Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2015) Volume 3, Issue 3
Objective: To assess the effect of GnRHa as luteal phase support in women undergoing controlled ovarian stimulation and IUI.
Design: A prospective, randomized trial.
Setting: Cytogenetic and Endoscopy Unit, Zagazig University Hospital.
Methods: Two hundred fourteen women either with unexplained or mild male factor infertility was planned to contribute to this study. After exclusion 18 women, 196 couples were assigned into two groups: GnRHa (study group, n = 98) were receiving Single dose of 0.1 mg of Triptorelin by SC injection 8 days after the insemination while non GnRHa (the control group, n = 98) were not receiving injection as luteal phase support.
Results: Serum progesterone levels at 10 days after IUI was statistically significantly increased in the GnRHa group than in non GnRHa group (p < 0.001), while, there were no significant differences between both groups in serum Progesterone level before triggering and 7 days after insemination. Pregnancy rates per cycle were (18.94% for GnRHa and 17.39% for non GnRHa group respectively (P = 0.78).
Conclusions: Luteal phase GnRHa administration can increase the progesterone level and consequently the luteal phase duration, with increase in the pregnancy rate in the GnRHa group but did not reaching the statistically significance level.
<Keywords: GnRH agonist; Luteal phase support; IUI; Pregnancy rate
Corpus luteum produces progesterone (P) in response to human chorionic gonadotropin (hCG) and luteinizing hormone (LH) [1]. Progesterone not only supports endometrial development but also potentially maintains the embryo survival by changing the immune system toward production of non-inflammatory T-helper (Th2) cytokines [2]. Luteal phase deficiency is a common feature of cycles resulting from follicular stimulation either with hMG alone or downregulated with a GnRHa and stimulated with hMG [3]. In stimulated IUI cycles, the existence of LPD is still controversial [4,5].
Multifollicular development and supra-physiologic steroid concentration may negatively affect LH secretion through a longloop mechanism. Disturbed LH secretion may induce LPD with premature luteolysis, low progesterone level and a shortened luteal phase [6,7]. Additionally, controlled ovarian stimulation (COS) may accelerate endometrial maturation and impeding receptivity to embryo implantation [8]. Therefore luteal phase support is a common practice in infertility treatment to improve embryo implantation and clinical pregnancy rates.
Different forms and doses of three therapeutic agents; hCG, progesterone and oral estradiol (E2) were suggested as different options for the luteal-phase support [3]. However, some data have suggested that there is a beneficial effect of GnRHa in the luteal phase on ART outcomes [9,10]. GnRHa could offer several advantages over existing options: (i) Available nasal self-administration, compared to hCG injections or multiple daily vaginal progesterone; (ii) The chance for early diagnosis of pregnancy [10]. Therefore, the effects of GnRHa administration in the luteal phase have been the focus of different studies. Fauser et al. [11] illustrated that endogenous FSH and LH surge induced by GnRHa is a physiological event with luteal phase steroid concentration near to those of normal cycles. GnRHa receptors have been described in the corpus luteum (CL) and human endometrium. So, Tesarik et al. [9] reported that injection of a single dose of GnRHa in the luteal phase was shown to increase pregnancy, implantation and birth rates in recipients of donated oocytes suggesting a possible direct effect of GnRHa on the embryo. The supposed mechanism of beneficial effect of GnRHa in LPD is not clear. It was suggested that GnRHa can preserve of the corpus luteum, directly affect the endometrium and the embryo or by combination of these possibilities. Conversely, other authors did not prove positive action from the injection of GnRHa in the luteal phase [12,13]. In a meta-analysis carried by Oliveira et al. [14], luteal-phase single-dose injection of GnRHa can increase implantation rate and improve clinical outcomes after ICSI. In this study we aimed to assess whether administration of GnRHa subcutaneously can support the luteal phase without inducing desensitization in patients undergoing controlled ovarian stimulation and IUI.
This was a single-center, prospective, randomized, linked control trial designed to verify the impact of luteal phase support with single dose injection of GnRHa in improving the reproductive outcome in stimulated IUI. After approval of the local ethics committee, the study was performed between December 2011and January 2014 at the Cytogenetic and Endoscopy Unit, Zagazig University Hospital, Egypt. Patients who selected to participate in this work gave their written informed consent before starting. As regards sample size calculation, two-sided significant level 95% with a power of 80% and the ratio of study to control group is 1:1 was applied. According to 25.5% pregnancy rate in the study group and 10% pregnancy rate in the control group as reported by Razieh et al. [15], a minimum of 107 women were needed in each group.
