Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2013) Volume 0, Issue 0
We report the results of hyperbaric oxygen therapy (HBO) for pancreatic and gastrointestinal disease. Thirty-nine patients received 100% oxygen at 2 atmospheres absolute pressure for 60 min. Results: In all four patients with liver abscess, feverishness subsided within 2.7 days after the start of HBO. All of three patients with infection after hepatic resection were relieved of systemic inflammatory response system (SIRS) and showed reduced CRP levels after HBO. In all of seven patients with acute appendicitis, pyrexia was relieved at 1.8 days after HBO introduction, and further surgery was not necessary. Among five patients with colorectal disease, HBO was effective in four, but ineffective in one. Five of six cases of infection after pancreatic resection were cured immediately after HBO. There were no complications such as middle ear inflammation, oxygen intoxication or pneumothorax. Conclusions: HBO is sometimes effective for treatment of refractory gastro enteric infections, especially those for which drainage is difficult. Pyrexia improved within 2.3 days after the start of HBO in most cases. If infection is refractory to standard antibiotics or drainage, HBO should be considered as an additional treatment. Since HBO is safe and generally cost-effective, it should be considered as an adjunct therapy for all gastro enteric infections.
<Keywords: Hyperbaric oxygen therapy, Pancreatitis, Abdominal infection, Pneumonia
In the field of abdominal surgery, hyperbaric oxygen therapy (HBO) is used mainly for adhesive ileus [1] and peumatosis intestinalis [2,3]. However, few reports have documented the use of HBO in other fields of gastroenterology. HBO has been shown to be especially effective for healing of complex ischemic wounds in patients with atherosclerosis or diabetes mellitus [4].
Recently HBO has also been used in cases of liver failure and liver transplantation [5]. HBO with 100% oxygen at twice sea level atmospheric pressure can create an arterial oxygen tension in excess of 2000 mmHg, and almost 400 mmHg in tissues [6]. Here we examined the utility of HBO for various gastroenteric diseases.
Thirty-nine patients with gastro enteric conditions that had proved refractory to conservative therapies such as antibiotics or drainage were treated with HBO between 2007 and 2012 in our department (Table 1). Patients were treated once a day in a hyperbaric chamber (BARA MED, Koike Medical, Tokyo, Japan) at a pressure of 2.0 atmospheres absolute and received 100% oxygen (Figure 1). Session duration was 60 min, and decompression was initiated at 15 min. Each patient provided written informed consent to undergo HBO.
Figure 1: Each session of HBO involved the use of 100% oxygen at 2 atmospheres absolute pressure for 60 minutes.
| Disease | Number of patients | Days required for pyrexia to subside | Mean of HBO sessions | Cases not effective to <38 degrees after HBO |
| Liver abscess | 4 | 2.7 | 15.3 | 0 |
| Abscess after hepatectomy | 3 | 2 | 11 | 0 |
| Acute appendicitis | 7 | 1.8 | 9.9 | 0 |
| Colorectal disease | 5 | 11.3 | 11.2 | 1 |
| Esophageal disease | 3 | 1 | 14.7 | 0 |
| Pancreatic disease | 7 | 1.6 | 12.3 | 1 |
| Ileus | 3 | no fever | 7.3 | 2 |
| Abdominal wall abscess | 1 | no fever | 28 | 0 |
| Subcutaneous phlegmon | 1 | 2 | 14 | 0 |
| Mesh infection | 1 | no fever | 14 | 0 |
| Pyogenic spondylitis | 1 | no fever | 26 | 0 |
| Pelvic abscess after resection of ileum | 1 | no fever | 14 | 1 |
| Abscess after gastric perforation | 1 | 3 | 10 | 1 |
| Acute obstructive suppurative cholangitis | 1 | 14 | ||
| Total | 39 | 14.4 |
Table 1: Thirty-nine patients with gastro enteric conditions that had proved refractory to conservative therapies.
The clinical parameters recorded for each patient included the period between onset of fever (more than 38 degree) and the start of HBO, body temperature at the time of HBO initiation, number of sessions (days) of HBO, period between the start of HBO and fever resolution (less than 38 degrees), white blood cell count, CRP levels before and after HBO, types of bacteria responsible for inflammation, and clinical outcome.
