Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2014) Volume 2, Issue 5
Purpose: To evaluate the effects of male aging on semen quality and DNA fragmentation in male infertility patients attending Andrology Laboratory at fertility center.
Methods: Semen samples of 217 infertile patients were analyzed using Computer-Assisted Semen Analysis (CASA). Sperm DNA fragmentation was measured by the sperm chromatin dispersion test.
Results: Subject’s ages ranged from 21 to 68 years. The mean age was 38.45 years. The patients were distributed into four groups: <30 years, 30-39 years, 40-49 years and ≥ 50 years. Parameters of volume, pH and concentration were similar in four evaluated groups (P: NS). An age-dependent increase in sperm DNA fragmentation was observed in four evaluated groups. The patients ≥ 40 years old had spermatozoa with fragmented DNA significantly higher compared to those patients from <30 years old and 30-39 years old (P<0.05). Percentages of morphologically normal spermatozoa in patients of ≥ 50 years old were significantly lower compared to those men from group 30-39 years old (P<0.05). Men older than 40 years old had percentages of sperm vitality significantly lower compared to men of 39 years old or less (P<0.05).
Conclusions: Sperm DNA fragmentation, progressive motility, and spermatozoa morphology are associated to advanced paternal age. However, volume, pH, and sperm concentration are not affected by male age.
Keywords: Sperm DNA fragmentation, SCD test, Male aging, Infertility, Semen parameters
The rises in life expectancy, women’s entry into the labor market and the popular use of contraception have contributed to the social phenomena of delaying family planning and parenthood to the mid or late thirties. This has also had a significant impact on males. In Germany, the median age of married fathers has increased from 31.3 years in 1991 to 33.1 years in 1999 [1]. The same trend has also been observed in England. In 1993, fathers aged 35-54 years accounted for 25% of live births. Ten years later, these percentages grew to 40% [2]. Among couples seeking pregnancy through Assisted Reproduction Technologies (ART), fathers are significantly older compared with those not needing ART (36.6 vs. 33.5 years) [3].
In contrast to oogenesis, in which the depletion of ovarian follicles marks the cessation of their reproductive life, spermatogenesis continues throughout life [4]. Nevertheless, male aging does exert a certain detrimental effect on reproductive organs and tissues. For instance, there is a decrease of testicular volume, alterations in testicular histomorphology, and a decrease in the inhibin B/FSH ratio consistent with a reduced Sertoli cell mass [5]. Other observable patterns include a decline in semen volume, motility and daily sperm production per testis [6]. No consistent data confirm that sperm concentration also decline with advancing age [7,8]. On the other hand, several studies have no correlation between advanced paternal age and rates of fertilization, implantation, pregnancy, miscarriage and live birth in IVF [9-13]. However, male aging was associated with a significant decrease in blastocyst embryo formation, probably reflecting male genomic activation within embryo. This effect don’t was observed in embryo quality at the cleavage stage [14,15].
Semen quality is frequently used as an indirect measure of male infertility. Ejaculate volume, sperm concentration, motility and morphology determined according to World Health Organisation (WHO) are the most important parameters evaluated in infertility centers as a part of routine semen analysis. However, theses traditional criteria provide little indication of possible nuclear DNA damage.
Recently, the integrity of sperm DNA is being recognized as a new parameter of semen quality and a marker of male infertility [16,17]. Nevertheless, DNA integrity assessment is not being carried out as a routine part of semen analysis in the clinical laboratory [18]. Sperm DNA fragmentation can be caused by apoptosis in the seminiferous tubule epithelium, defects in chromatin remodeling during the process of spermiogenesis, oxygen radical-induced DNA damage during sperm migration from the seminiferous tubules to the epididymis, the activation of sperm caspases and endonucleases, damage induced by chemotherapy and radiotherapy, and the effect of environmental toxicants [19]. In humans, high levels of sperm nuclear DNA damage have been related to low fertility potential, failure to obtain blastocysts, blockage in embryo development after embryo implantation, increased risk of recurrent miscarriages, reduced chances of successful implantation, and negative effect on the health of offspring [14,20-22].
