Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Research Article - (2016) Volume 5, Issue 2
Background: Palatal neoplasm cases in human are very rare. More than 90% neoplasms of the palate is squamous cell type. Not only cytological pleomorphism but also nuclear anomalies are reported to be observed in oral squamous cell carcinoma (OSCC). But, site specific cytological pleomorphisms are not reported so far. Therefore, an attempt has undertaken to investigate the cytopathology of human palatal neoplasms, pattern of cervical lymph node (CLN) metastasis and to analyse the probable etiological risk factors associated with it in the present study.
Methodology: In a hospital-based study, out of 136 oral cases, 9 palatal cases (6 male and 3 female) registered during May 2007 to May 2009 were included in this study. Detail case-history including the nature and types of addiction of each individual was recorded prior to the collection of samples. Two scraped exfoliated cytosmears were collected from the affected site on the pre cleaned-coded glass-slides. Collected cytosmears were immediately fixed in 1:3 aceto-alcohol (1 part of glacial acetic acid and 3 parts of ethyl alcohol). One set of smears was stained with Papanicolaou’s stain and the other was counter-stained with Giemsa’s stain for cytopathological analysis. American Joint Committee for Cancer Staging and End-Results Reporting (AJC) formulated TNM (Tumor-Node-Metastasis) System for staging of OSCC was followed.
Result: Cytopathologically, a number of pleomorphic cytological atypias, such as, keratinized spindle cell (KSC), keratinized tadpole cell (KTC), keratinized strap (Antischkow) cell (KSC-A), large and small keratinized fiber cells (KFC), large and small keratinized round cells (KRC), micronucleated cell (MNC), plump keratinized squamous cell (PKSC) and non-keratinized malignant squamous cell (NMSC) were observed in such palatal neoplasms. Except NMSCs, all other cells were keratinized. Out of these, PKSC and MNC were well differentiated; KSC, KTC, KFC, KRC and KSCA were moderately differentiated and NMSC was poorly differentiated. Interestingly, in addition to the micronucleated cell (MNC), KSC-A was found to be a modal cytological atypia irrespective of age, site, sex and degree of pathogenicity which may be attributed to the addiction of tobacco in general and smoking in particular.
Conclusion: Chewing and smoking of various form of tobacco and drinking of alcohol contribute a lot to the genesis of cytological pleomorphism in human palatal neoplasm. Typically atypical cells like KSC, KTC, KSC-A, KFC, KRC, PKSC, MNC and NMSCs although found less in number, modal occurrence of KSC-A along with the MNC in all the palatal neoplasm may be directly correlated with any form of tobacco smoking.
Keywords: Exfoliated cytosmear; Palatal neoplasm; Cytological pleomorphism; Addiction
Human palatal neoplasm is rare. It accounts for 5% to 15% of intraoral carcinomas, depending whether it is on the hard or soft palate [1]. Clinically, palatal neoplasm manifests itself as a poorly defined, ulcerated, painful lesion on one side of the midline. Sometimes, it may crosses the midline and extend from the upper gingivo-alveolar area to the tonsillar pillar or even the uvula of the oral cavity [2]. On the basis of origin, epidermoid carcinoma, adenocarcinoma, and benign mixed tumors are more common than melanoma, lymphosarcoma and myosarcoma to the palate of oral cavity [3]. Generally, most cancers of the palate are uncommon and squamous cell carcinoma (SCC) type [4]. Cytological pleomorphism is well observed in oral squamous cell carcinoma (OSCC) [5]. However, site specific cytological pleomorphisms are not reported so far. Therefore, an attempt has undertaken to investigate the frequency of pleomorphic cytological atypias in the exfoliated cytosmears of human palatal neoplasms, pattern of cervical lymph node (CLN) metastasis and to analyse the probable etiological risk factors associated with it in the present study.