Liver abscess, and abscess after hepatectomy
HBO was performed for four cases of liver abscess. The mean number of sessions (days) of HBO was 15.3 (range 4 to 28), and the period between onset of fever and the start of HBO was 4 to 14 days. In all four cases the fever decreased to less than 38 degree within 1 to 4 days after the start of HBO (mean 2.7 days). The mean white blood cell count decreased from 11565 to 4415 micro little, and the mean CRP level from 15.0 to 0.4 mg/dl. The causative bacteria included Citrobacter, Enterococcus and Staphylococcus. All four cases were resolved without percutaneous transhepatic abscess drainage (Figures 2a-2d).
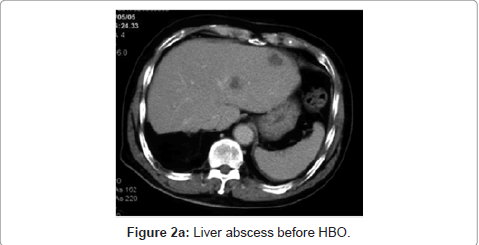
Figure 2a: Liver abscess before HBO.
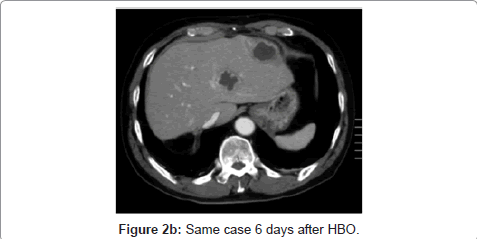
Figure 2b: Same case 6 days after HBO.
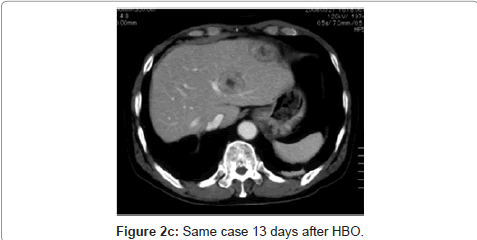
Figure 2c: Same case 13 days after HBO.
Figure 2d: Same case 21 days after HBO.
HBO was also performed for three post-hepatectomy patients, all of whom had undergone segmentectomy of S8. One of the three had MRSA infection and SIRS, but his condition improved 3 days after starting HBO. The other two patients with abscesses were also cured after 13 and 14 sessions of HBO, respectively.
Acute appendicitis
HBO was applied to 7 cases of acute appendicitis. Appendectomy was not performed for 2 of these cases because of severe extension of retroperitoneal abscess or phlegmon. The other cases involved postappendectomy abscesses. The mean number of HBO sessions was 9.9 (range 7 to 14). Pyrexia decreased to below 38 degrees 1.8 days (range 1 to 3 days) after initiation of HBO. The mean white blood cell count decreased from 13183 to 7185 micro little, and the CRP level from 13.7 to 0.7 mg/dl. All seven patients were discharged without further drainage surgery (Figures 3a and 3b).
Figure 3a: Intra-abdominal abscess due to appendicitis before HBO.
Figure 3b: Abscess was improved after 10 sessions of HBO (same case).
Colorectal disease
HBO was applied to five cases of colorectal disease comprising intraperitoneal abscess after endoscopic mucosal resection for sigmoid colon adenoma, pelvic abscess after sigmoidectomy for ischemic necrosis of the sigmoid colon due to anti-phospholipid antibody syndrome, retroperitoneal abscess after right hemicolectomy for ascending colon cancer, and two cases of ileo-cecal diverticulitis.
The mean number of HBO sessions was 11.2. Four of the patients were cured within 2 to 9 days after the initiation of HBO. However, HBO was not considered effective for the case of pelvic abscess after sigmoidectomy for ischemic necrosis of the sigmoid colon due to antiphospholipid antibody syndrome, because resolution of SIRS took longer days as 23 days.
Esophageal disease
HBO was employed for three cases of esophagieal disease. Two of them involved mediastinal abscess and peritoneal abscess after esophagectomy, and the other was esophago-tracheal fistula due to radiation for lung cancer. Pyrexia was resolved within one day after HBO in all three patients (Figures 4a and 4b). However, the esophagotracheal fistula was not cured.
Figure 4a: Mediastinal abscess after esophagectomy (before HBO).
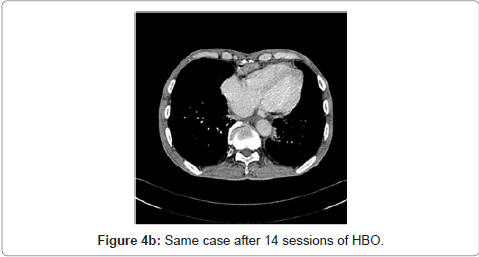
Figure 4b: Same case after 14 sessions of HBO.
