Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2015) Volume 0, Issue 0
Introduction: Pharmacists play an active role in community healthcare provision where they administer vaccines to their patients in accordance with state laws and regulations. Pharmacists contribute to disease prevention and the promotion of health. In Puerto Rico, pharmacists may administer vaccines against tetanus, diphtheria and pertussis, influenza, and pneumonia by protocol without a prescription. Background: By 2012, only 22% of the population aged 65 and older in Puerto Rico was vaccinated against pneumococcal vaccine. In the same year, 15% of the population between the ages of 18 and 64 years old were vaccinated. Poor promotion of the pneumococcal vaccine may be one of the barriers to a high vaccination rate. The purpose of the study was therefore to promote the uptake of pneumococcal vaccination among high-risk patients in a community pharmacy setting by implementing a pilot educational program capable of being expanded across multiple pharmacies in Puerto Rico. Methodology: This is a prospective, descriptive study in a single community pharmacy setting. The educational program promoting the pneumococcal vaccine was implemented over a 3-month timeframe. Inclusion criteria included: aged 21 years and older with at least one-pneumonia risk factors or aged 65 years and older. Some of the strategies of the educational program to promote the immunization utilizations rates were distribution of prescriptions flyers, telephonic outreach, educational programs, and promotional material within the pharmacy. Results: 259 patients were identified for the pneumonia educational program and 183 patients (70.6%) participated in the study. Twelve (12) weeks after implementing the educational program, 62 vaccines had been administered in 2015 vs. 13 vaccines administered during the same timeframe in 2014. Total number of pneumococcal vaccinations administered at the pharmacy as well as vaccination rate per total prescription volume were analyzed and compared utilizing descriptive statistics. Conclusion: Pharmacists are trained to administer vaccinations and implementation of an educational program in the community pharmacy setting can improve immunizations rates.
Keywords: Pneumococcal vaccine rates; Educational program; Immunization campaign; Pharmacists as immunizers
Pharmacists play an active role in community healthcare provision where they administer vaccines to their patients in accordance with state laws and regulations. Through vaccination programs, pharmacists contribute to disease prevention and the promotion of health. Pharmacists are also the most accessible healthcare professional in many communities and consistently reported one of the most trusted by patients [1]. In Puerto Rico, pharmacists may administer vaccines against tetanus, diphtheria and pertussis, influenza, and pneumococcal by protocol without a prescription.
Most susceptible to getting the pneumococcal infection are persons aged 65 years and older, and children under the age of 5 years old. One method of prevention is the administration of pneumococcal vaccination. There are two types of vaccines against pneumococcal disease: Pneumococcal Conjugate Vaccine 13 -valent (PCV13) and Pneumococcal Polysaccharide Vaccine 23 – valent (PPSV23). By 2012, only 22% of the population aged 65 and older in Puerto Rico was vaccinated with any pneumococcal vaccine compared with a nationwide rate of 69%. In the same year, only 15% of the population between the ages of 18 and 64 years old were vaccinated [2]. According to new Advisory Committee on Immunization Practices (ACIP) guidelines, “PCV13 and PPSV23 should be administered to all adults aged > 65 years. People who have not received pneumococcal vaccine or have an unknown immunization history should receive both PCV13 and PPSV23, allowing a period of 6-12 months between each vaccine [3]. If a patient is already vaccinated with either PPSV23 or PV13, they should receive the other vaccine after at least 1 year [4]. For adults aged 19-64 years, PPSV23 is recommended in adults with chronic heart disease, chronic lung disease, chronic liver disease, alcoholism, diabetes mellitus, who smoke cigarettes, or reside in Long Term Care Facility (LTCF).
Additionally, ACIP recommends use of PCV13 vaccine in adults 19 aged and older with immune-compromising conditions [5].
Poor promotion of the pneumococcal vaccine may be one of the barriers to a high vaccination rates. In an attempt to overcome this barrier, we implemented an educational intervention to increase the rates of pneumococcal vaccination and ultimately prevent the spread of pneumococcal infection in the Puerto Rican population. We hypothesized that implementing a community pharmacy-based educational program about pneumococcal vaccination will increase the uptake of this vaccine. The purpose of the study was therefore to promote the uptake of pneumococcal vaccination among high-risk patients in a community pharmacy setting by implementing a pilot educational program capable of being expanded across multiple pharmacies in Puerto Rico [6-8].