Two hundred fourteen stimulated cycles in 214 infertile women either with unexplained or mild male factor infertility undergoing stimulated IUI was planned to participate in this study. As expecting 5%-10% losses, 18 ladies were excluded as they do not reach the optimum response and the cycles were canceled; (1) non responsive, (2) spontaneous ovulation, (5) excessive number of follicles, (3) did not follow treatment as advised, and (5) lost to follow-up. Lastly after exclusion, 196 couples were involved with the following inclusion criteria; female age was 18-37 years with patent both tubes, normal hormonal profile and accepted semen analysis. Exclusion criteria were a history of ovarian hyper stimulation syndrome (OHSS), endometriosis poor response and previous ovarian surgery. Women with unexplained infertility were diagnosed based on a normal semen analysis according to WHO criteria, confirmed tubal patency and ovulatory menstrual cycles based on mid-luteal progesterone levels or ultrasonic follicle tracking. Mild male factor infertility is established when 2 or more semen analyses have 1 or more variables below the 5th centile (as defined by the WHO, 2010), therefore a sperm count more than 10 million per ml and sperm motility grade (a) and (b) more than 50% in post- processing semen sample was mandatory.
All patients included in the study were subjected to complete history taking and clinical examination. All cycles were gently stimulated after baseline transvaginal ultrasonography (TVS). Ovulation stimulation was done by using low dose step – up protocol begins on the 3rd to the 5th day of the cycle [according to cycle length]. Starting with 75IU highly purified hMG (Merional; IBSA, Lugano, Switzerland) once daily I.M. After 7 days, TVS folliculometry was repeated every 2-3 days. The dose of hMG tailored according to the response. Stimulation continued until one to three follicles reached a mean diameter of 18 mm and the endometrial thickness ≥ 8 mm. Ovulation was triggered by hCG, 10.000 IU, IM (Choriomon, IBSA, Switzerland) administration and single IUI was performed 36 hours later. Intra uterine insemination was done using fresh semen obtained from the husband. All the samples were prepared by swim-up technique. Sonographic evidence of ovulation was change in the ultrasound measurement of the follicle size or the follicle usually disappears from the ultrasound view completely.
Luteal-phase supplementation
At this stage women were divided randomly by using random table (computer), software Open Epi version 3.21 into two groups; study group (GnRHa) group and control (no GnRHa) group. Patients were allocated to either group using the randomization mentioned while allocation concealment concentrated on preventing selection and confusing biases. In Study group; [98 women] single dose of 0.1 mg Triptorelin, (Decapeptyl FERRING Pharmaceutical Pvt. Ltd, Mumbai, India), was given by SC injection 8 days after the insemination, while in the control group (98 women) no injection was used as LPS. Irrespective of whether GnRHa was used as luteal-phase support or not, all women were given vaginal progesterone suppositories 400 mg (Prontogest, GMP Marcyrl) once daily starting at the day of the insemination and continued for two weeks later when a pregnancy test was scheduled.
In this study, day 8 after insemination was selected to inject GnRHa as this the expected time for implantation in IUI cycles which based on a prior study carried by Tesarik et al. [9] in which they injected GnRHa at the expected time of embryo implantation (6 days after ICSI treatment). Ovulation was considered to have occurred when circulating progesterone level is more than 10ng/ml. In both groups, luteal phase length was calculated from 48hrs after the triggering up to and includes the day before the onset of menstruation. Length ≤ 11 days was considered short luteal phase [16].
Hormone assays
The day of hCG injection was defined as luteal Day 0 (LD0). Serum Progesterone level were measured in all cases before triggering, 7 days and 10 days after IUI (LD0, LD 9 and LD12). A biochemical pregnancy was defined by a detection of plasma β-hCG concentration >10 mIU/ml two weeks after insemination. Pregnancy rate was defined as number of patient with serum beta hCG ≥20 mIU/ml on day 14 after insemination divided by the total number of patients. A clinical pregnancy was defined as presence of an intrauterine gestational sac with a heartbeat 3 weeks after a positive hCG test.
Statistically analysis
Data of the study were checked, entered and analyzed by using SPSS (Statistical Product and Service Solutions) version 19. Data were expressed as number and percentage for qualitative variable such as biochemical and clinical pregnancy. Chi-square (X2) test was used to compare the proportions. Mean ± SD for quantitative variables for example duration of infertility, age, BMI, semen parameters and stimulation characteristic. Comparison of quantitative variables between the study and control groups was done using Student’s t-test. P < 0.05 was considered statistically significant.
