Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2015) Volume 0, Issue 0
Introduction: Patients living in central rural towns in Puerto Rico comprise one of the most critical at-risk populations of limited health literacy due to the higher incidence of poverty and lower educational levels within this sector. The objective of this study was to assess the effect of clinical pharmacist intervention on medication adherence and disease knowledge among patients with low health literacy from the municipalities of Adjuntas and Lares in Puerto Rico. Methods: This study used a prospective analysis of patients referred for a pharmacist educational intervention in two rural outpatient clinics of Puerto Rico. Thirteen patients with inadequate glycemic control (A1C ≥ 9%), uncontrolled hypertension (≥ 150/90) or medication non-adherence (PDC < 0.80) were referred to the study by a primary care physician. Initial health literacy was measured by the Spanish Short Test of Functional Health Literacy in Adults (S-TOFHLA). The primary outcome of the study was average change of medication adherence assessed by calculating the proportion days covered (PDC) at baseline and at the end of the study period. The secondary outcome of the study was average change in patient’s disease-related knowledge using the Diabetes, Hypertension and Hyperlipidemia (DHL) knowledge instrument measured at baseline and at the end of the study period. The average change on hemoglobin A1C and blood pressure was also calculated between baseline and post-intervention evaluation. Results: The study showed a significant improvement in disease-related knowledge and modest improvements in disease clinical markers and medication adherence. Adherence improved from an average PDC of 0.59 to a PDC of 0.64. Disease related knowledge improved from an average 58% to an 83% in questionnaire scores. Conclusion: Due to small patient recruitment and the lack of statistically significant data in this study, further research with a larger patient population is required to accurately identify the potential benefits of these interventions.
Keywords: Health literacy; Community pharmacy; Medication adherence; Pharmaceutical care; Proportion days covered (PDC); Spanish short test of functional health literacy in adults (S-TOFHLA); Ambulatory care
Health literacy has been defined by the Centers for Disease Control and Prevention as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” [1]. According to the United Nations Educational, Scientific and Cultural Organization Institute of Statistics an estimated 16% of the world’s adult population lack basic literacy skills [2]. Limited health literacy is associated with poor adherence, inadequate control of chronic conditions, and increased healthcare costs. Studies have demonstrated a higher rate of hospitalization and use of emergency services among patients with limited literacy skills [3]. Persons with limited health literacy skills are more likely to have chronic conditions and are less able to manage them effectively. Studies have found that patients with high blood pressure [4], diabetes [4-6], asthma [7], or HIV/AIDS [8] who have limited health literacy skills have less knowledge of their illness and its management.
The 2010 U.S. Census Bureau in Puerto Rico reported that literacy rate was 92%. Although Census data seems to reflect adequate levels of literacy for Puerto Rican people, the data does not provide an accurate portrait of the functional health literacy in the island [9].
Certain demographic subgroups are at greater risk of having low health literacy, including people with chronic disease, lower educational attainment, elderly, underserved minority groups and immigrants. Patients living in central rural towns in Puerto Rico comprise one of the most at-risk populations of limited health literacy due to the higher incidence of poverty and lower educational levels within this area. Adjuntas is the municipality in Puerto Rico with the highest level of poverty (79%) and illiteracy rate (30.0%). Additionally, Adjuntas is the third municipality with the highest rate of unemployment. Hence, the unemployment rate is 23.3% in Adjuntas and 17.9% in Lares [10].
Recent evidence suggests that diabetes education improves selfmanagement and glycemic control in those with limited health literacy [11]. Despite increasing concern about the impact of low health literacy on diabetes care, hypertension, and medication adherence, there are no proven interventions available for this population in Puerto Rico that address low health literacy.
The objective of this study was to assess the effect of clinical pharmacist intervention on medication adherence and disease related knowledge among patients with low health literacy from the municipalities of Adjuntas and Lares in Puerto Rico.