In this study, we evaluated the effects of male ageing on semen quality and sperm DNA damage and elucidating possible correlations between parameters.
Patients
A total of 217 patients for infertility evaluation at Andrology Laboratory, FERTILAB Laboratory of Assisted Reproduction Lima, Peru were included in this study. All the patients had non antibiotic treatment, history of chemotherapy, radiotherapy, or chronic illness. This protocol was approved by the Institutional Review Board (IRB) and the corresponding Ethics Committee.
Semen samples
The semen samples were collected by masturbation in aseptic conditions in to sterile cups after 2-7 days of sexual abstinence. Semen analysis was performed after semen liquefaction for 30 min at room temperature. Seminal volume, seminal pH, sperm motility, sperm morphology, and sperm concentration were assessed according to World Health Organization criteria [23].
Sperm DNA fragmentation assessment
The sperm DNA damage was evaluated by Sperm Chromatin Dispersion (SCD) test [24] using the Halosperm® Kit (Halotech Dna, Spain). Briefly, sperm samples from each patient, containing after dilution or concentration not < 5 million and not >10 million spermatozoa per milliliter, were used. The kit contains aliquots of agarose gel in Eppendorf tubes. Each semen sample was processed after the agarose gelled (from immersion in a water bath at 90°C for 5 min). When the Eppendorf tubes reached a temperature of 37°C (5 min at 37°C in a dry atmosphere), 25 μL of sperm were added and gently mixed. Twenty microliters of this mixture were placed on precoated slides and covered with 22x22 mm coverslide. The slides were maintained at 4°C for 5 minutes to produce a microgel containing embedded spermatozoa. The coverslides were gently removed, and the slides were immersed in a previously prepared acid solution (80 μL of HCl added to 10 mL of distilled water) for 7 minutes. After removal from this solution, the slides were incubated for 25 minutes in 10 mL of lysing solution (provided in the Halosperm kit). After rinsing in distilled water, the slides were dehydrated for 2 minutes in three concentration of alcohol (70%. 90% and 100% vol) for 2 minutes each and either were stored (storage was possible several months in optimal conditions) or were processed immediately with staining solution for 10 minutes with continuous airflow. Staining was performed with 1:1 (vol/vol) by using Wright’s solution (Merck, Darmstadt, Germany) and phosphate-buffered saline solution (Merck). The slides were rinsed in tap water, allowed to dry at room temperature, processed for upright o inverted bright-field microscopy at x100, and covered with 22x22 mm coverslide. Operators scored ≥ 500 spermatozoa for each patient according to the patterns established by Fernández et al. [24]. Strong staining is preferred to visualize the dispersed DNA loop halos. Removal of sperm nuclear proteins results in nucleoids with a central core and a peripheral halo of dispersed DNA loops. The sperm tails remain preserved. The acid treatment produces DNA unwinding that is restricted in those nuclei with a high levels of DNA strand breakage. After the subsequent lysis, sperm nuclei with fragmented DNA produce very small or no halos of dispersed DNA. However, nuclei without DNA fragmentation release their DNA loops to form large halos.
Statistical analysis
Statistical analysis was carried out using the statistic package Stata 10 (StataCorp, College Station, TX). Data are represented as Mean ± SD. Group comparisons were made the χ2 test and Student’s t-test. It was considered a statistical significant difference when P<0.05.
