Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2018) Volume 8, Issue 2
Pancreatitis is an inflammatory disorder of the pancreas, affecting its endocrine and exocrine function. It is mainly associated with abdominal pain, vomiting, nausea, indigestion, steatorrhea, weight loss and diabetes. There are many variants of pancreatitis that have been broadly divided into acute and chronic pancreatitis. In both the conditions, patients may suffer with recurring episodes of the aforesaid symptoms with progression of the disease. Pancreatitis is conservatively managed by emergency hospitalizations, lifelong pancreatic enzymes and supplements with modifications in diet and lifestyle. Advance surgical intervention is also being used in some cases to provide long term solution. However, the benefits of such procedures are limited to certain pockets of the world. Owing to unpredictable nature of the disease and limitations of treatment possibilities, pancreatitis adversely affects psychological, physical and financial status of the patients. In this scenario, many patients opt for alternate medicines. A North India based Ayurvedic clinic has earned reputation in bringing complete and sustainable relief in significant number of cases of Recurrent Acute/ Chronic Pancreatitis (RA/CP). A data on 319 well diagnosed cases demonstrates that Ayurvedic Treatment Protocol (ATP) has been able to bring complete relief in significant number of patients, without causing any side effect. Statistical analysis of the data shows that the treatment brought significant improvement in weight and reduction in frequency of attacks. ATP comprises of a few Ayurvedic formulations that are prescribed for a period of one year, along with regulated diet and lifestyle as well as complete physical and mental rest. The main Ayurvedic formulation used in the treatment is Amar. Experimental studies conducted using Amar have demonstrated its protective properties against pancreatitis. Further research is being conducted for the systematic and scientific development of this specialized ATP.
Keywords: Pancreatitis; Acute, Chronic; Ayurveda; Herbo Mineral Formulation; Rasa Shastra
Pancreatitis is an inflammation of the pancreas. It develops when enzymes secreted by the pancreas are unable to pass into the duodenum due to blockage within the pancreas. These active enzymes begin to digest pancreatic tissues, resulting in inflammation [1]. Broadly, Pancreatitis can be categorized into Acute and Chronic phase. Acute Pancreatitis (AP) is marked by inflammation in the pancreas and may be associated with recurrent episodes [2]. Chronic Pancreatitis (CP), on the other hand, is characterized by structural changes in the pancreas, visible in radiological images [3]. Pancreatitis is further classified into Recurrent Acute Pancreatitis, Acute on Chronic Pancreatitis, Chronic Calcific Pancreatitis, Necrotizing Pancreatitis, Groove Pancreatitis, Interstitial Pancreatitis, Hemorrhagic Pancreatitis and Familial pancreatitis [4,5]. Pancreatitis cannot be attributed to a uniform cause. However, TIGAR-O factors (T-Toxins, IIdiopathic, G-Genetic, A-Auto immune, R-Recurrent and OObstructive) are widely accepted for causing different forms of Pancreatitis [6].
All sorts of Pancreatitis are majorly associated with moderate to severe abdominal pain, nausea, vomiting, steatorrhea, weight loss. In some cases, gall stones, pseudocysts, ascitis, diabetes, multiple organ failures or cancer may also develop [7,8]. This is usually managed by emergency hospitalizations and lifelong enzymes with periodical monitoring. Asian and African continents have another variant of Pancreatitis, termed as Tropical Chronic Pancreatitis (TCP), which afflicts the young and is more prevalent among non-alcoholics. Protein malnutrition and mineral deficiency are major causative factors for TCP [9,10].
Pancreatitis is irreversible, progressive and fatal in nature and adversely affects the psychology of patients. Conventional medicines are found useful in tackling emergency situations, prolonging life span in majority of the cases. Yet, variable characteristics of the disease, especially sudden onset of symptoms and gradual progression, continue to infuse phobia among Pancreatitis patients. Hence, these patients always look for alternate solutions.