Between December 2011 and January 2014, two hundred fourteen women had been scheduled for IUI and had been invited to participate in this study. Eighteen women were excluded because they did not reach the optimum response. Finally, 196 women were enrolled and randomized; ninety eight subjects were included in each group. All of them received vaginal progesterone as routine luteal phase support and GnRHa was added for the study group (Figure 1).
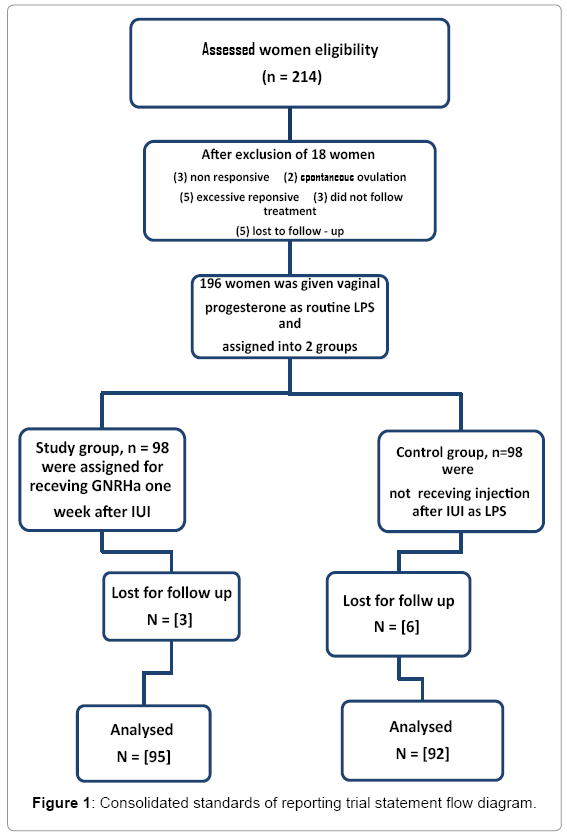
Figure 1: Consolidated standards of reporting trial statement flow diagram.
Table 1, comparing the epidemiological data between the studied groups and demonstrating that there was no statistically significant difference regarding mean age, duration of infertility, BMI, basal hormonal profile as well as preprocessing semen parameters. Regarding stimulation characteristic; total dose of hMG, period of stimulation, mean follicles diameters, as well as total follicles number also post processing semen parameter were similar in both groups (Table 2). As regards circulating level of progesterone, there was no statistically significant difference between both groups either before hCG injection (LD0) or 7 days after insemination [LD9]. However, serum progesterone level 10 after insemination [LD12] was higher in the study group than in the control group (38 ± 5.5 vs. 26 ± 2.5) respectively p < 0.001 which is statistically highly significant. As regards cycle outcome, there was no statistically significant differences in luteal phase length, biochemical and clinical Pregnancy (Table 3).
| Number of couples | Study Group [98] | Control Group [98] | T test | P value |
|---|---|---|---|---|
| Age / year | 25.0 ± 2.1 | 24.4 ± 3.0 | 1.62 | 0.11 |
| Duration of infertility / year | 4.62 ± 1.6 | 4.9 ± 1.0 | 1.46 | 0.14 |
| BMI / kg m2 | 22.8 ± 1.3 | 22.4 ± 1.6 | 1.92 | 0.06 |
| Basal FSH level / IU | 6.1 ± 1.7 | 5.8 ± 1.1 | 1.46 | 0.14 |
| LH / IU | 6 .0± 0.7 | 5.8 ± 0.8 | 1.86 | 0.06 |
| TSH / IU | 2.33 ± 0.82 | 2.43 ±0.24 | 1.15 | 0.25 |
| Prolactin ng/mL | 13.62 ± 4.0 | 12.5 ± 4.5 | 1.84 | 0.06 |
| Pre-processing semen parameters | ||||
| Count (mil/mL) | 29.1 ± 5.9 | 30.0 ± 4.0 | 1.39 | 0.17 |
| Motility (%) | 45.0 ± 5.1 | 44.0 ± 4.9 | 1.41 | 0.16 |
BMI = Body Mass Index; FSH = Follicular Stimulating Hormone; TSH = Thyroid-
Stimulating Hormone; LH = Luteinizing Hormone
Table 1: Demographic data of patients undergoing treatment with (study group) or without (control group) luteal phase GnRHa support.
