Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Short Communication - (2013) Volume 2, Issue 2
The External Branch of the Superior Laryngeal Nerve (EBSLN), which innervates the cricothyroid muscle, is important for voice quality. However, different identification rates for the nerve have been reported in thyroid surgery, with few surgeons not being able to identify the nerve at all. Different variants of the nerve have been described and various techniques have been used in order to identify the nerve. Our study aims to quote the identification rate of the EBSLN in thyroid surgery using standard dissection techniques. We feel that the definite prevalence of the Type III Friedman variant explains why the nerve may not be identified in a definite number of patients. The clinically relevant message of our study is that, even though it may not be possible to routinely identify the EBSLN in all cases of thyroid surgery, yet this nerve would be preserved by the standard extra capsular dissection techniques.
<Keywords: External branch of superior laryngeal nerve; Thyroidectomy; Inferior constrictor of pharynx; cricothyroid muscle
Though all surgeons routinely identify and preserve the Recurrent Laryngeal Nerve (RLN) using standard dissection techniques, this is not so for the External Branch of Superior Laryngeal Nerve (EBSLN). Different variants of the nerve have been described and various techniques have been described to identify it (see below).
The EBSLN supplies the cricothyroid muscle. This muscle increases the longitudinal tension of vocal folds and raises the pitch of voice [1]. The effects of the injury are subtle and include mild to moderate breathy voice, reduction in the average pitch of voice, especially the inability to raise the pitch of voice that leads to reduction of the voice range [2]. The severity would vary according to the voice demands of the individual and is undoubtedly important in professional voice users and singers. The nerve runs in close relation to the upper pole of the thyroid gland and is definitely at risk of injury during dissection [3]. Hence, the identification and preservation of the EBSLN should be a routine principle of thyroid surgery.
The famous opera singer Amelita Galli-Curci suffered damage to the EBSLN after thyroid surgery. This nerve has since become known as the “nerve of Galli-Curci.”
Various classification systems have been used to describe the course of the EBSLN. The Friedman classification system describes three anatomic variants of the nerve [4] which have been studied by cadaveric dissection [5]. The other classification systems for the EBSLN are the Cernea classification and the Kierner classification [6-8].
We have tried to evaluate the rate of identification of the EBSLN in 64 thyroidectomies performed over a two year period at a tertiary care hospital using standard thyroidectomy technique as described by Shah and Patel [9]. We feel the Friedman classification has a clinical implication describing the Type III variant which cannot be identified in routine thyroid surgery.
Sixty-four patients, aged 8-61 years, who underwent hemithyroidectomy at a tertiary care Hospital over a period of two years, were included in the study. They were all operated using extracapsular dissection technique described by Shah and Patel [9]. The identification rate of the Friedman variants of the EBSLN was calculated using standard dissection techniques.
The patients were clinically evaluated for any changes in voice related to injury to the EBSLN. Particularly, we evaluated hoarseness of voice, easy fatigability, and inability to produce high pitch voice, difficulty with high pitch, three days, one month and six months after the operation. Furthermore, patients underwent indirect laryngoscopy including videolaryngoscopy, and voice recording.
In 53 patients (83%) the EBSLN was identified and preserved. In 11 patients (17%) the nerve could not be identified at all.
Figure 1 shows intraoperative identification of the EBSLN. Pie diagram showing the percentage of the different Friedman variants identified is at Figure 2.
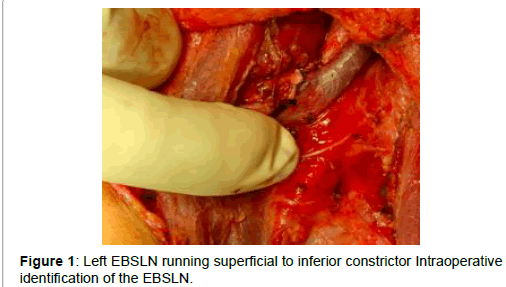
Figure 1: Left EBSLN running superficial to inferior constrictor Intraoperative identification of the EBSLN.
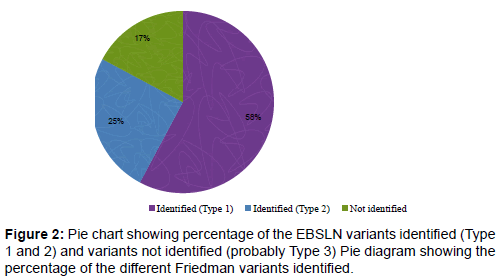
Figure 2: Pie chart showing percentage of the EBSLN variants identified (Type 1 and 2) and variants not identified (probably Type 3) Pie diagram showing the percentage of the different Friedman variants identified.
One patient had an iatrogenic RLN which was recognised intraoperatively and repaired. One patient had a transient RLN paresis, probably due to cautery injury, which recovered after one month.
In basic anatomy textbooks, the EBSLN is described as passing superficial to inferior constrictor muscle and piercing it to supply cricothyroid muscle [10,11]. Various landmarks have been described to identify the EBSLN in thyroid surgery. As described by Stell and Maran, the nerve lies in the Joll’s triangle [12]. The sternothyrolaryngeal triangle of Joll is formed laterally by the upper pole of the thyroid gland and the superior thyroid vessels, superiorly by the attachment of the strap muscles to the thyroid cartilage and medially by the midline. On its floor lies the cricothyroid muscle supplied by the EBSLN.
