Journal of Defense Management
Open Access
ISSN: 2167-0374
ISSN: 2167-0374
Research Article - (2013) Volume 0, Issue 0
Background: Hyperbaric Oxygen Therapy (HBOT) involves the administration of pure oxygen under high pressure conditions. HBOT is used as an adjuvant therapy for a variety of conditions; including chronic wounds, infections, stroke, tissue transplantation, anemia, cancer management, skin flaps & grafts, CO poisoning, air or gas embolism, decompression thickness, necrotizing fasciitis, crush injury, compartment syndrome, gas gangrene and autism.
Objective: This prospective study was designed to evaluate the efficacy of HBOT as adjuvant treatment for diabetic foot ulcers in comparison to the conventional treatment.
Patients and methods: This study comprised 82 diabetic patients, aged 38 to 72 years. Patients were randomized into two groups: Group A assigned to receive HBOT in combination with conventional wound care & group B received conventional wound care only for the treatment of diabetic foot ulcers. Outcomes were measured every week for 1st two months during the treatment period and then at three-month intervals for one year. Ulcers were graded using Wagner classification system. Both groups were compared as regards healing time, need of amputation, quality of life.
Results: The demographic characteristics of the 82 patients were 28 women (34%) and 54 men (65.9%), age range from 32 to 72 years. The median ulcer duration for both groups was 7.2 months, and the median ulcer area was 3.5 cm2. There was non-significant difference between both groups as regard demographic characteristics. Complete healing of the index ulcer was significantly faster in hyperbaric group 50% in comparison to 29% in group B. 2 major amputation were performed in HBOT group as compared to 3 cases in group B; all of them were Wagner grade IV. Five minor amputations were performed in each group during the 1st year of follow up. 63% of group A were satisfied as regard the management of their ulcers in comparison to 41% in group B.
Conclusion: This study supports the role of HBOT as an adjuvant in healing of diabetic foot ulcers & improving quality of life.
Keywords: Hyperbaric oxygen therapy; Diabetic foot ulcers
Diabetic foot ulcers are a major complication that affects 4-10% of the diabetic population [1]. The major causes of these ulcers are ischemia/hypoxia, neuropathy, and infection, and they often coexist. Treatment often requires long-term hospital admissions and frequent outpatient visits [2,3]. Furthermore, loss of mobility poses a great burden on the patient and the health care system [4]. At centers of excellence, 19-35% of diabetic ulcers are reported as non-healing & 12% progress to lower extremity amputation [5-7]. Thus for foot ulcers, there is still a need for new treatment strategies beside conventional therapy.
Hyperbaric Oxygen Therapy (HBOT) defined as breathing 100% oxygen at pressures higher than normal atmospheric pressure at sea level in a hyperbaric chamber [8]. For hyperbaric oxygen, pressure is expressed in multiples of the atmospheric pressure at sea level, which is 1 atmosphere (1 atmosphere is 14.7 pounds per square inch, 1 kg per square centimeter, or 760 mm Hg). Since oxygen has an important role in the physiology of wound healing, HBOT is a useful adjunct in the treatment of diabetic foot ulcers [8-10]. Moreover, HBOT has been reported to have other effects on wound healing: it reduces the progression and accelerates the regression of atherosclerosis in animal models; enhances neutrophil killing ability, stimulates angiogenesis and enhances fibroblast activity and collagen synthesis [11-13].
This study was designed to evaluate the efficacy of HBOT as adjuvant treatment for diabetic foot ulcers in comparison to the conventional treatment.
This double blind prospective comparative & pilot study was conducted in General Surgery Department & Hyperbaric Unit, Armed Forces Hospital Program-Jubail; Saudi Arabia, from the period 2007 till 2013 and comprised 82 diabetic patients, aged 38 to 72 years. Patients were randomized into two groups: Group A assigned to receive HBOT in combination with conventional wound care and group B received conventional wound care only for the treatment of diabetic foot ulcers.