| Stimulation characteristics | Study Group [98] |
Control Group [98] |
t test |
P Value |
|---|---|---|---|---|
| Total dose of hMG (IU) | 750 ± 37.5 | 737.5 ± 75 | 1.47 | 0.14 |
| Duration of stimulation /day | 10.1 ± 1.05 | 10.4 ± 1.3 | 1.77 | 0.08 |
| Total number of follicles | 2.96 ± 0.8 | 3.1 ± 0.9 | 1.15 | 0.25 |
| Mean follicles diameter(mm) | 19.4 ± 1.5 | 19.0 ± 1.8 | 1.69 | 0.09 |
| Endometrial thickness/mm | 9.1 ± 1.0 | 9.3 ± 0.7 | 1.62 | 0.11 |
| Post-processing semen parameter | ||||
| Count / mil / ml | 21.97 ± 2.71 | 22.7 ± 2.6 | 1.92 | 0.06 |
| Motility (%) | 38.7± 5 | 40.1± 5.5 | 1.73 | 0.08 |
Table 2: Stimulation characteristics of both studied groups.
| Study group | Control group | t test |
P value | |
|---|---|---|---|---|
| Number of couples after 1st exclusion | [ 98 ] | [ 98 ] | ||
| Serum progesterone (ng/ml) before hCG * | 0.90 ± 0.3 | 0.85 ± 0.3 | 1.16 | 0.24 |
| Number of couples after 2nd exclusion | [95] | [92] | ||
| Serum progesterone (ng/ml) | ||||
| Day 7 after IUI (LD9)** | 13.3 ± 1.5 | 13.1 ± 1.8 | 0.82 | 0.41 |
| Day 10 after IUI (LD12)** | 38 ± 5.5 | 26 ± 2.5 | 9.05 | < 0.001 |
| Luteal phase length (days) | 14.6 ± 1.5 | 14.2 ± 1.8 | 1.69 | 0.09 |
| Biochemical pregnancy (cycle) | ||||
| Clinical Pregnancy / (cycle) | 20/95 (21.05%) | 18/92 (19.56%) | χ2= [0.06] | 0.8 |
| 18/95 (18.94%) | 16/92 (17.39%) | χ2= [0.08] | 0.78 |
*hCG = Human Chorionic Gonadotropin; **LD = Luteal Day
Table 3: Luteal-phase characteristics and outcome in both groups.
Normal corpus luteum function requires optimal follicular growth, adequate LH surge, luteinized granulosa cells and continuous stimulant LH pulses. Corpus luteum secretes P that causes secretory changes of the endometrium and accordingly increases the chance of the implantation [7]. Damaged CL leading to deficient luteal phase, harmful effect on oocytes, embryo and endometrium quality, which have been suggested as possible causes of the low pregnancy rate [17]. Single dose injection of GnRH a in the luteal phase was also associated with an increase in implantation, pregnancy and birth rate in recipient women of donated eggs in whom corpus luteum was absence suggesting direct effect of GnRH a on the embryo [9].
Pituitary inducing desensitization by GnRH agonist is depending on the extent and the dose of exposure. Possibly low dose and short acting GnRHa may actually sustain its stimulatory effect and thus restore serum LH levels in favor of maintaining P and E2 levels to support the luteal phase [18]. For this reason in this study, only single dose of GnRHa was used as LPS to induce near-maximal LH level during the luteal phase.
This prospective randomized study was performed to evaluate the effects of GnRHa administration as a single dose [0.1 mg Triptorelin] 8 days after IUI on luteal-phase characteristics and clinical outcomes. The observation showed that there was an increase in serum progesterone level on LD12 in the study group as compared to the controlled group, the difference was seen and it was statistically highly significant (38 ± 5.5 vs. 26 ± 2.5, P < 0.001), respectively. This significantly increase in the progesterone level in GnRHa group and consequently the luteal phase duration increase the pregnancy rate in the GnRHa group but this increase did not reaching the statistical significant level. A singleblinded clinical trial study conducted by Bibi et al. [19] to evaluate the efficacy of luteal phase support with intra vaginal local synthetic progesterone in stimulated IUI cycles, they conclude that there were increasing in progesterone level and prolonged luteal phase, but does not affect success rate in terms of achieving pregnancy. This similarities and differences between these and our results may be attributed to different method used to increase progesterone level either by GnRHa or direct intra vaginal cyclogest application. On the other hand, Erdem et al. [4] found that LPS with vaginal P positively affects the success of stimulated IUI cycles in women with unexplained infertility.