In a hospital-based study, out of 136 oral cases, 9 (6.62%) palatal cases (6 males and 3 females) registered during May 2007 to May 2009 were included in this study. Detailed case-history including the nature and types of addiction of each individual was recorded prior to the collection of samples. Two scraped exfoliated cytosmears were collected from the affected site on the pre cleaned-coded glass-slides. Collected cytosmears were immediately fixed in 1:3 aceto-alcohols (1 part of glacial acetic acid and 3 parts of ethyl alcohol). A set of smears was stained with Papanicolaou’s stain and the other set was counterstained with Giemsa’s stain for cytopathological analysis. Out of 1000 observed cells, the cytological atypias were scored and evaluated.
American Joint Committee for Cancer Staging and End-Results Reporting (AJC) formulated TNM (Tumor-Node-Metastasis) System for staging of OSCC was followed [6].
The cases: Clinical aspects
Out of 136 oral cases, 9 (6.62%) palatal cases (6 male and 3 female) were included in this study, who were registered at the Out-Patient Department of Achaya Harihar Regional Cancer Centre (AHRCC), Cuttack, the only Government Hospital dedicated for the treatment of cancer patients in Odisha, during May 2007 to May 2009. Detailed case-history (including age, sex and clinical out-put) of the patients was summarised in Table 1. The age of the patients was ranged from 32 to 83 years with an average of 53 ± 15.85 years. Clinically, out of such nine palatal cases, 5 (55.6%) were suffered from exophytic ulcerative tumour, 2 (22.2%) with exophytic tumour without any ulceration, and the rest 2 (22.2%) with erythroplakia. Except case no-5, i.e., only in one case (11.1%), entire left part of the hard palate (≥ 2.5 cm) and <1 cm of the anterior end of the soft palate was affected and all the rest 8 (88.9%) cases, the lesions were absolutely restricted to the hard palate with a lesion of ≥ 2 cm in diameter in each case (Figure 1).
| Case No. | Age | Sex | Specific Site | Lesion Size | LesionType | Cytological Atypias | Addiction | Metastasis if any |
TNM staging* |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 58 | Female | Hard Palate | ≥2 cm | Erythro-leucoplakia | PKSC, MNC, KSCA, NMSC | Chewing, Smoking, Drinking | Cervical Lymph Node (CLN), Single, left, Contra-lateral | T0N1M0/Stage 0 |
| 2 | 46 | Male | Hard Palate | ≥2.5 cm | Exophytic tumour | PKSC, MNC, KSCA | Smoking | Absent | T1N0M0/Stage I |
| 3 | 37 | Male | Hard Palate | ≥2 cm | Exophytic tumour | PKSC, MNC, KSCA, NMSC | Chewing, Smoking, Drinking | CLN,Single, left, Contra-lateral | T1N1M0/Stage III |
| 4 | 66 | Female | Hard Palate | ≥2 cm | Exophytic Ulcerative tumour | KSC, MNC, KSCA,KRC, KFC | Chewing, Smoking | CLN, Multiple,Right, Contra-Lateral | T1N2cM0/Stage IVA |
| 5 | 32 | Female | Hard-Soft Palate | ≥2.5 cm | Exophytic Ulcerative tumour | KSC, MNC, KSCA, KRC, KFC, NMSC | Chewing, Reverse Smoking, Drinking | CLN, Multiple Ipsilateral | T1N2bM0/Stage IVA |
| 6 | 45 | Male | Hard Palate | ≥2.6 cm | Erythroplakia | PKSC, MNC, KSCA | Chewing, Smoking | CLN, Single, Right, Contra-lateral | T1N1M0/Stage III |
| 7 | 83 | Male | Hard Palate | ≥3.5 cm | Exophytic Ulcerative tumour | MNC, KSCA, NMSC | Chewing, Smoking, | CLN, Multiple,bi-lateral | T1N2cM0/Stage IVA |
| 8 | 62 | Male | Hard Palate | ≥2.5 cm | Exophytic Ulcerative tumour | KSC, MNC, KSCA,KRC, KFC, NMSC | Chewing, Smoking | CLN, Single, Right, Contra-lateral | T1N1M0/Stage III |
| 9 | 48 | Male | Hard Palate | ≥3 cm | Exophytic Ulcerative tumour | KSC, MNC, KSCA,KRC, KFC, NMSC | Chewing, Smoking | CLN, Multiple,Right, Contra-lateral | T1N2cM0/Stage IVA |
Table 1: Age, sex and addiction-wise clinical features and diagnostic cytological atypias in nine cases with palatal neoplasm. * American Joint Committee for Cancer Staging and End-Results Reporting. Chicago: American Joint Committee on Cancer, 2002.