All patients underwent full clinical examination, preoperative duplex on lower limb and vascular assessment. Inclusion criteria of the study were: non-healed diabetic foot ulcer (for at least 4 weeks) grade II-IV according to Wagner [14] classification; adequate distal arterial perfusion. Exclusion criteria of the study were: 1-Impending amputation; 2-Exposed calcaneous bone with no prospect of weight bearing potential; 3-Medical conditions which preclude safe HBOT e.g. clinical depression, severe dementia, previous thoracic surgery, previous spontaneous or trauma induced pneumothorax, history of congestive heart failure, unstable angina, chronic sinusitis, major ear drum trauma, severe arthritis or morbid obesity; 4-Major large vessel disease, or patients, who undergone vascular surgery or angioplasty within the last 3 months; 5-Women who are currently pregnant or are breast feeding or women of child bearing potential who are not currently taking adequate birth control.
Wound care is standardized throughout the entire study to several different dressing types e.g. simple gauze, sitosterol dressing or alginate, collagen/oxidized cellulose dressing; dependent on the type of the wound (dry, wet or infected). The frequency of wound dressings changed as required by the standard care, based on the characteristics of the wound. Clinical signs of infection are noted and antibiotic theory initiated if required and swabs obtained. Debridement was done if needed.
Patients in group A received their HBOT in multi-occupant hyperbaric chamber at 2.5 atmospheres, and patients breathe from individual masks which supply 100% oxygen and remove the exhaled gas. The duration of each session is 90 minutes for 5 days a week.
Follow-up schedule
Outcomes were measured every week for 1st two months during the treatment period and then at three–month intervals for one year. Ulcers were graded using Wagner classification system. Both groups were compared as regards healing time, need of amputation, quality of life.
Healing of foot ulcers was defined as complete healing of the index ulcer. The index ulcer was defined as the ulcer with largest area and duration of at least three months at the time of inclusion. An ulcer was considered healed when it was completely covered by epithelial regeneration and remained so until the next visit in the study. Wagner grade IV ulcers were considered healed when the gangrene had separated and the ulcer below was completely covered by epithelial regeneration.
If a major amputation (above ankle) was required, the ulcer was considered non-healed. The decision to amputate is made by a vascular surgeon and by meeting any of the following criteria: Persistent deep infection involving bone and tendons; ongoing risk of severe systemic infection related to the wound; inability to bear weight on the affected limb and pain causing significant disability.
If the patient died during the follow-up period, she/he was censored at the time of the death. For determination of psychological and physical welfare a disease-specific questionnaire-diabetic foot ulcer scale, performed at baseline and after 8 weeks.
Wagner classification of diabetic foot ulcer
Grade I: Superficial lesions
Grade II: Deep ulceration reaching tendons and bone
Grade III: Involvement of deep tissues with infection
Grade IV: Gangrene of a portion of the foot
Grade V: Gangrene of the whole foot, usually amputation is required
Statistical analysis
Data were analyzed using t-test and Chi-square test. Results of postoperative questionnaires were analyzed. Statistical analysis was conducted using the SPSS (Version 10, 2002) for Windows statistical package. P value <0.05 was considered statistically significant.
During the inclusion period a total of 95 participation were registered, 13 were excluded according to the study protocol, so 82 patients underwent randomization into 2 groups: group A, patients received HBOT in combination with conventional wound care for treatment and group B, patients received conventional wound care only; each group was 41 patients.
The demographic characteristics of the 82 patients were 28 women (34%) and 54 men (65.9%), age range from 32 to 72 years. The median ulcer duration for both groups was 7.2 months, and the median ulcer area was 3.5 cm2. Vascular surgery was previously performed in the affected lower limb in 17 (20.7%) patients. There was non-significant (P value >0.05) difference between both groups as regard demographic characteristics at base time (Table 1).