India is the only country where different systems of medicines like, Ayurveda, Unani, Siddha and Homeopathy, are officially recognized as independent systems of medicines in conjunction with conventional medicine [11]. As per the prevailing laws, a registered Ayurvedic practitioner can prepare his own medicines for use in his clinical practice, without obtaining any drug manufacturing licence [12]. In this scenario, a North India based Ayurvedic physician has reported significant and sustainable results in treating RA/CP patients [13-15]. The growing reputation of this centre attracts a fair number of Pancreatitis patients from various parts of India and abroad. In this paper, we report clinical data of enrolled patients, who completed one year of ATP (n=319/620).
Ayurveda is an ancient Indian system of medicine [16]. It has laid down its own principles to maintain the health of the healthy and treat the diseased. This system of medicine greatly emphasises on diet, lifestyle and medicines, prepared using substances of plant, animal and mineral origin. It also ascribes the effect of geographical location, weather and arrestation of basic urges on the health of an individual. Rasa Shastra is one of the eight clinical specialities of Ayurveda , which was developed in 6th BC. It deals with the therapeutics of processed metals and minerals, which are moderately to severely toxic in raw form. Such information is well described in ancient texts of Rasa Shastra [17,18]. Copper is highly toxic to human body in metallic form but also possesses anti-inflammatory properties [19,20]. Rasa is a synonym of Mercury. Rasa Shastra could be defined as the science of Mercury, which is the third most toxic metal [21]. This fact is very well accepted in Rasa Shastra . There are elaborate methodologies for processing Mercury. It is said that Mercury turns therapeutically potent by increasing the frequency of sublimation with Sulphur [18]. However, these statements have not been substantiated using in-vitro, in-vivo or experimental studies.
Pancreatitis is a deadly disease that adds substantial physical, emotional and financial burden to victims and their families. It is progressive in nature. Even a single attack of Acute Pancreatitis may turn into Chronic Pancreatitis in due course [22]. Chronic Pancreatitis may further lead to pancreatic cancer and uncontrolled diabetes in fair number of cases. Acute Pancreatitis may cause 4.8-13.5% mortality during hospitalisation. Out of these, 50% are attributed to multi-organ failures [23]. Chronic Pancreatitis brings 17%, 30% and 55% deaths in 5, 10 and 20 years respectively [24]. In recent years, use of Complementary and Alternative Medicine (CAM) has been widely accepted. A report by Grand View Research, Inc. projects the global CAM market to reach 196.87 Billion USD by 2025 [25]. CAM had traditionally been integral parts of people’s lives in India. With rising global interest and acceptance, their popularity is rapidly rising again. To strengthen and advance research in these areas, India has set up an independent central ministry of Ayurveda, Yoga, Unani, Siddh a and Homeopathy (AYUSH). The ministry and its different departments are headed by independent ministers and secretaries at both central and state level. At academic level, graduate, post graduate and doctorate courses in these systems are being taught in various parts of India. Besides, independent research councils and national institutes provide opportunities to carry research and extend services to people.
A total number of 620 patients volunteered for Ayurvedic treatment between January 1997 and September 2018. These patients were diagnosed with different forms of Pancreatitis, by leading medical doctors employed with hospitals of repute in the country, using modern diagnostic methods like Ultrasound, Magnetic Resonance Cholangiopancreatography, Endoscopic Retrograde Cholangiopancreatography, Computed Tomography scan and blood tests (Figure 1). Our clinical data indicates that more men (516) than women (104) were affected by the disease, a gender ratio of 5:1. Out of 620, 479 patients were of the reproductive age group (19-45 years), 63 were of the age group of 11-18 years, 58 patients more than 45 years old and 20 patients were less than 11 years of age. Data on geographical distribution shows that these patients came from all over the country. 77% patients were from North India, 19% from South India and 4% were NRIs. It was interesting to note that majority of the patients were non alcoholics (70.5%), non-tobacco users (80.3%), vegetarians (51.3%) with no family history (95.3%) [26]. Overall, these patients had an average history of RA/CP of 52.2 ± 48.2 months with a total of 5711 attacks and 3099 hospitalizations. A random analysis of expenses incurred in emergency hospitalisations, follow ups, investigations and indirect expenditures by the patients (n=413/620) showed that every patient spent an average of nearly INR six lacs thirty two thousand eight hundred and fifty four (Rs. 6,32,854; approx. 10,000 USD) on management of the disease before opting for ATP. Prior to Ayurvedic treatment, many patients were on pancreatic enzymes and had undergone stenting. The enrolled patients were asked to provide their old medical records for review and undergo fresh radiological (MRCP) and pathological tests (hemogram, liver function, kidney function, lipid profile, glycosylated haemoglobin, serum Vitamin D3 and B12) to ascertain the disease status.