This study used a prospective analysis of patients referred for a pharmacist educational intervention in 2 rural outpatient clinics of Puerto Rico. The two outpatient clinics selected for patient recruitment were Policlínica Castañer in Adjuntas and Hospital Castañer in Lares. Subjects were identified and referred to the study by a primary care physician. Inclusion criteria included: age 21 years or older; documentation of at least one of the following: hemoglobin A1C ≥ 9%, systolic blood pressure ≥ 150, diastolic blood pressure ≥ 90, and medication non-adherence (PDC <0.8). Exclusion criteria included persons younger than 21 years of age, pregnant women, and patients with both blood pressure and hemoglobin A1C at goal.
Of the thirteen patients referred to the study by physicians, all participated in an initial encounter which consisted in an individualized clinic visit. During the visit, the Spanish version of the Short Test of Functional Health Literacy in Adults (S-TOFHLA) instrument was used to measure the functional health literacy. S-TOFHLA is a validated tool that only uses questions from two reading comprehension passages of the full test and is commonly utilized when evaluation of health literacy is needed for research purposes. There are 36 items that are administered in 7 minutes. The scoring categorizes respondents into inadequate (0-16), marginal (17-22) or adequate levels (23-36) of health literacy [12].
During the first encounter, a diabetes and/or hypertensionknowledge questionnaire was also administered to measure baseline knowledge of both diseases. The Diabetes, Hypertension and Hyperlipidemia (DHL) [13] knowledge instrument was used to measure diabetes and hypertension knowledge. The DHL is a validated instrument used for assessing the knowledge of patients with type 2 diabetes in the Malaysian population. The instrument was translated to the Spanish language and only the diabetes and hypertension sections were used for the purposes of the study. The questionnaire consisted of a total of fourteen questions: seven questions on diabetes and seven questions on hypertension. The answers for each question in the knowledge questionnaire was scored as true, false or don’t know. Analyses was performed by scoring 1 for a correct response and 0 for an incorrect or don’t know response. The total score was converted into percentage, ranging from 0 to 100 percent. Zero indicated the lowest level of knowledge, while 100 indicated the highest level.
Blood pressure, heart rate, weight, height, body mass index, and highest level of education were also assessed for all patients at the first clinic visit. Baseline haemoglobin A1C laboratory value was assessed from the medical records of both clinics.
The pharmacist intervention consisted of disease education, medication counselling, and instruction on the importance of adherence and self-monitoring with oral, written and visual information. Each prescription bottle was labeled with illustrative colors representing the directions and frequency of the administration of the medication. Educational content covered an introduction to diabetes and/or hypertension, blood glucose and/or blood pressure management, oral medications and insulin, nutrition and physical activity, and the prevention of complications (including eye, foot, cardiovascular, and kidney diseases). Illustrative medication schedules and blood pressure and glucose diaries were provided to each patient.
Follow-up consisted of bi-weekly telephone calls for the first month, followed by phone contact every four weeks through the study period. In total, three follow-up appointments were conducted. At each follow-up, education on medication adherence and healthy lifestyle changes was encouraged.
The primary outcome of the study was change of medication adherence measured at baseline and at the end of the study period. Adherence was assessed by calculating the proportion days covered (PDC) [14] for all medications filled. For this study, adherence was defined as a PDC of 0.8 or greater, and non-adherence was defined as a PDC of less than 0.8. The secondary outcome of the study was change in patient’s disease-state knowledge using the DHL knowledge instrument measured at baseline and at the end of the study period.
Comparison of change in hemoglobin A1C and blood pressure at baseline and the end of the study period was also evaluated. Data was obtained from the patient’s medical record at the hospital by assessing clinic data performed during the normal course of their care.
Differences between baseline and end of study data was analyzed with descriptive statistics. The Microsoft® Excel program was used to determine and describe the socio-demographic variables and mathematical findings.
The study was approved by the University of Puerto Rico Medical Science Campus IRB committee. A Spanish informed consent sheet was submitted to the IRB. All patients did consent their approval in participating in the study.