| Group A No (41) | Group B No (41) | P value | |
|---|---|---|---|
| Age (years) | 57 (38-69) | 55 (39-72) | ns |
| Female (%) | 12(29) | 16(39) | ns |
| Male (%) | 29(71) | 25(61) | ns |
| Mobility: | |||
| Walking without support (%) | 65 | 62 | ns |
| Walking with support (%) | 23 | 27 | ns |
| Wheel chair (%) | 12 | 11 | ns |
| Diabetes duration, mean ( years) | 19±5.8; range 2-29 | 21±3.2; range 3-35 | ns |
| Diabetes Type ½ (%) | 36/64 | 39/61 | ns |
| Index ulcer size(cm2) | 3.7; range 2-51 | 3.5; range 3-40 | ns |
| Ulcer duration ,mean (months) | 6±8.2; range 3-43 | 7±4.7; range 3-40 | ns |
| Wagner classification: | |||
| Grade II (%) | 59 | 55 | ns |
| Grade III (%) | 23 | 30 | ns |
| Grade IV (%) | 13 | 15 | ns |
| Index ulcer location: | |||
| Toe (%) | 29 | 35 | ns |
| Planter forefoot (%) | 25 | 21 | ns |
| Middle Foot (%) | 12 | 17 | ns |
| Heel (%) | 7 | 9 | ns |
| Malleoli (%) | 8 | 6 | ns |
| Dorsal (%) | 3 | 0 | ns |
| Previous vascular surgery (%) | 17.1 | 24.3 | ns |
| Prior major amputation (%) | 11 | 9 | ns |
| Prior minor amputation (%) | 34 | 36 | ns |
ns: non-significant, major amputation: above ankle
Table 1: The demographic characteristics of the patients enrolled in the study.
As regard HBOT 26 patients (63.4%) completed more than 40 treatment sessions, 34 (82.9%) completed >30 sessions, and 5 (12%) completed <10 treatment sessions. One patient received 18 sessions of HBOT and another patient 26 sessions. Early treatment (of HBOT) termination was due to claustrophobia in two patients, death in two patients and one patient underwent major amputation. Open vascular surgery in the affected lower Limb was not performed on any patient in both groups during 1st year follow up, but percutaneous angioplasty was carried out in 5 patients (3 in group A and 2 in group B).
Complete healing of the index ulcer was significantly faster (P=0.03) in hyperbaric group 50% in comparison to 29% of those treated with conventional wound care only, after one year follow up (Figure 1).

Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies.
Four participants, 2 in HBOT group and 2 in conventional wound care group died during the 1st year of follow up. In HBOT, one died after 5 sessions and the other after 9 sessions, in group B, 2 patients died, one after 3 months and the other after 7 months.
Two major amputations were performed in HBOT group as compared to 3 cases in group B; all of them were Wagner grade IV. Five minor amputations were performed in each group during the 1st year of follow up.
26 (63%) patients of group A were satisfied as regard the management of their ulcers in comparison to 17 (41%) patients in group B (P<0.01). Figures 2-6 show limb salvage in five diabetic patients in HBOT group.
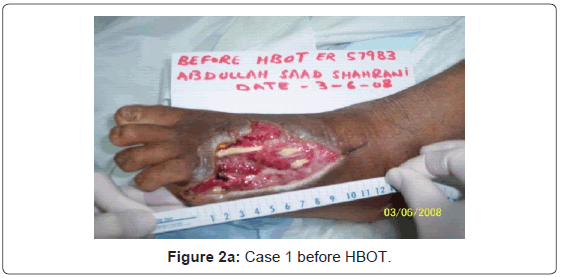
Figure 2a: Case 1 before HBOT.
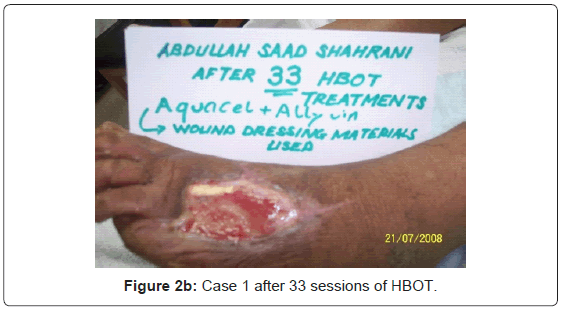
Figure 2b: Case 1 after 33 sessions of HBOT.