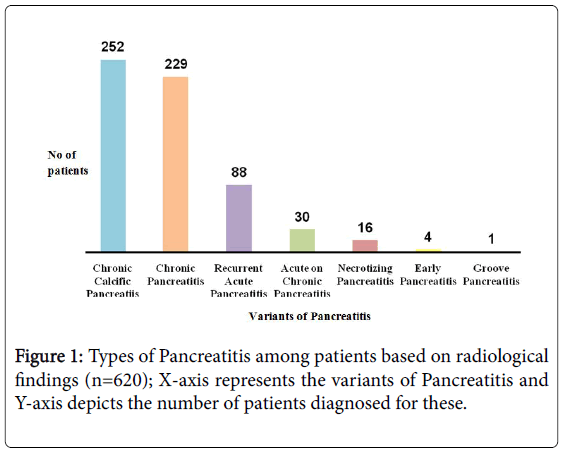
Figure 1: Types of Pancreatitis among patients based on radiological findings (n=620); X-axis represents the variants of Pancreatitis and Y-axis depicts the number of patients diagnosed for these.
After clinical evaluation, patients were admitted for three weeks for supervised indoor treatment at the centre. The treatment comprised of some herbo mineral formulations (Table 1) along with special focus on regulation of diet and lifestyle. Each patient was given a 1200 to 1600 calorie rich daily diet, divided into three meals and three snacks, and devoid of aerated drinks, caffeinated beverages, alcohol, onion, tomato, garlic, refined flour, packaged, precooked and reheated food. Daily intake of water for patients was decided based on their body weight (30 ml per kg body weight per day). Patients were advised to take complete mental and physical rest. At the onset of ATP, each patient was dewormed using Tablet Albendazole 400 mg [27]. The patients who had low levels of Vitamin D3 and Vitamin B12 were put on weekly dose of 60,000 IU Cholecalciferol mixed in 100 gm milk cream and a daily supplement of Methylcobalam in 1500 mcg with breakfast respectively [28,29]. With the start of the treatment, pancreatic enzymes were withdrawn in each patient. Patients suffering from diabetes and hypertension were permitted to continue anti diabetic and antihypertensive medicines in consultation with a physician.
| Name of Medicine | AMAR | RasonVati | Prak-20 | Narikel Lavan |
|---|---|---|---|---|
| Form | Capsule | Tablet | Powder/ Capsule | Powder |
| Dosage | 4 mg per kg body weight per day divided into three doses, given during meals | 1 gm, thrice a day after meals with water | 1 gm, thrice a day with meals | 1 gm, twice a day mixed in curd and water, on empty stomach |
| Number of patients | 620 | 466 | 593 | 305 |
Table 1: Details of herbo mineral formulations prescribed to patients (n=620).
After three weeks, the patients were discharged with one month’s medicines. As follow up, each patient was closely monitored over phone or mail on daily basis. For the entire year, refill batches of medicines were dispatched by courier against payment. At the end of the year, patients were called for revaluation-physical, pathological and radiological.