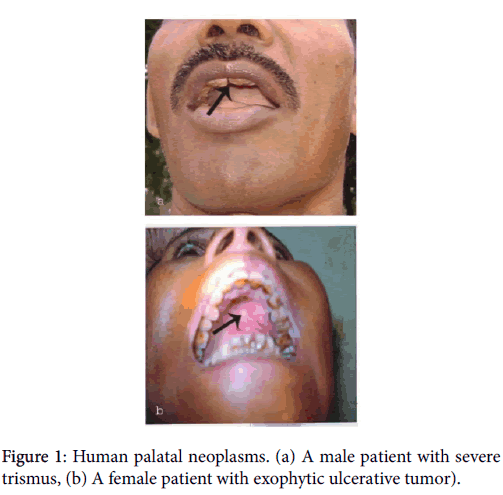
Figure 1: Human palatal neoplasms. (a) A male patient with severe trismus, (b) A female patient with exophytic ulcerative tumor).
Regional or Cervical lymph node (CLN) metastasis was observed in 8 (88.9%) cases and absent in 1 (11.1%) case only. Out of 8 cases, 2 with single CLN on left Contra-lateral, 2 with single CLN on right Contra-lateral and 4 with multiple CLNs of which 2 with CLNs on right Contra-lateral, 1 with CLN on bi-lateral and 1 with CLNs on ipsilateral in position. No distant metastasis was observed in these palatal cases.
The TNM (Tumor-Node-Metastasis) system formulated by the American Joint Committee for Cancer Staging and End Results Reporting (AJC) is generally followed for the staging of SCC of the oral cavity [6]. Tumor (T) staging is based on the size of the primary tumor. Nodal (N) staging is also based on size and site or location. Metastasis (M) staging refers to the absence (M0) or presence (M1) of distant metastasis. On the basis of TNM staging, Case-1 was recorded to be at Stage 0, Case 2 with Stage I, 3 cases (Case-3, 6 and 8) with Stage-III and the rest 4 cases (Case 4, 5, 7 and 9) were in Stage- IVA. Except Case 1, all 8 cases were found to be in potentially advanced stage of palatal neoplasm, so far as oral carcinogenesis is concerned.
Almost all the patients were smokers. Smoking of bidi was a common practice among all the palatal cases. Out of 9 cases, 4 (44.4%) patients were addicted to chewing and smoking of tobacco and the rest 5 (55.6%), in addition to chewing and smoking of tobacco, were also addicted to drinking of different forms of alcohol for more than 15 years. Chewing of paan, betel-quids and gutkha were predominantly observed in the younger generation- particularly in the age group of 30-49 years in our study. Along with khaini and oral snuff-dipping, regular drinking of handia (a fermented form of boiled rice) and mahuli (a fermented form of boiled mohua flower) was a routine life of the alcoholics. However, a lady of 32 years (Case No. 5), from Ganjam District of Odisha, besides chewing of tobacco and drinking of homemade alcohol and tadi (a fermented form of palm tree juice) was also habituated with reverse smoking.