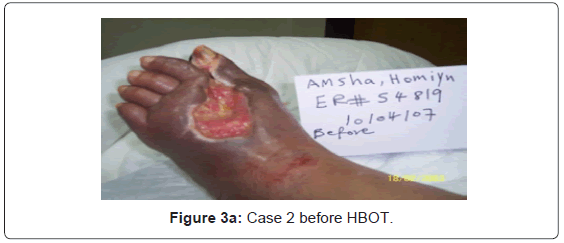
Figure 3a: Case 2 before HBOT.
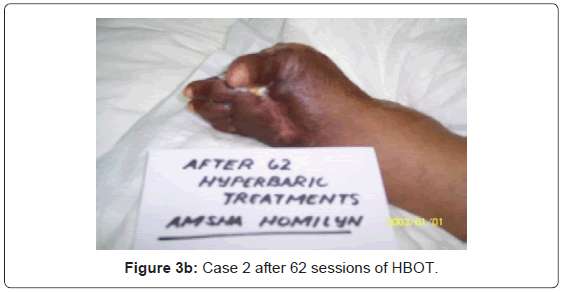
Figure 3b: Case 2 after 62 sessions of HBOT.
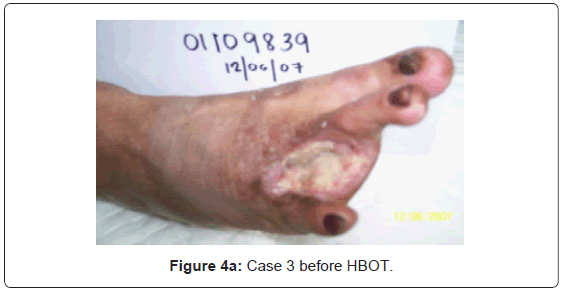
Figure 4a: Case 3 before HBOT.

Figure 4b: Case 3 after 42 sessions of HBOT.
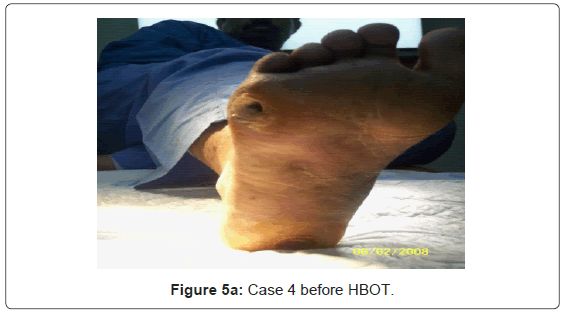
Figure 5a: Case 4 before HBOT.
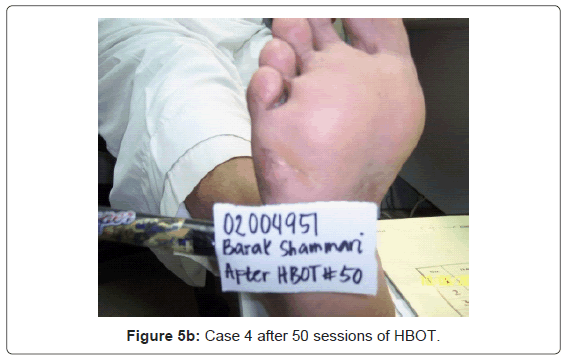
Figure 5b: Case 4 after 50 sessions of HBOT.
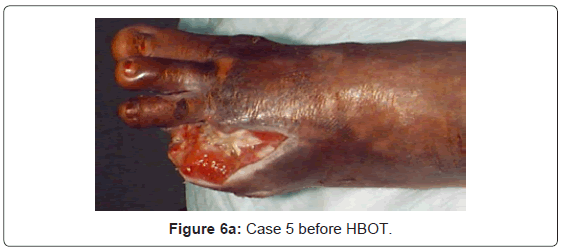
Figure 6a: Case 5 before HBOT.