In stimulated IUI cycles, multiples follicles and corpora lutea secrete large amounts of E2, P and inhibin A which characterized by a temporary rise. These temporary increases suppress the levels of LH and FSH to very low level [20], which manifested by low P levels and /or a short luteal phase [21]. Fauser et al. [11] showed that GnRHa induce endogenous FSH and LH surge with physiological luteal phase steroid concentration near to those of normal cycles. So a trial to improve the cycle’s outcome through increase luteal phase P and E2 concentration close to normal level was the desired objective of this study.
Regarding cycle outcome, the biochemical and clinical pregnancy rate were higher in the GnRHa group than in the non GnRHa group (21.05% vs. 19.56%) for the former and (18.94% vs. 17.39%) for the later respectively. The difference was seen but it was not reaching statistically significant level. These results are in agreement with those obtained by Tesarik et al. [22] who described a significant improvement in ICSI cycles outcomes with the similar protocol of single- dose GnRHa administration 6 days after ICSI. This improvement includes implantation and live birth rates as well as in serum P luteal concentrations in both GnRH agonist– and GnRH antagonist treated protocols, suggesting combined beneficial effects on the corpus luteum and on the embryo. Additionally, other studies suggest that the GnRHa could perhaps have a positive effect through its action on the embryo and/or the endometrium. Tesarik et al. [9] showed that there was no increase in miscarriage rates with an improvement in implantation and twin pregnancy rates in recipients of donated eggs who underwent a single dose of GnRHa (0.1 mg of Triptorelin) 6 days after ICSI, compared with placebo. That finding would support the possible positive effects of GnRHa on the embryo and/or the endometrium.
Concerning the embryo, some reports have revealed that GnRH and GnRHa stimulate placental hCG production in vivo [23] and in vitro [24]. Tesarik et al. [22] observed that in women who achieved pregnancy after using triptorelin as LPS in ICSI program, there was an increased secretion of luteal serum hCG by early-implanting embryos and so, improve their implantation potential.
While some studies demonstrated that using GnRHa as luteal phase adjuvant was found to be beneficial [9,22], other studies did not found any significant positive effect either in IUI cycles [25] or ICSI cycles [13]. On the other hand, a meta-analysis carried by Oliveira et al. [14] reveal that single-dose GnRHa in the luteal phase can improve clinical outcomes after ICSI. However, with considering the heterogeneity of the included trials, it seems early to advise the use of GnRH-a in the luteal phase. A study carried by Bellver et al. [25] in which three hundred forty-four women undergoing IUI due to mild to moderate male factor. The women were assigned to two groups: Study group, n = 172 were selected for receiving a single s.c injection of 0.1 mg triptorelin 8 days after hCG administration and control group, n = 172 for receiving solvent only. The authors conclude that injection of GnRHa at the time of implantation does not improve pregnancy rate of IUI cycle. Additionally, a study carried by Ata et al. [13], in which 570 women divided randomly to receive single-dose of 0.1 mg of triptorelin versus placebo 6 days after ICSI in women stimulated with a long GnRHa protocol. They did not find any variations in implantation, clinical pregnancy or multiple pregnancy rates. Another study carried by Kyrou et al. [26] in which 400 IUI cycles was performed, they found that there was no significant difference in cases with and without luteal support, with micronized progesterone. The discrepancy in their results can be attributed to the differences in types of luteal phase support, study population, protocol of ovulation induction.
Van der Linden et al. [27] made seven different comparisons to collect a complete over view of different methods of luteal phase support. They conclude that progesterone is associated with high ongoing pregnancy and birth rate than placebo. Moreover use of one or two doses of GnRH in addition to the progesterone is associated with higher ongoing pregnancy and live birth rates than progesterone alone. In a systematic review carried by Kyrou et al. [28] to detect whether the addition of GnRHa for luteal phase support in IVF / ICSI cycles increase the probability of live birth and they conclude that addition of GnRHa in the luteal phase significantly enhance the probability of live birth rates.
We conclude that even though administration of GnRHa can increase the progesterone level and consequently the duration of luteal phase, the pregnancy rate increase in the GnRHa group but did not reaching the statistical significant level. Definitely there is a need for additional randomized controlled trials to prove the true clinical benefit of luteal phase GnRHa administration before its inclusion established into daily clinical practice to avoid unexpected and undesirable side-effects [29].
The authors thank the clinical and para-clinical staff of cytogentic unit, Zagazig university Hospital for their help and supports in the preparation of this manuscript.