Oral squamous cell carcinoma exhibits a high degree of cytological plomorphism with no exception to the palatal neoplasm. Cytopathologically, a number of pleomorphic cytological atyias, such as, keratinized spindle cell (KSC), keratinized tadpole cell (KTC), keratinized strap (Antischkow) cell (KSC-A), large and small keratinized fiber cells (KFC), large and small keratinized round cells (KRC), micronucleated cell (MNC), plump keratinized squamous cell (PKSC) and non-keratinized malignant squamous cell (NMSC) were observed in such palatal neoplasms. Except NMSCs, all other cells were keratinized. Out of these, PKSC and MNC were well differentiated and the later was proved to be a potential onco-indicator during oral carcinogenesis; KSC, KTC, small and large KFCs, small and large KRCs and KSCA were moderately differentiated and NMSC was poorly differentiated (Figure 2).
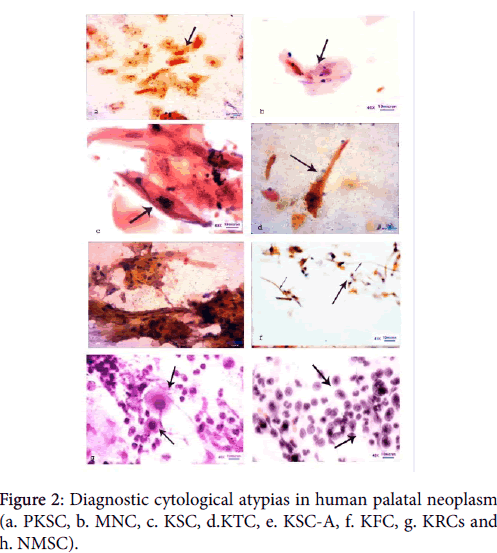
Figure 2: Diagnostic cytological atypias in human palatal neoplasm (a. PKSC, b. MNC, c. KSC, d.KTC, e. KSC-A, f. KFC, g. KRCs and h. NMSC).
Numerically, a total of 1756 atypias from 6 male and 1388 atypias from 3 female sample were recorded (Table 2). Number of NMSCs was recorded to be the highest whereas SKFCs were found to be the lowest (Figure 3). It is important to note that in addition to the micronucleated cell (MNC), KSC-A was observed to be a modal atypia irrespective of age, sex and degree of pathogenicity which may be attributed to the addiction of tobacco in general and smoking in particular. The highest relative percentage of atypias was recorded to be 57% in the age group of 30-49 years in male and 67.9% in the age group of 50-69 years in female (Figure 4).
| Age groups in years | No. of samples | KSC | KTC | KSC-A | LKFC | SKFC | LKRC | SKRC | MNC | PKSC | NMSC | Total (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | |
| 30-49 | 4 | 1 | 16 | 9 | 5 | 4 | 12 | 12 | 7 | 5 | Nil | 1 | 6 | 2 | 4 | 3 | 18 | 4 | 265 | 138 | 668 | 267 | 1001(57.0) | 445 (32.1) |
| 50-69 | 1 | 2 | 8 | 19 | 6 | 10 | 6 | 16 | 2 | 10 | 2 | 4 | 2 | 4 | 4 | 5 | 8 | 14 | 114 | 297 | 203 | 564 | 355 (20.2) | 943 (67.9) |
| 70-89 | 1 | Nil | 10 | Nil | 6 | Nil | 7 | Nil | 3 | Nil | Nil | Nil | Nil | Nil | 6 | Nil | 10 | Nil | 124 | Nil | 234 | Nil | 400 (22.8) | Nil |
| Total | 6 | 3 | 34 | 28 | 17 | 14 | 25 | 28 | 12 | 15 | 2 | 5 | 8 | 6 | 14 | 8 | 36 | 18 | 503 | 435 | 1105 | 831 | 1756 | 1388 |
Table 2: Age group and sex-wise enumeration of diagnostic cytological atypias in human palatal neoplasm (M-Male, F-Female). Figures in parentheses indicate the relative percentage with respect to the total number of atypias scored.