The EBSLN innervates the cricothyroid muscle which tenses the vocal cord. The voice symptoms associated with injury of the nerve are mild to moderate breathy voice, reduction in the average pitch of voice and a reduced voice range [1,2] with difficulties in high pitch and singing voice, which is very important in a professional voice user. However, more importance has always been given to the RLN in thyroid surgery and no uniform consensus exists regarding identification of the EBSLN.
Different identification rates of the EBSLN have been quoted by authors with few not performing routine identifications [13]. The techniques used for the identification of the EBSLN mentioned in literature include the use of nerve stimulator, the inspection of the distal part of the inferior constrictor muscle and individual ligation of the superior thyroid vessels [7,14-17] The principle of any surgery is the identification of any structure in order to preserve it. This applies to identification of the EBSLN as well. However the statement “The superior laryngeal nerve- I know where it should be and I avoid it, but I have never seen it,” is often quoted by surgeons.
This lack of uniformity regarding the surgical protocol for identification of the EBSLN is probably because it has a variable anatomical course. The course of this nerve has been described by many authors, and various classification systems have been described [6,8]. The EBSLN classification of the Cernea variants in Indian population has been studied [18-20].
The EBSLN classification system mentioned in literature by Cernea et al. [6] and Kierner et al. [8] are detailed at Tables 1 and 2.
| Cernea classification[6] | |
|---|---|
| Type 1 | Crosses STA > 1 cm above upper pole of thyroid |
| Type 2a | Crosses STA < 1 cm above upper pole of thyroid |
| Type 2b | Crosses STA under cover of upper pole of thyroid |
Table 1: The EBSLN classification system of Cernea et al.
| Kierner classification[8] | |
|---|---|
| Type 1 | Crosses STA > 1 cm above upper pole of thyroid |
| Type 2 | Crosses STA < 1 cm above upper pole of thyroid |
| Type 3 | Crosses STA under cover of upper pole of thyroid |
| Type 4 | Descends dorsal to artery and crosses STA branches immediately above upper pole of thyroid |
Table 2: The EBSLN classification system of Kierner et al.
Friedman has described three variants of the EBSLN as detailed below:
Type 1: The nerve runs superficial to the inferior constrictor muscle.
Type 2: The nerve penetrates the lower part of the inferior constrictor muscle.
Type 3: The nerve runs deep to the inferior constrictor muscle.
The Type 3 variant may account for the fact that many authors state that the nerve could not be identified in the region of the upper pole of the thyroid gland during thyroid surgery.
We feel the non identification rate of 17% in our study is also probably due to the prevalence of the Type III Friedman variant, which cannot be identified in routine thyroid surgery as it lies completely buried under the fibers of the inferior constrictor muscle of the pharynx.
Also, during the postoperative follow up the patients did not show any symptoms or signs of EBSLN injury, probably because this nerve was preserved by using the technique of the extracapsular dissection (which permitted to stay close to the thyroid gland), and by the individual ligation of branches of the superior laryngeal vessels, though they were not identified.
Figures 3-5 depict the three Friedman variants of the EBSLN.
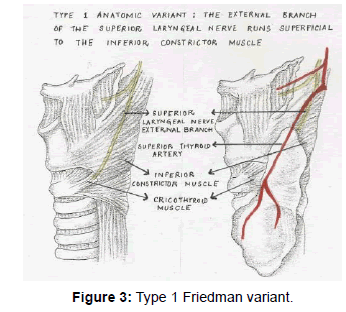
Figure 3: Type 1 Friedman variant.
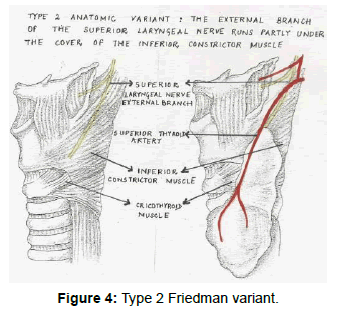
Figure 4: Type 2 Friedman variant.
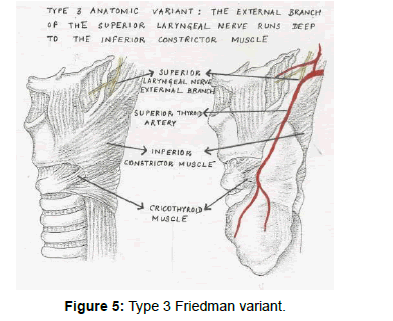
Figure 5: Type 3 Friedman variant.
The cardinal principal of surgery is identification of a structure in order to preserve it. This principal applies to thyroid surgery as well. Though all surgeons routinely identify and preserve the RLN using standard dissection techniques this is not so for the EBSLN. Different variants of the nerve have been described by various authors and various techniques have been described to identify it. We feel that this is probably due to the definite prevalence of the Type III Friedman variant of this nerve, which would not be encountered in the standard surgical field. Persistent searching for the nerve where a Type III Friedman variant is present would lead to frustration for the surgeon and unnecessary damage to surrounding structures. However, using a standard and meticulous technique of extracapsular dissection, the nerve would be preserved in all cases.