Pancreatic disease
Pyrexia was resolved by HBO within 2 days in a patient with an infected pseudocyst due to alcoholic pancreatitis (Figures 5a and 5b).
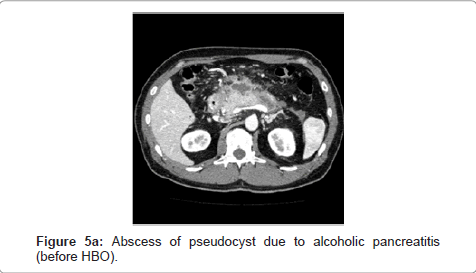
Figure 5a: Abscess of pseudocyst due to alcoholic pancreatitis (before HBO).
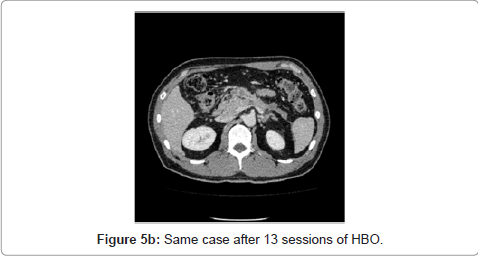
Figure 5b: Same case after 13 sessions of HBO.
HBO was also applied to three patients after pancreatoduodenectomy. In one of them, although CT showed absence of abscess formation in the abdominal cavity, pyrexia was refractory, requiring daily NSAIDs and antibiotic infusion after surgery. Three days after the introduction of HBO therapy, the fever was resolved (Figure 6).
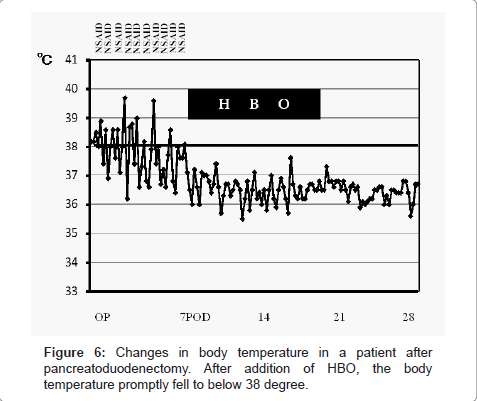
Figure 6: Changes in body temperature in a patient after pancreatoduodenectomy. After addition of HBO, the body temperature promptly fell to below 38 degree.
HBO was also used for three patients with intra abdominal abscess after distal pancreatectomy. Although the fever was resolved one day after HBO in two cases, the abscess was not cured, and re-operation was required in one case.
Ileus
Three cases of ileus were treated with HBO, being effective in one case and not effective in two. Paralytic ileus was cured within 5 days after HBO. An ileus tube was required in one case because HBO was not effective. Reoperation was performed for ileus after resection of transverse colon cancer.
Other diseases
HBO was very effective for treatment of abdominal wall infection, subcutaneous phlegmon around the drainage T-tube, and pyogenic spondylitis (Figure 7a) after cholecystectomy due to spontaneous gallbladder rupture (Figure 7b). However, HBO was not effective for pelvic abscess after resection of an irradiated small intestine or for abdominal abscess after gastric perforation. Reoperations were required in both cases.
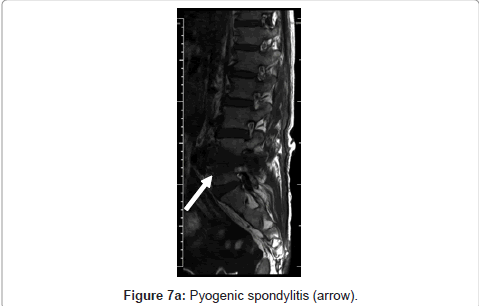
Figure 7a: Pyogenic spondylitis (arrow).
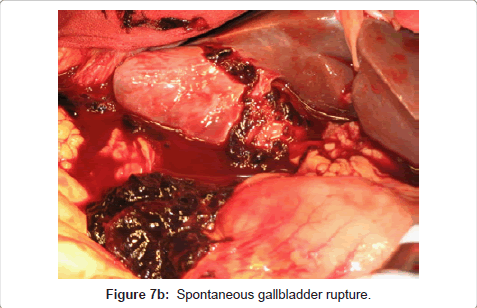
Figure 7b: Spontaneous gallbladder rupture.