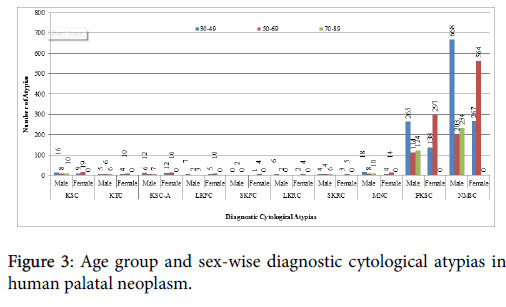
Figure 3: Age group and sex-wise diagnostic cytological atypias in human palatal neoplasm.
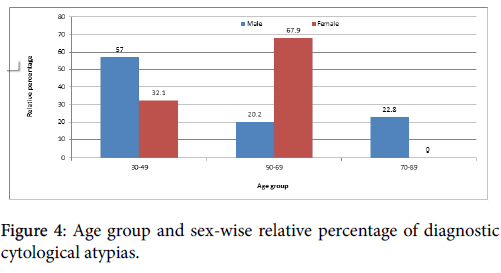
Figure 4: Age group and sex-wise relative percentage of diagnostic cytological atypias.
The palate is commonly called as the roof of the oral cavity. Anatomically, it is divided into the hard palate (part of the oral cavity) anteriorly and the soft palate (part of the oropharynx) posteriorly. Palate harbours a variety of neoplasms. Generally, epidermoid carcinoma, adenocarcinoma, and benign mixed tumors are more common than melanoma, lymphosarcoma and myosarcoma to the palate [3]. SCC of the palate accounts for 5% to 15% of intraoral carcinomas, depending whether it is on the hard or soft palate. More than 90% neoplasms of the palate are squamous cell type. [1]. Out of 136 oral cases, only 9 (6.62%) palatal cases (6 male and 3 female) were included in this study. Findings indicate that palatal neoplasm is a rare type of malignancies which corroborates the earlier findings [1,4].
Unlike other parts of the oral cavity, it is practically too difficult to differentiate a benign tumor from a malignant one in the palatal region [3]. Sometimes, a malignant tumor may mimic to be a benign one and vice versa [7] as maximum numbers of cytological atypias are observed to be either well differentiated or moderately differentiated [8]. Really, a transitional state of cellular alteration creates an ambiguity and brings about a diagnostic dilemma. As in the case of case no. 1, who was reported to be precancerous and in Stage 0 (T0N1M0), presence of NMSC along with other cytological atypias in her exfoliated cytosmear indicates a clear malignancy [9]. However, along with the MNCs few moderately differentiated cells (KSC, KSCA, KRC and KFC) were observed in case No-4 (T1N2cM0) who was recorded to be in Stage IVA. Martin probably had observed such metamorphic transitional state in the cellularity during progression from benign tumors to cancer in palate [3].
There are varieties of symptoms of palatal cancer such as lumps, painful swelling and ulcers in mouth resulting in an uneasy and uncomfortable swallowing of food. Other symptoms like night sweating and weight loss are found in such cases. The mouth may become difficult to open, a condition called trismus. Speech patterns may change and some words may become hard to pronounce properly. As with many cancers, the symptoms of palate cancer become intensified and more if not detected at an early stage.
Although tobacco [10] and alcohol [11] are found to be the main culprits in oral carcinogenesis, their role in the genesis of neoplasm at hard palate is doubtful. However, the growing evidences indicate that reverse smoking is a specific etiologic factor for SCC of the hard palate. In reverse smoking, the practice of holding the lit end of the bidi, cigarette or chutta in the mouth causes smoke to hit the hard palate directly so that an intense heat is generated during smoking [12]. Reverse smoking is being predominantly observed among the females of Srikakulam district of Telengana (earlier in Andhra Pradesh) and Ganjam district of Odisha State. Reddy observed that the prevalence of hard palate neoplasm was more (73.8%) in females at younger age than males and the estimate risk was 132 times greater in women who smoked chuttas in reverse than in other women [13]. In an epidemiological study, Gavarasana and Susarla have found that the frequency of reverse smoking was 6.23 times higher in females than in males [14]. In a cross-sectional study in rural Andhra Pradesh have reported that the prevalence rate of palatal lesions was 55% due to reverse smoking of chutta [15].