This was a prospective, descriptive study in a single community pharmacy setting. Institutional Review Board (IRB) already approved the protocol. The educational program promoting the pneumococcal vaccine was implemented during a 3-month (March to May, 2015) timeframe. All vaccine administration data was collected from Electronic Health System in aggregate without patient specific information. Per ACIP guidelines, the education program targeted all community pharmacy patients who were either (a) aged 65 years and older, or (b) aged 19 years and older with at least one immunecompromising condition or other risk factor for pneumococcal disease. The educational program was multifaceted.
The inclusion criteria for the research included (a) aged 21 years and older with at least one pneumococcal risk factor including smoker, cardiovascular diseases, asthma, or immune-compromising diseases (cancer, HIV), or (b) aged 65 years and older. Exclusion criteria for the research included (a) aged 20 years and younger (legal minors in Puerto Rico), (b) aged 21-64 years with no pneumonia risk factor, or (3) previously vaccinated against pneumococcal disease.
Collaborators in the educational program included a pharmacy resident, pharmacists, and pharmacy technicians.
The Strategies of the educational program implemented (Table 1) included educational flyers attached to prescriptions, weekly educational programs at the pharmacy, promotional materials within the pharmacy, and proactive telephonic outreach to pneumococcal vaccination candidates. Patients were identified for telephonic outreach in two ways. First, calls were made to patients that had previously been administered other vaccines at the pharmacy, but not yet received the pneumococcal vaccination through Vaccine Administration Record (VAR) documentation recorded. The candidates were identified in the pharmacy database using the inclusion criteria described above. Second, a flag alert appeared for all patients who met inclusion criteria when they came to the pharmacy to pick up a prescription. This flag triggered a pharmacist consultation for vaccine education. Primary endpoints for the study were total number of pneumococcal vaccinations administered at the pharmacy during the 12-week educational program. These endpoints were analyzed with descriptive statistics and compared with historical data as a control from the same timeframe in the previous year. Additionally, number of vaccine administrations per 1,000 prescriptions dispensed each week was also measured to control for potential changes in overall pharmacy prescription volume or pharmacy traffic between the historical control period and study period.
| Strategy | Description |
|---|---|
| Distribution of prescription flyers | Educational flyers were placed on all new and refill prescriptions dispensed at the pharmacy |
| Telephonic outreach | The pharmacy resident conducted calls to pharmacy customers who were candidates for pneumococcal vaccination as initial contact. |
| Educational Programs | The pharmacy resident conducted a weekly educational program at the pharmacy to promote the pneumococcal vaccine and provide education and guidance on the condition of pneumonia. |
| Promotional Materials within the pharmacy | Posters were placed in different areas of the pharmacy and brochures were made available to pharmacy customers about pneumococcal immunization. |
Strategies implemented
The table above describes the four strategies used for program promotion, ways of
patient outreach, and implementation of the project at the pharmacy.
Table 1: Strategies of the educational program implemented.
Patient details about the recruitment process during the implementation of the educational program are described in Table 2. 259 patients were identified for the pneumococcal vaccination educational program and 183 patients (70.6%) participated in the study. Of the patients who did not participate in the study, 7 refused participation, 59 did not answer calls from the pharmacy after three attempts, and 10 were previously vaccinated. Also of note, of the 183 patients that participated in the study, 51 had no insurance coverage for pneumococcal vaccination at the pharmacy.
| Quantity n (%) | |
|---|---|
| Total patients identified | 259 (100) |
| Participating in the program | 183 (70.6) |
| Refused participation | 7 (2.7) |
| Unable to reach | 59 (22.8) |
| Excluded based upon exclusion Criteria (previously vaccinated) |
10 (3.9) |
Patient recruitment
The table above represents the recruitment process during the implementation of the project based on the inclusion and exclusion criteria.
Table 2: Patients recruited for pneumonia educational program.
During the 3-month study period, 62 pneumococcal vaccines were administered at the community pharmacy compared to 13 vaccines administered in the same time period during the previous year (Figure 1). Interestingly, there was at least one vaccination administered each week of the study period while weeks 1, 2, 7, 8, 10, and 11 had no vaccine administrations during the historical control period./p>
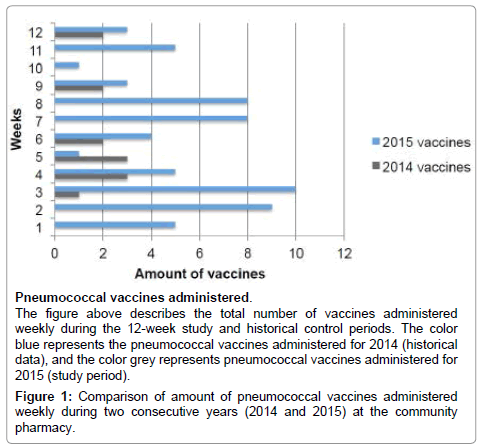
Figure 1: Comparison of amount of pneumococcal vaccines administered weekly during two consecutive years (2014 and 2015) at the community pharmacy.