A total of three hundred nineteen patients have completed one year duration ATP (Table 2) and are leading normal and pain free life (Figure 2). Sixty-eight patients dropped due to various reasons (Table 3). Thirteen patients collected medicines but never consumed any dose and five patients were lost to follow up. Two patients reported disease progression and discontinued the treatment after seven months and eleven months respectively. There were total eight deaths during and after ATP; one patient died on twenty-fifth day of ATP due to the disease progression to advanced cancer of pancreas, another patient lived symptom free for four years after completing ATP and died in a conventional hospital after developing an abrupt acute attack of Pancreatitis, one patient died of hepatic failure caused due to infective hepatitis after one month of completion of ATP and another one died of obstructive jaundice induced hepatic failure after eleven months of ATP. Two patients, who presented with hyperbilirubinemia (Bilirubin>20 mg/dL) at the onset of ATP, died on day ninety and two hundred of ATP. Another patient, who had been suffering with Chronic Liver Disease for four months before starting ATP, died of hepatic failure after one month of starting ATP. One patient contracted a cardiac arrest after completing one-year of ATP.
| Reason | Number of patients |
|---|---|
| Total enrolments | 620 |
| Treatment complete | 319 |
| On treatment | 205 |
| Drop outs | 68 |
| Did not start treatment | 13 |
| Deaths | 8 |
| Lost to follow up | 5 |
| Progression of disease | 2 |
Table 2: Overall response of the treatment.
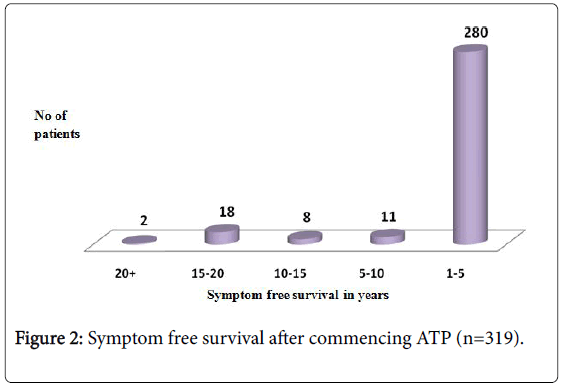
Figure 2: Symptom free survival after commencing ATP (n=319).
| Reason | Number of drop outs |
|---|---|
| No improvement | 48 |
| Poor compliance, treatment discontinued | 10 |
| Underwent surgery | 5 |
| Inadequate care | 3 |
| Complications due to Bariatric surgery, had to discontinue | 1 |
| Financial issues | 1 |
Table 3: Reasons for drop outs (n=68).
Impact evaluation (n=319)
There was marked improvement in the clinical condition in those patients who could complete one-year long ATP. Significant reduction was seen in number of emergency attacks and hospitalizations. Of 319 patients who completed ATP, 212 (66.5%) had suffered weight loss before ATP. The number dropped to 30 (9.4%) after the treatment. Also, only 4 (1.3%) patients had gained weight in the previous year of ATP, while taking pancreatic enzymes, but 140 (44%) patients gained weight during the one year of ATP (Figure 3). This effect was seen in spite of total withdrawal of pancreatic enzymes after the commencement of ATP. No adverse effect was reported by any patient. A random comparative analysis of pre and post ATP radiological images showed that there was no progression of the disease in these cases (n=133/319).
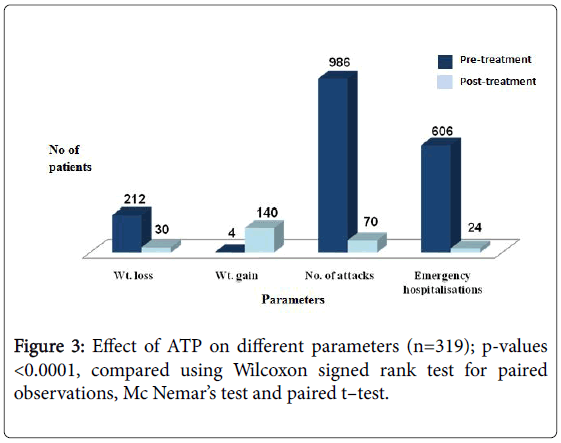
Figure 3: Effect of ATP on different parameters (n=319); p-values <0.0001, compared using Wilcoxon signed rank test for paired observations, Mc Nemar’s test and paired t–test.
Pancreatitis is an inflammatory process of the pancreas with variable characteristics. It causes irreversible damage to the organ and is progressive in nature, often leading to mortality in fair number of cases. The onset and periodical exacerbations of symptoms are managed conservatively by emergency hospitalisations, lifelong enzymes, surgical intervention and pancreatic replacement [8]. However, these measures have their own limitations and fail to eliminate psychological fear from the minds of the patients.