It has also been demonstrated that there is a close relation between reverse smoking, nicotina somatitis and carcinoma of hard palate. The intense heat generated by smoking causes changes in the oral mucosa - typically on the hard palate. The stem of the pipe increases the amount of heat directed at the hard palate, resulting in a higher incidence of nicotine stomatitis in pipe smokers [16]. Quigly et al. have found that besides carcinogens in smoke, the high temperature (76°C) of the burning cigar is believed to be the causal factor of palatal cancer [17]. Rizzolo and Chiodo have reported that the severity and extent of the lesion is directly proportional to the frequency of tobacco inhalation. They have emphatically stated that it is not the chemicals in the tobacco, but the heat generated by the burning lit is responsible for the mucosal changes in the palate [18]
Alcohol is classified as a carcinogen by the International Agency for Research on Cancer (IARC). Alcohol, acting both independently as well as synergistically with smoking has been implicated in oral carcinogenesis [19]. More importantly, alcohol may act as a solvent and enhance the penetration of carcinogens into the target tissues. Ethanol acts locally and become a cause of epithelial atrophy which increases the penetration of carcinogens through the oral mucosa. It has been observed that more the concentration of ethanol, greater is the permeability and sooner is the epithelial atrophy [20]. Acetaldehyde-a primary metabolic product of alcohol (ethanol) is found to be genotoxic and carcinogenic [21].
The combined and interactive effects of tobacco use and alcohol consumption are found to be multiplicative. Smoking increases the acetaldehyde burden following alcohol consumption and alcoholdrinking enhances the activation of pro-carcinogens present in tobacco. Compared with persons who neither drink nor smoke, the risk of developing OSCC is increased 80 fold in persons with the highest level of tobacco smoking and alcohol drinking [22]. Mohanta et al. have earlier reported that the combined effect of tobacco and alcohol was found to be more genotoxic than the single use on the buccal mucosal cells [23]. In the present study, all cases were mostly bidi smokers. Among them, one female was habituated with the reverse smoking in the form of chutta. Not only the patients were addicted to chewing of tobacco but also habituated with drinking of alcohol. In this study, it is presumed that the carcinogens present in the smoke of tobacco and alcohol play a major role in the development of palatal neoplasm. Also, the pyrogenicity of tobacco smoke and volatile as well as dehydrating nature of alcohol probably accelerate a drastic cellular alternation and carcinogenesis in the palate of oral cavity.
Several studies on the metastasis of SCC of the tongue and floor of mouth have been reported [24]. Only a few studies are there related to the metastasis of hard palate neoplasm [25-27]. Mukherji et al. have reviewed the expected lymphatic drainage of various sub-sites of the upper aerodigestive tract and emphasized that tumors attain the lymphatic drainage associated with their primary location. Tumors that cross the midline to the contralateral side or spread to adjacent subsites will acquire the lymphatic drainage associated within these areas [28]. Rouviere described three separate drainage pathways for the soft palate, anterior, middle, and posterior [29,30]. Although both the anterior and posterior pathways are potential drainage pathways for the soft palate, the posterior pathway is the more common pathway for the soft palate lesions while the anterior pathway is more common for hard palate tumors. Aydil et al. have reported that the most common neoplasms of the hard palate were minor salivary gland tumors (MSGTs). SCCs were relatively rare in their series. Although threefourth of neoplasms was at an advanced stage, neck metastasis was not a characteristic of malignant epithelial neoplasms located in the hard palate [31].
