Journal of Defense Management
Open Access
ISSN: 2167-0374
ISSN: 2167-0374
Research Article - (2013) Volume 0, Issue 0
Objective: This prospective study was designed to evaluate the feasibility and outcome of thyroidectomy using Ultrasonically Activated Scalpel (UAS) in comparison to the conventional thyroidectomy. Patients and Methods: This study comprised 40 patients with mean age 41.4 � 9 years, divided into two groups: Group A comprised 25 patients underwent thyroidectomy using UAS and 15 patients underwent conventional thyroidectomy (Group B). Both groups were compared as regards operating time, operative blood loss, postoperative seroma formation and surgeons? satisfaction regarding the ease of dissection, need of blood vessel ligation and dryness of the surgical field. Results: Mean operative time was significantly shorter in group A (77 � 5.8 minutes) compared to group B, (105.7 � 6.5 minutes). Intraoperative blood loss showed a significant reduction in group A, (85 � 5.4 gm) compared to group B (125.3 � 7.8 gm). There was a positive significant correlation between the reduction of intraoperative blood loss and operating time in both groups despite being more significant in group B. Mean total surgeons? satisfaction scores showed a significant difference in favor of satisfaction by using UAS. Conclusion: The use of UAS for thyroidectomy is feasible and could minimize intraoperative bleeding with shorter duration of surgery and had achieved significant surgeons? satisfaction.
Keywords: UAS: Ultrasonically Activated Scalpel; Thyroidectomy
The ideal hemostatic instrument for surgical use would allow the surgeon to grasp and dissect tissue, while at the same time have the capacity to apply an energy source to reliably and rapidly ligate and divide vascular structures with reliable hemostasis and little injury to the surrounding tissues [1]. Currently and widely used mono-polar electrocautery has a non-negligible risk in damaging nerves directly or by thermal diffusion through metallic instruments or fluids. Even coagulated tissue may easily be removed and result in late bleeding [2].
The Ultrasonically Activated Scalpel (UAS) uses high-frequency ultrasound energy and can be used as a substitute for electro-surgery, lasers and steel scalpels in both laparoscopic and conventional surgery. Its unique mechanism of action allows cutting and coagulation without causing a significant rise in temperature at the tissue level [3]. Cutting speed and degree of coagulation can be adjusted to power source and pressure applied on the terminal. Lateral thermal effect is 1-3 mm wide that represents less than a half of the one produced by electrocautery [4]. Its safety has been tested extensively in animal experiments and there is now ample evidence to suggest that it produces less thermal damage in vitro compared to electro-surgery and lasers [5]. Cakan et al. [6] compared the deepness of lung tissue damage caused by UAS and unipolar electrocautery in rats as measured with the ocular micrometer in light microscopy and reported that UAS induces significantly less tissue damage than electrocautery in rat lungs.
This study was designed to evaluate the feasibility and outcome of thyroidectomy using UAS in comparison to the conventional thyroidectomy.
This prospective comparative and pilot study was conducted in General Surgery Department, Armed Forces Hospital Program-Jubil; Saudia Arabia and comprised 40 patients aged 29 to 56 years assigned to undergo thyroidectomy for various indications. Patients were randomly allocated in two groups: Group A, comprised 25 patients underwent thyroidectomy using the UAS and Group B, included 15 patients underwent conventional thyroidectomy.
Technique of thyroidectomy using UAS
The Ultrasonically Activated system consists of a hand piece, cord, console, and foot pedal. We used the CS14C hand piece in all cases; this is composed of an active, curved blade, a protective anvil, and a shaft 12 cm long and 5mm wide.
Transverse collar incision was made and the upper flap was dissected and elevated using the UAS blade. The middle thyroid vein was sealed and transected by using the UAS blade. The superior pole of the thyroid was exposed by retracting the sternohyoid and sternothyroid muscles laterally and superiorly and fully dissected using a right angle dissector, then the upper pole was sealed and transected using the UAS. The UAS was also used in a similar fashion to transect the inferior thyroid veins. After medial rotation of the thyroid gland, various branches of inferior thyroid artery were divided. During this step, every effort was made to identify and protect the recurrent laryngeal nerves and parathyroid glands. The same steps were repeated for the contralateral lobe.
Finally, after irrigation of the wound, the strap muscles and the platysmal layer were approximated using 3-0 polyglactin suture in an interrupted manner. Small-sized closed-suction drainage was used and removed on the second postoperative day. The skin was closed using subcuticular 4-0 nonabsorbable suture.
Both groups were compared as regards operating time, operative blood loss (=weight of wet sponges-weight of dry sponges), postoperative seroma formation and surgeons’ satisfaction regarding the ease of dissection, need of blood vessel ligation and dryness of the surgical field. Surgeons’ satisfaction was graded according 4-grade satisfaction scale: excellent=3, good=2, fair=1 and unsatisfied=0 (Figures 1-8).