A total of 217 seminal samples from infertile men were analyzed regarding the semen parameters and DNA fragmentation. The age of the patients ranged from 21 to 68 years with a mean of 38.45 years. The results were allocated to four age groups:
1. <30 years (26.69 years in average; n=16)
2. 30-39 years (34.69 years in average; n=111)
3. 40-49 years (43.41 years in average; n=78)
4. ≥ 50 years (56.58 years in average; n=12)
The results of the basic semen parameters and DNA fragmentation according to male age are shown in table 1. Parameters of volume, pH and concentration were similar in four evaluated groups (P: NS). Percentages of motility were significantly lower in patient’s ≥ 50 years old compared to the other evaluated groups (P<0.05). The percentages of sperm with normal morphology significantly decrease after 30 years old, as well as the sperm vitality after 40 years olds (P<0.05).
| <30 years (n=16) | 30-39 year (n=111) | 40-49 years (n=78) | ≥ 50 years (n=12) | |
|---|---|---|---|---|
| Age (Mean ± SD) Volume (mL) pH Concentration (x106 /mL) Motility (%) Morphology (%) Vitality (%) DNA Fragmentation (%) |
26.69 ± 2.53 3.93 ± 2.06 7.82 ± 0.32 266.11 ± 184.64 54.01 ± 17.21 4.63 ± 1.42 88.94 ± 5.25 35.59 ± 7.52 |
34.69 ± 2.68 3.22 ± 1.46 7.95 ± 0.37 233.68 ± 200.64 48.29 ± 21.41 3.86 ± 1.73a 81.24 ± 21.01 39.37 ± 8.39 |
43.41 ± 2.72 2.79 ± 1.18 7.86 ± 0.37 240.25 ± 197.17 44.06 ± 22.08 3.52 ± 1.35a 79.69 ± 20.61a 41.99 ± 7.65a,b |
56.58 ± 5.99 2.60 ± 2.18 8.03 ± 0.42 249.09 ± 214.19 38.21 ± 22.64a 3.01 ± 079a,b 77.17 ± 15.32a 47.70 ± 3.89a,b,c |
aP <0.05 in relation to the group <30 years
bP <0.05 in relation to the group 30-39 years
cP <0.05 in relation to the group 40-49 years
Table 1: Descriptive statistics and comparison between four evaluated age groups.
Our data showed that sperm DNA fragmentation increases with advancing age. Thus, the percentages of DNA fragmentation were significantly higher in men from groups 40-49 years old and ≥ 50 years old compared to men from groups <30 years old and 30-39 years old (P<0.05). Also, men ≥ 50 years old had significantly high values of DNA fragmentation compared to men 40-49 years old (P<0.05).
When splitting the patients into a group of Normozoospermic men and a group of men with at least one impaired conventional semen parameter or Infertile men, the two groups were significantly different from each other, concerning the total values of concentration, motility, morphology and DNA fragmentation (P<0.05) (Table 2).
| Age group (years) | N | DNA Fragmentation (%) | Concentration (x 106/mL) | Motility (%) | Morphology (%) |
|---|---|---|---|---|---|
| Normozoospermic | |||||
| < 30 | 12 | 33.84 ± 5.99 | 291.53 ± 189.76 | 60.03 ± 14.52 | 5.04 ± 1.39 |
30-39 |
47 | 33.65 ± 6.36 | 315.86 ± 192.29 | 63.04 ± 9.55 | 5.35 ± 1.17 |
| 40-49 | 31 | 37.38 ± 4.46 | 287.30 ± 192.28 | 61.01 ± 12.79 | 4.55 ± 0.72 |
| ≥ 50 | 1 | 34.60 | 250.50 | 37.90 | 4.00 |
| Total | 91 | 34.92 ± 5.89 | 302.20 ± 189.32 | 61.57 ± 11.61 | 5.02 ± 1.12 |
| Infertile men | |||||
| <30 | 4 | 42.60 ± 11.60 | 189.85 ± 167.59 | 35.93 ± 11.32 | 3.38 ± 0.48 |
| 30-39 | 64 | 43.68 ± 7.46 | 170.36 ± 184.59 | 36.94 ± 21.13 | 2.69 ± 1.07 |
| 40-49 | 47 | 44.63 ± 7.94 | 208.55 ± 196.11 |
32.65 ± 19.57 | 2.81 ± 1.22 |
| ≥ 50 | 11 | 47.70 ± 3.89 | 248.96 ± 224.65 | 38.23 ± 23.75 | 2.91 ± 0.77 |
| Total | 126 |
44.41 ± 7.47a | 192.49 ± 191.58a | 35.40 ± 20.45a | 2.78 ± 1.09a |
aP<0.05 in relation to the Normozoospermic group
Table 2: Descriptive statistics and comparison between patients Normozoospermic an infertile men.