In the present study, CLN metastasis was observed in 8 (88.9%) cases and absent in 1 (11.1%) case only. Out of 8 cases, 2 with single CLN on left Contra-lateral, 2 with single CLN on right contra-lateral and 4 with multiple CLNs of which 2 with CLNs on right contralateral, 1 with CLN on bi-lateral and 1 with CLNs on ipsilateral in position. No distant metastasis was observed in these palatal cases.
Guggenheimer et al. have reported that there was a delay in diagnosis of months to years in many patients lead to regional as well as distant metastasis [32]. It is important to note that all the cases included in our study were the referral cases and first time registered for the treatment in AHRCC, Cuttack, Odisha. They had neither undergone radiotherapy nor surgery nor chemotherapy earlier. From this study, it is presumed that not only delayed in diagnosis, but also the period and amount of consumption of carcinogenic substances (such as tobacco and alcohol) play a vital role in oral carcinogenesis followed by metastasis. Colombo et al. have described an extremely rare case of an oral metastasis limited to the hard palate mucosa and gingiva that was originally diagnosed and treated as a periodontal inflammatory disease, but subsequently proved to be the first manifestation of a gastric carcinoma [33].
With regard to the CLN metastasis, several workers have detected some important molecular markers associated with microvascular angiogenesis and lymphogenesis. These molecular markers primarily act as the promoters of regional lymph node metastasis in many cancers [33]. Vascular endothelial growth factor (VEGF) positivity is the most significant predictor of poor prognosis and thus its expression may prove to be an important prognostic factor in head and neck cancer [34]. Matrix metalloproteinases (MMP) especially MMP-1 and integrin-3, can provide an accurate biomarker for predicting the risk of CLN metastasis in OSCC [35]. Li et al. evaluated the impact of CLN metastasis on the survival of patients with SCC of the hard palate. They reported that the presence of CLN in patients was associated with the decreased survival rates. They also proposed that SCC of the hard palate should be treated aggressively, and elective neck dissection should be considered because of the high rate of cervical metastasis [36].
Among the intra-oral neoplasms, the palatal neoplasm poses a difficult diagnostic dilemma for the clinician as well as the oncopathologists [36]. Clinically indistinguishable neoplasm may mimic to be a benign one, but cytopathologically the patient might be in an advanced stage. Chewing and smoking of various form of tobacco and drinking of alcohol contribute a lot to the genesis of cytological pleomorphism in human palatal neoplasm. Typically atypical cells like KSC, KTC, KSC-A, KFC, KRC, PKSC, MNC and NMSCs although found less in number, modal occurrence of KSC-A along with the MNC in all the palatal neoplasm may be directly correlated with any form of tobacco smoking. The carcinogens present in the smoke of tobacco and alcohol play a major role in the development of palatal neoplasm. Also, the pyrogenicity of smoke and volatile as well as dehydrating nature of alcohol may accelerate a drastic cellular alternation followed by carcinogenesis in the palate of oral cavity. To conclude, the stage of advancement of oral SCC at the time of diagnosis is the most important prognostic factor. Presence of any such cytological atypias in the exfoliated palatal cytosmear is practically helpful in determining the stage of the palatal neoplasm. However, the role of tobacco and alcohol in connection to unusual CLN metastasis with particular reference to the palatal neoplasm needs further research.
The authors are thankful to Prof. Gadadhar Parida, M.D, formerly Professor and Head, Department of Oncopathology, Acharya Haihar Regional Cancer Centre (AHRCC), Cuttack, Odisha, India for his guidance and supervision during cytopathological analysis. We are also indebted to the Head P.G. Department of Zoology, Utkal University, Vani Vihar, Bhubaneshwar, Odisha, India and to the Director, AHRCC, Cuttack, Odisha, India for permitting us to collect samples from oral cancer patients and also for providing library and laboratory facilities. One of us (AM) is grateful to the University Grants Commission (UGC), New Delhi, India for awarding UGC Meritorious Research Fellowship to carry out the research work.