Figure 6b: Case 5 after 60 sessions of HBOT.
Wound healing has been shown to be delayed in patients with diabetes and particularly in patients with diabetic foot ulcers [15]. Peripheral neuropathy, peripheral vascular disease, and poor glycemic control in conjunction with minor foot trauma increase the likelihood that patients with diabetes will develop foot ulcers [16]. Between 5 and 10% of diabetic patients have or have had such foot ulcerations, with approximately 1% requiring lower extremity amputation. The risk of amputation for those patients is greater than for the non-diabetic population [15,17].
HBOT involves the administration of 100% oxygen under high pressure conditions. HBOT is used as an adjuvant therapy for a variety of conditions; including chronic wounds, skin flaps, infections, edema, stroke, tissue transplantation, anemia, cancer management and war injuries e.g. gas gangrene, crush injuries, blast injuries chronic traumatic brain injury and, decompression sickness. HBOT is known to improve antibacterial defenses, increase blood flow, reduce edema, maintain tissue oxygenation, stimulate fibroblast and collagen production and prevent lipid peroxidation [18].
In the current study, complete healing of the index ulcer was significantly faster in hyperbaric group 50% in comparison to 29% of those treated with conventional wound care only, after one year follow up. Our findings are in agreement with those reported in previous studies [11,19-22]. This could be attributed to that; HBO was found to increase the tensile strength in skin wounds and stimulate angiogenesis histologically [23,24]. The angiogenic properties induced by HBO are derived from the increase in oxygen tension that may persist for several hours after HBOT [13,25]. Also, it has been demonstrated that HBO can increase the tolerance of tissue to ischemia, diminish metabolic disturbances, improve tissue microcirculation, and reduce platelet aggregation. These characteristics, combined with the ability of plasma to carry dissolved oxygen to areas where red blood cells cannot reach, have been shown to have a beneficial effect on oxygenation of many hypoxic tissues [23,26]. Moreover, Aydin et al. [27] observed that with HBOT help to increase Insulin-like Growth Factor (IGF-1) levels, which promotes wound healing. A lack of IGF-1 expression within the basal layer and fibroblasts may contribute to retarded wound healing in diabetes mellitus patients [15]. Insulin and IGF-1 play important roles in vascular biology. Both hormones regulate vascular tone, in part by decreasing vasoconstrictor responses to agonists, such as angiotensin II, norepinephrine, and vasopressin [28].
Niinikoski [1] observed that, some microvascular parameters such as transcutaneous partial oxygen pressure (TcPO2) could be useful in predicting which patients will benefit from HBOT. He recommended that HBO should be added to conventional treatment if the TcPO2 close to the trophic lesion in 2.5 Atmospheric Absolute HBO is over 200 mm/Hg. But because these analyses are limited by their deficient primary clinical data, they should be interpreted with caution. In the current study TcPO2 was not used as a criterion for patient selection.
As regard major amputation, in our study, there were 2 major amputations in HBOT group versus 3 major amputations in group B of only conventional wound care. However in our study, there was insufficient power to analyze the rate of major amputation which were only performed due to life threatening infection, Also all the major amputation in our study, were Wagner grade IV ulcers. These results go in hand with Duzgun et al. [20] and Kalani et al. [21] who have shown the beneficial effect of HBOT in preventing amputations. Also Tiaka et al. [19] reported that HBO reduces amputation rates and increases the likelihood of healing in infected diabetic foot ulcers, resulting in better quality of life. Moreover, in a meta-analysis done by Liu et al. [29] revealed that, treatment with HBO improved the rate of healing, reduced the risk of major amputations in patients with diabetic foot ulcers and improve quality of life. On the other hand Margolis et al. [30] observed that HBO neither improved the likelihood that a wound would heal nor prevented amputation in diabetic foot ulcers.
In conclusion this study supports the role of HBOT as an adjuvant in healing of diabetic foot ulcers and improving quality of life. Several key issues remain to be addressed such as developing vigorous criteria to determine which patients are likely to benefit from the therapy.