There were no complications such as oxygen intoxication, inflammation of the middle ear, or pneumothorax in this series.
The use of HBO is reportedly beneficial for chronic non-healing diabetic wounds, compromised skin grafts, bone and soft tissue radiation necrosis, and gas gangrene [7,8]. HBO therapy has been reported for a patient with perinephritic abscess due to polycystic kidney disease [9]. Therefore, HBO may also have potential therapeutic benefits for gastroenteric conditions. HBO is reportedly effective for clearance of not only anaerobic but also aerobic bacteria [10].
HBO has been reported to ameliorate hepatic ischemia reperfusion injury in a rat model [11]. HBO also helps to enhance liver regeneration in living donor adult liver transplantation [12]. HBO after hepatectomy reduces the need for perioperative erythrocyte transfusion and also the incidence of postoperative complications, as well as affecting postoperative immunological responses [13]. HBO is reported to effectively prevent both bacterial overgrowth and translocation in rats with jaundice [14]. In the present study, we found that a combination of antibiotics and HBO was effective for management for intractable liver abscess.
There have been a number of reports of HBO for colorectal diseases. These have included its use for proctitis caused by irradiation of the pelvic area including the rectum and anus [15], and healing or clinical improvement of chronic radiation enteritis in two thirds of treated patients [16]. Supplementary systemic oxygen has been reported to decrease the rate of infection after colorectal surgery [4]. We consider that HBO is effective for management of diverticulitis or remnant peritoneal abscess, separate from the digestive tract, after colorectal surgery. On the other hand, we observed that HBO is not effective– without surgical intervention - for abscesses showing continuity with the digestive tract, resection and anastomosis of the perforation site, or colostomy, should be scheduled for such cases.
In the esophageal field, mediastinal gas gangrene due to esophageal perforation has been treated successfully with HBO [17]. In our experience, HBO is also useful for management of mediastinal abscess after esophagectomy. HBO has been used to treat radiation-induced hemorrhagic gastritis of the gastric conduit after esophagectomy [18]. In our present series, esophago-tracheal fistula was not cured by HBO. This is not because HBO failed but some illnesses are refractory to all man-made treatments simply due to the severity of the disease. One previous report has described that HBO was used successfully to treat a case of esophagotracheal fistula after ingestion of a lithium disc battery in 12-month-old child [19].
In the pancreatic field, the effectiveness of HBO has been examined mainly using a rat model [10]. HBO for management of severe acute pancreatitis is reportedly safe, and may have a role in improving treatment outcomes [20]. We also experienced a case of infected pseudocyst in a patient with alcoholic pancreatitis for which HBO proved effective, apparently ameliorating infection and local edema.
Recently the number of patients undergoing surgery for intraductal papillary mucinous neoplasm of the pancreas has been increasing [21,22]. In such cases, the pancreatic parenchyma is soft, and this makes pancreatic fistula after pancreatectomy a potentially lethal complication. The importance of drainage for pancreatic fistula after pancreatectomy has been reported [23]. It is indisputable that surgical or interventional drainage and antibiotics are essential for the treatment of gastroenteric infection. However, concurrent HBO seems to confer an additional anti-infection effect. In this series, a case of pyrexia after pancreatectomy was cured promptly by HBO, probably due to the bactericidal effect of high tissue oxygen pressure. High oxygen pressure also alleviates insufficiency of the peripheral circulation, allowing antibiotics to reach wider areas of tissue and providing oxygen to devitalized tissue.
HBO is reportedly effective for ileus. However, two of three such cases in our present series were not cured by HBO. An ileus tube or surgery may be more appropriate for treatment of mechanical ileus, whereas HBO may have better applicability for paralytic ileus.
HBO is usually used in combination with other treatments, such as antibiotics or drainage. Because randomized studies of HBO have been rare, there is insufficient evidence to indicate the optimal timing of therapy, or for establishing criteria that would allow selection of patients who would benefit from it [7].
In conclusion, HBO is effective for management of refractory infections in the gastroenteric field. HBO is especially effective for infections that are difficult to drain, such as retroperitonitis or phlegmon. In most of the present cases, pyrexia improved within 2.3 days after the start of HBO. HBO should be considered as an additional treatment for patients with infections that are refractory to standard antibiotics or drainage.