The regression analysis shown a significantly association between age and DNA fragmentation (a; r=0.106; p=0.0001) (Figure 1a), progressive motility (b; r=0.042; p=0.0028) (Figure 1b) as well as morphology (c; r=0.054; p=0.0017) (Figure 1c).
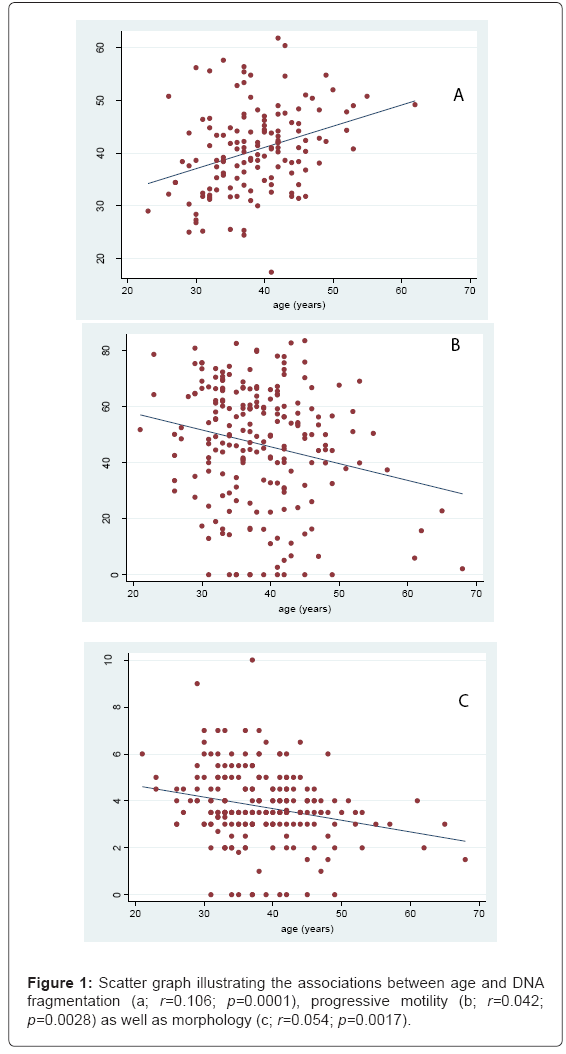
Figure 1: Scatter graph illustrating the associations between age and DNA fragmentation (a; r=0.106; p=0.0001), progressive motility (b; r=0.042; p=0.0028) as well as morphology (c; r=0.054; p=0.0017).
Normal sperm genetic material is required for successful fertilization, as well as for further embryo and fetal development that will result in a healthy offspring. Sperm DNA contributes half of the offspring’s genomic material and abnormal DNA can lead to derangements in the reproductive process.
Recently, there has been growing interest in the use of DNA integrity as a marker of male infertility. Sperm DNA damage has been attributed to a variety of intra and extratesticular factors [25]. The most important is the production of Reactive Oxygen Species (ROS) which is excited by excessive stress, competitive sports, alcohol and drug abuse or nicotine. If produced in abundance, ROS can be enter the cell nucleus, bind to the DNA and cause its fragmentation [26-29]. Several studies have reported that redox balance is deregulated in the ejaculates from infertile males, with glutathione peroxidase 4 being one of the main enzymes involved in this issue [30]. However, DNA fragmentation is also a feature of physiological processes like apoptosis and necrosis [31,32].