Total vaccination rate per total prescription volume was also analyzed and compared to historical data. The overall pneumococcal vaccination rate (defined as number of vaccinations per 1,000 prescriptions) for the study period was 3.4, compared with 0.84 for the historical control period. Figure 2 shows the weekly pneumococcal vaccination rates during the study period and historical control period.
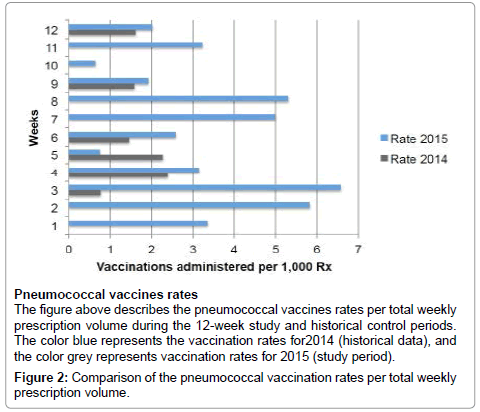
Figure 2: Comparison of the pneumococcal vaccination rates per total weekly prescription volume.
Historically, the pneumococcal vaccine was one of the less utilized vaccines at the research site. However, we found that following educational outreach by the pharmacist, many patients decided to come to the pharmacy to receive pneumococcal vaccination. The overall increase in total number of vaccinations and vaccination rate for the study period compared with the historical period was consistent for each individual week within the study period with the exception of week 5 (Figures 1 and 2). It is important to note that while normally there are 3 immunizing pharmacists working at the study site, during week 5 there was only
1 immunizing pharmacist available due to travel for a conference. This absence of immunizing pharmacists did not occur during the historical control period.
For a complete success in this type of project, we believe it is optimal to have a team that collaboratively educates, orients, and promotes the educational campaign. However, a major limitation of this study was the lack of collaboration from other pharmacy personnel, as their current daily responsibilities in the pharmacy did not allow for continued promotion of the project. Although there was a significant increase in pneumococcal vaccinations during the study period, we believe further benefit could result from more extensive collaboration between all pharmacy personnel in the educational program.
Another important consideration when interpreting these results is the type of clients at the pharmacy. The chain pharmacy used in the study has a population that is of a higher socioeconomic class with a high level of literacy. Additionally, many patients at this pharmacy are not accustomed to spending much time at the pharmacy receiving educational orientation or counseling. This lead to a challenge of receiving patient interest in or buy-in of the educational outreach program. Lastly, we observed a much higher than expected number of patients with insurance plans that did not contract with the pharmacy for pneumococcal immunizations.
We believe the strengths of the study to include a design that can be easily implemented in other community pharmacies, good external validity, and standardized patient education materials ensured all patients received the same educational outreach.
Despite several limitations, the study did identify a significant increase in pneumococcal vaccination rates each week, with the exception of week 5 described above. We believe this type of educational program can be used as a model in different pharmacies for health promotion and disease prevention in Puerto Rico. It is important that as health professionals, pharmacists continue improving clinical services, decrease healthcare costs, and improve the quality of care patients receive. Pneumococcal vaccinations have already been widely accepted as meeting both of these goals, and pharmacist-lead educational programs may play an important role in the improvement of vaccination rates in Puerto Rico.
Puerto Rico is facing major health disparities with regards to pneumococcal immunization rates. The active role of pharmacists in the community is essential to improve health education. Pharmacists are trained to administer vaccinations and capable of improving immunization rates. Implementing an educational program in a community setting can improve public health, patient education, and pharmacy revenue. In conclusion, the implementation of a community pharmacy based educational program about pneumococcal vaccination increased the utilization of this vaccine.
Advisor, Preceptors, and Director of Residency Community Pharmacy Program in the University of Puerto Rico, Medical Sciences Campus.
Preceptors, Corporate Department in IL, and Administrator of Walgreens, Inc.