Out of twenty-four patient referrals, six did not meet the inclusion criteria and five were unable to be reached. Three patients had initial evaluation at their home since they were not able to come to the clinic due to transportation limitations. Table 1 demonstrates the baseline characteristics of the population that were included in the study. The final sample size was thirteen patients; six male patients (46%), seven female patients (54%) and twelve illiterate patients as defined by the S-TOFHLA (92%). In terms of location, four patients were from Policlinica Castañer in Adjuntas (39%) and eight were from Hospital General Castañer in Lares (61%).
| Characteristic | Mean | Range |
|---|---|---|
| Age (years) | 66 | 46-78 |
| BMI (kg/m2)* | 32.1 | 21.4-41.8 |
| Scholarity (grade) | 4 | 0-35 |
| S-TOFHLA* | 7 | 1-12 |
| A1C (%)* | 9.7 | 6-15.7 |
| Systolic Blood Pressure (mmHg) | 158 | 111-194 |
| Diastolic Blood Pressure (mmHg) | 79 | 60-103 |
| Score of DM* Knowledge Questionnaire (%) | 57 | 30-71 |
| Score of HTN* Knowledge Questionnaire (%) | 58 | 43-71 |
| Total Correct Questions of DM* Knowledge Questionnaire | 4 | 2-5 |
| Total Correct Questions of HTN* Knowledge Questionnaire | 4 | 3-5 |
| PDC* | 0.59 | 0.31-0.76 |
*BMI (Body Mass Index), S-TOFHLA (Spanish version of the Test of Functional Health Literacy in Adults (S-TOFHLA), A1C (Hemoglobin A1C), DM (Diabetes Mellitus), HTN (Hypertension), PDC (Proportion Days Covered)
Table 1: Population baseline characteristics.
Table 2 provides the baseline summary data of each patient by age, gender, and site, highest level of education, S-TOFHLA score, hemoglobin A1C, blood pressure, questionnaire scores and PDC. Twelve patients (92%) demonstrated inadequate level of health literacy and one showed adequate level of health literacy (8%). Eight patients had a hemoglobin A1C ≥ 9% (62%), eleven had a systolic blood pressure ≥ 150 (85%), one had a diastolic blood pressure ≥ 90 (8%) and all had a PDC < 0.80.
| Patient | Age | Gender* | Site* | Highest Education Achieved (Grade) | S-TOFHLA* | A1C* (%) | Systolic BP* | Diastolic BP* | DMQ* (%) | HTNQ* (%) | PDC* |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 68 | F | P | 4 | 6 | 12.7 | 187 | 77 | 30 | 71 | 0.65 |
| 2 | 46 | F | C | 12 | 35 | 12.5 | 125 | 81 | 71 | 57 | 0.76 |
| 3 | 55 | F | P | 1 | 2 | 7.2 | 159 | 60 | 57 | 71 | 0.31 |
| 4 | 63 | M | C | 3 | 3 | 8 | 167 | 103 | 71 | 57 | 0.80 |
| 5 | 72 | F | C | 1 | 6 | 6.3 | 155 | 82 | 43 | 57 | 0.57 |
| 6 | 78 | M | C | 7 | 0 | 9.7 | 194 | 86 | 71 | 71 | 0.63 |
| 7 | 69 | M | C | 2 | 6 | 9.1 | 155 | 77 | 57 | 57 | 0.75 |
| 8 | 57 | F | P | 7 | 5 | 15.7 | 145 | 84 | 71 | 71 | 0.39 |
| 9 | 67 | M | C | 3 | 4 | 10.1 | 111 | 63 | 57 | 43 | 0.70 |
| 10 | 70 | F | C | 1 | 2 | 6 | 158 | 72 | 43 | 57 | 0.47 |
| 11 | 70 | M | C | 3 | 4 | 11.4 | 160 | 76 | 57 | 57 | 0.60 |
| 12 | 74 | M | C | 2 | 9 | 8.5 | 180 | 74 | 43 | 43 | 0.49 |
| 13 | 75 | F | P | 6 | 4 | 9.4 | 152 | 77 | 71 | 43 | 0.65 |
*F (Female), M (Male), P (Policlinica Castañer in Adjuntas), C (Hospital General Castañer in Lares), S-TOFHLA (Spanish version of the Test of Functional Health Literacy in Adults (TOFHLA), A1C (Hemoglobin A1C), Systolic BP (Systolic Blood Pressure), Diastolic BP (Diastolic Blood Pressure), DMQ (Diabetes Mellitus Knowledge Questionnaire Score), HTNQ (Hypertension Knowledge Questionnaire Score), PDC (Proportion Days Covered)
Table 2: Summary of patient’s baseline data.
