance, and poor appetite [10,11].
The lower presence of antithyroid antibodies (positive anti-TPO and/or anti-TG antibodies) among our participants (20%) (Table 1) than in the general population (54% to 67%) [18-22], was in agreement with previous reports on HD patients with hypothyroidism [23,24]. The inconsistent etiology of hypothyroidism in the general population and HD patients was not clearly understood in the past. Previous studies have shown that maintenance dialysis cannot improve impaired immunity in HD patients [25,26] and both titer and response rate remained low despite vaccinations for viral hepatitis, tetanus and diphtheria [27,28]. Hence, we postulated that the inconsistent prevalence of antithyroid antibodies in hypothyroidism between the general population and HD patients may partly be due to the impairment of immune function in dialysis patients.
No case of hyperthyroidism was found after L-thyroxin therapy with dosage adjusted according to clinical manifestations, patient’s tolerance of L-thyroxine, and hematocrit level >30%. In contrast, there were cases of hyperthyroidism found after L-thyroxine therapy with dosage adjusted in accordance with keeping serum TSH values within the normal range [11]. Such difference can be attributed to our approach to dosage adjustment. In addition, of the 7 hypothyroid patients in this study, only 2 became euthyroid while most hypothyroid patients became euthyroid (normal thyroid function) after L-thyroxine therapy with dosage adjusted according to the TSH and T4 value. Nevertheless, the 2 patients who became subclinical hypothyroid and the other 2 who remained hypothyroid all had improved clinical manifestations and anemia as well as reduced EPO dosage. The results of the NMNT patient in this study indicate that L-thyroxine therapy may not be needed for hypothyroid HD patients with hematocrit level >35%. Since the thyroid controls a tremendous number of physiological functions and anemia is a multifactorial syndrome, in particular in this population. Thus this study may not be able to answer all the questions regarding the complex interactions and the hypothyroid patients with high hematocrit level but no EPO and L-thyroxine therapy.
This study showed that there was a portion (3 of 10) of HD patients with hypothyroidism caused by medications such as interferon for viral hepatitis and amiodarone for arrhythmia. Therefore, medicationinduced hypothyroidism should be kept in mind for every HD patient with hypothyroidism. Such medications should be discontinued if possible. In cases where discontinuation of medications is impossible due to the underlying diseases, L-thyroxine therapy can still improve anemia and clinical symptoms as seen in our MT patients.
In conclusion, physicians are often unaware of hypothyroidism being a possible cause for poor response of EPO in HD patients. Instead of adjusting the dosage of L-thyroxine therapy with reference to TSH, T4 or FT4 values as in previous research, dosage adjustments made according to clinical manifestations and treatment target of hematocrit level >30% could reduce EPO dosage, improve anemia under lower maintenance dose of L-thyroxine, and avoid hyperthyroidism.
Study limitations
Several methodological issues should be taken into consideration when interpreting our results. First, there are only 10 HD patients with Incidental hypothyroidism diagnosed after thyroid function screening test in 695 HD patients. While our large sample of HD patients could avoid biases, the number of Incidental hypothyroidism cases was small, which may be due to its relatively low incidence. Second, the exact onset and duration of thyroid diseases could not be known from this crosssectional study. Third, we could not differentiate whether or not the clinical symptoms exhibited by the interferon-induced hypothyroid patient were caused by hypothyroidism or side effects of interferon or both. Despite these limitations, L-thyroxine therapy with dosage adjusted by clinical manifestations could avoid L-thyroxine-induced hyperthyroidism, relieve the clinical symptoms of hypothyroidism, reduce the EPO dosage and improve anemia in HD patients with Incidental hypothyroidism.
This study was supported by a grant (V99C1-150) from the Taipei Veterans General Hospital, Republic of China. We thank Ms. Jung Ai Lu, Shih Min Chiu and Ya Hui Sun for their technical support.