During the past two decades a number of tests have been introduced for the analysis of sperm DNA fragmentation. These tests include TUNEL assay [33], Comet assay [34], CMA3 [35], in-situ nick translation [36], DNA breakage detection fluorescence in situ hybridization (DBD-FISH) [37], SCD [24], and the SCSA [38].
In the present study, the presence or absence of DNA fragmentation was determined by examining the halo size by SCD test; a simple, highly reproducible and less expensive technique, yielding results highly correlated with those from other procedures like the DBD-FISH and the SCSA [39].
In Western societies, advanced paternal age is a phenomenon that parallels advanced maternal age and is associated with various reproductive hazards. Testicular function, risk of chromosomal disorders and sperm parameters deteriorate rather gradually with advanced age. Our results found that DNA fragmentation increase by male aging similar to those results observed by Plastira et al. [40] and Vagnini et al. [41]. The patients ≥ 40 years old had spermatozoa with fragmented DNA significantly higher compared to those patients from <30 years old and of 30-39 years old (P<0.05). In some studies, a paternal age-related increase in DNA fragmentation was not observed, but this is probably due to limited sample size [42-44]. Furthermore, the advanced paternal age was associated with a significant decrease in sperm motility and percent normal sperm morphology. Similar results were reported by Levitas et al. [45], Cardona et al. [46], Molina et al. [47] and Brahem et al. [44] while Winkle et al. [42] only reported a decrease in sperm motility.
In males, germ cells divide continuously. It has been estimated that 30 spermatogonial stem cell divisions take place before puberty, when they begin to undergo meiotic divisions. From then on, 23 mitotic divisions per year occur, resulting in 150 replications by the age of 20 years and 840 replications by the age of 50 years [48]. Because of these numerous divisions of stem cells, older men may have an increased risk of errors in DNA transcription. Furthermore, germ cell is also continuously under attack from endogenous and exogenous factors that can induce a wide range of DNA lesions that can be formed under normal processes such transcription, recombination, and replication [49].
On the other hands, one of the main theories of aging states that aging results from an accumulation of unrepaired DNA lesions; such lesions have been routinely linked to aging in many tissues including the brain, the liver and the testis [50,51]. Paul et al. [51] showed that there is an age-related, accumulation of DNA damage in the testis, particularly caused by oxidative stress in the form of 8-oxodG lesions. Furthermore, aging seems to lower the capacity of germ cells to repair such DNA damage, resulting in the production of spermatozoa with increased DNA damage. This is likely to lead to a decline in genome integrity that may be passed on to future generations, specifically the offspring of older males.
In assisted reproduction programmes, several studies shown that high levels of sperm DNA fragmentation are related to lower pregnancies rates either natural or using IUI, IVF and ICSI procedures [52-56] and higher aneuploidies rates in embryos [57-59]. Greco et al. [60] reported 29 ICSI cycles in which the percentage of DNAfragmented spermatozoa, detected by TUNEL assay, was >15%, only two pregnancies and no births were obtained. Muriel et al. [61] and Benchaib et al. [21] shown that the DNA fragmentation level was inversely correlated with fertilization rate, embryo quality to achieve blastocyst stage, and embryo morphological quality. Additionally, high incidence of DNA fragmentation has been frequently observed among infertile couples with unexplained aetiologies and with recurrent pregnancy failures and high abortion rates [62,63].
On the other hand, several techniques have been proposed to select sperm with lower of DNA fragmentation like use of Annexin-V, protein that binds specifically to phosphatidylserine and enables the identification of cells apoptotic [64] and significantly reduce the percentage of spermatozoa with DNA fragmentation, and a sperm selection method based on sperm Hyaluronic Acid (HA) binding [65]. HA-bound spermatozoa show low chromosomal aneuploidies and DNA fragmentation, and good nuclear morphology [66].
Finally, our study demonstrated that increased age in infertile men is associated with an increase in sperm DNA fragmentation and decline in sperm motility and percentage of normal morphology spermatozoa.
The authors thank Mr. Héctor Mendoza-García for kindly reviewing the spelling and syntax in this manuscript.