Table 3 provides the post-intervention summary data of each patient by haemoglobin A1C, blood pressure, questionnaire scores and PDC. Four patients had a haemoglobin A1C ≥ 9% (23%), six had a systolic blood pressure ≥ 150 (46%), one had a diastolic blood pressure ≥ 90 (8%) and all had a PDC < 0.80. Three patients did not provide final haemoglobin A1C data and one did not provide final blood pressure data measurements.
| Patient | A1C* (%) | Systolic BP* | Diastolic BP* | DMQ* (%) | HTNQ* (%) | PDC* |
|---|---|---|---|---|---|---|
| 1 | 11.8 | 169 | 70 | 86 | 86 | 0.71 |
| 2 | N/A | 139 | 89 | 100 | 100 | 0.78 |
| 3 | 6.7 | 155 | 84 | 71 | 86 | 0.50 |
| 4 | 8 | 176 | 82 | 71 | 57 | 0.71 |
| 5 | 6.3 | 148 | 85 | 71 | 86 | 0.51 |
| 6 | 7.5 | 173 | 78 | 86 | 86 | 0.75 |
| 7 | 11.3 | 156 | 93 | 100 | 100 | 0.64 |
| 8 | N/A | 142 | 44 | 100 | 86 | 0.38 |
| 9 | N/A | 138 | 78 | 86 | 86 | 0.74 |
| 10 | 6.2 | 147 | 82 | 86 | 100 | 0.60 |
| 11 | 10.6 | 152 | 56 | 71 | 57 | 0.72 |
| 12 | 8.5 | N/A | N/A | 71 | 86 | 0.60 |
| 13 | 10.2 | 148 | 81 | 71 | 71 | 0.79 |
*A1C (Hemoglobin A1C), Systolic BP (Systolic Blood Pressure), Diastolic BP (Diastolic Blood Pressure), DMQ (Diabetes Mellitus Knowledge Questionnaire Score), HTNQ (Hypertension Knowledge Questionnaire Score), PDC (Proportion Days Covered)
Table 3: Summary of population post-intervention data.
The average change of PDC, questionnaire scores and clinical markers of the each disease was calculated between baseline and post-intervention evaluation. The following changes in average baseline values were observed: an increase of 8.5% in PDC, a 43.9% increase in diabetes knowledge questionnaire score, a 44.8% increase in hypertension knowledge questionnaire score, a decrease of 0.6% in haemoglobin A1C, a 1.9% decrease of systolic blood pressure and a 2.5% decrease of diastolic blood pressure. Figures 1-5 depict the average changes observed in the variables measured.
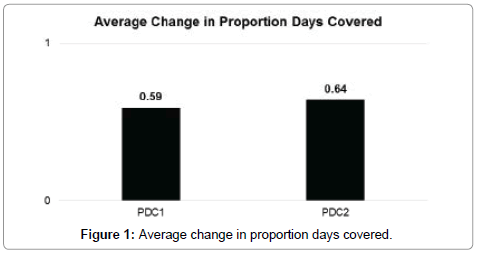
Figure 1: Average change in proportion days covered.
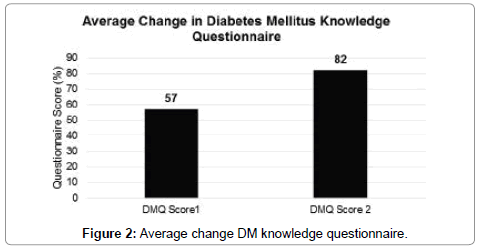
Figure 2: Average change DM knowledge questionnaire.