In this scenario, a North India-based Ayurvedic Centre has developed a treatment protocol which shows promising results in the management of the disease. From the clinical data generated by the Centre, in total six hundred twenty patients enrolled themselves between January 1997 to September 2018. These patients were treated using a standard ATP, comprising of Amar, Rason Vati, Prak 20 and Narikel Lavan along with a balanced diet composed of protein, carbohydrate/starch, fruits, vegetables and fat. We report clinical results of 319 beneficiaries of Ayurvedic treatment offered at the Centre, this far. All patients responded well to a year-long ATP. Besides, improving the general health condition of the patients, significant clinical results were noted. For example, after completing the treatment, frequency of pancreatic attacks and emergency hospitalization reduced significantly. The patients also gained healthy weight, which otherwise dwindles in this diseased condition, one of the many symptoms of pancreatitis. ATP was hence, well tolerated by all patients with no reported side-effects.
The abovementioned ATP is derived from Rasa Shastra, one of the eight clinical specialities of Ayurveda, which deals with substances of mineral, animal and plant origin, that are moderately to highly toxic in their raw forms [17]. There is enough literature on how to detoxify these toxic substances to products of therapeutic value. However, these procedures that are classically followed and practiced lack scientific validation.
Ayurvedic formulations used in the treatment are well described in classical texts and have been in use for ages for different ailments depending upon the perception of the treating physician, with the exception of Prak-20 and Amar, which fall under the category of patent and proprietary medicines. Amar, a herbo-mineral formulation (HMF) (PCT Application No. 3373/DEL/2014 dated 20.11.2014, Patent Office, Delhi, India), the main HMF used in the treatment of Pancreatitis, is prepared using Copper, Mercury and Sulphur with extracts of Luffa echinata and Clitorea ternatea together with lemon juice. It takes about three years of continuous processing to convert toxic Copper, Sulphur and Mercury into medicinal mineral form (Figure 4).
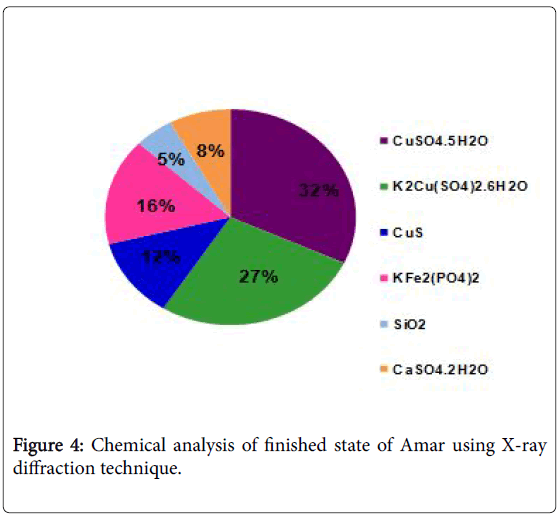
Figure 4: Chemical analysis of finished state of Amar using X-ray diffraction technique.
Prak-20 is modified and standardized form of a classical medicine and has proven hepato-protective properties [30]. Rason Vati is used to improve digestion, bloating and anorexia [31]. Narikel Lavan is used to treat colic pain and inflammation of the Gall Bladder [31]. No reported toxicity was observed in patients, which indicates that minerals present in Ayurvedic formulations coupled with regulated diet and lifestyle might play a crucial role in arresting disease progression and improving the quality of life of patients. This treatment was incidentally developed in mid 70s [32]. The prima facie evidences created over twenty one years of clinical practice suggest that further research be carried for the scientific development of this protocol.
We are thankful to the patients and their families for participating in the program. Our special thanks to Gopa Indu, Devendu Prakash, Gaurav Chaudhary for assisting in the preparation of Ayurvedic formulations. We also acknowledge the contribution of Mahima Verma, Karuna Swaroop and Preeti Sharma in data generation and manuscript writing.