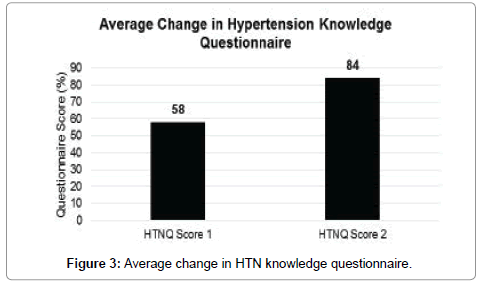
Figure 3: Average change in HTN knowledge questionnaire.
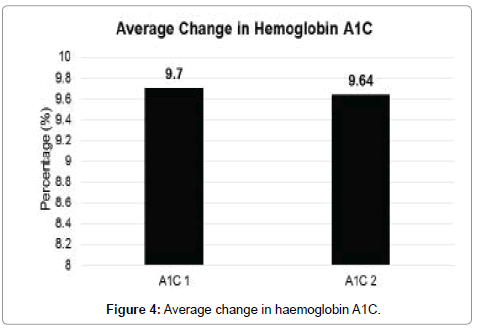
Figure 4: Average change in haemoglobin A1C.
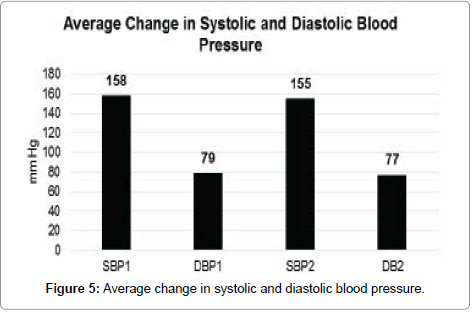
Figure 5: Average change in systolic and diastolic blood pressure.
Our study showed an increase in medication adherence represented by an increase of the PDC value. However, the desired level for adherence (PDC > 0.80) was not reached in all patients. An increase in disease knowledge was also observed in the study due to an increase in both diabetes and hypertension knowledge questionnaire scores. Nevertheless, the DHL knowledge questionnaire instrument has only been validated in the English language and in Malaysia. These could represent a limitation of the study since the instrument has not been previously validated in a Puerto Rican or Spanish population.
Study findings also showed a slight decrease in haemoglobin A1C and blood pressure at the end of the study. However, follow-up data was not available for all patients. Additionally, the study evaluated pharmaceutical care during two months of intervention. A greater impact on clinical markers may require a longer study period.
Transportation issues in most patients were a limitation of the study. Hence, follow-up was achieved by telephonic encounters. Future research that integrates transportation incentives or other proactive means for arranging reliable transportation for patients might address this.
Our research study is consistent with other studies that demonstrate that pharmaceutical care intervention can improve disease-related knowledge, clinical markers, and medication adherence in patients with hypertension and/or diabetes [15-17]. Future research with a larger sample size and a longer duration of time may determine if the effect of pharmacist management on disease-related knowledge, haemoglobin A1C, blood pressure and medication adherence is sustainable after study completion. Likewise, it could provide better analysis of pharmaceutical care services in Puerto Rico and their effect on patient outcomes among patients with low health literacy [18-22].
Addressing health literacy is a critical part of providing highquality healthcare. Medication counselling during the dispensing process is often the last opportunity for pharmacists to ensure that patients understand how to use their medications appropriately and identify adherence issues and medication related problems. Hence, pharmacists can support and expand local efforts to help identify patients at risk of low health literacy and develop educational programs in the community to improve medication use and chronic disease understanding among these patients.
Our study showed a significant improvement in disease-related knowledge and modest improvements in disease clinical markers and medication adherence among patients with low health literacy receiving pharmacist educational interventions in areas of Castañer, Lares and Adjuntas, Puerto Rico. Due to small patient recruitment and the lack of statistically significant data in this study, further research with a larger patient population is required to accurately identify the potential benefits of these interventions.