Figure 1: The UAS hand piece.
Figure 2: Transverse collar incision.

Figure 3: Elevation of the upper flap using UAS blade.

Figure 4: UAS cutting through the upper pole.

Figure 5: The inferior thyroid veins grasped between the UAS blades.
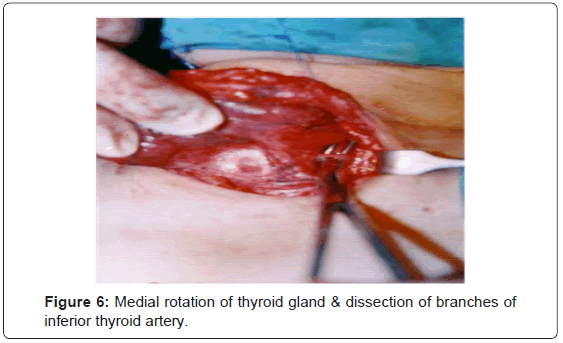
Figure 6: Medial rotation of thyroid gland & dissection of branches of inferior thyroid artery.
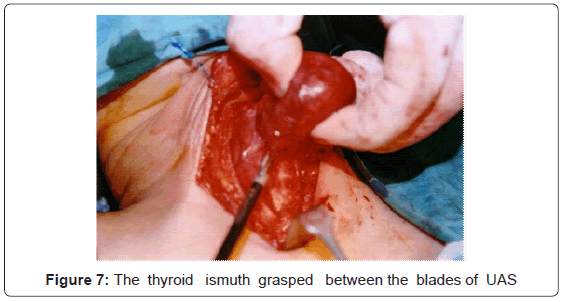
Figure 7: The thyroid ismuth grasped between the blades of UAS

Figure 8: The thyroid bed completely free (without sutures).
Statistical analysis
Data were analyzed using t-test and Chi-square test. Results of postoperative questionnaires were analyzed. Statistical analysis was conducted using the SPSS (Version 10, 2002) for Windows statistical package. P value <0.05 was considered statistically significant.
The study comprised 40 patients; 33 females and 7 males, with mean age 41.4 ± 9, range 29-56 years. There was a non-significant difference between patients enrolled in both groups as regards the age and sex presentation (Table 1).
| Total | Group A | Group B | |
|---|---|---|---|
| Number (%) | 40 | 25 (62.5%) | 15 (37.5%) |
| Age (mean ± SD; years) | 41.4 ± 9 | 42.6 ± 9.4 | 39.2 ± 8.2 |
| Sex; M:F | 7:33 | 4:21 | 3:12 |
Table 1: Patients’ data.
All patients underwent total or near-total thyroidectomy; 7 for primary thyrotoxicosis and 29 for multinodular goiters and 3 patients for papillary carcinoma and one for a follicular carcinoma.
The mean operative time in group A was 77 ± 5.8; range 70-90 minutes, whereas in group B it was 105.7 ± 6.5; range 95-115 minutes, with a significant (P<0.05) decrease of operative time in group A compared to that recorded in group B (Figure 9). The use of UAS was advantageous in cases with primary thyrotoxicosis and cancer thyroid, where its use could significantly (P<0.05) reduce the operative time to 77.5 ± 2.6 and 80 ± 7.1 minutes, respectively, in group A in comparison to 103.3 ± 2.9 and 112.5 ± 3.5 minutes, respectively in group B (Figure 10).
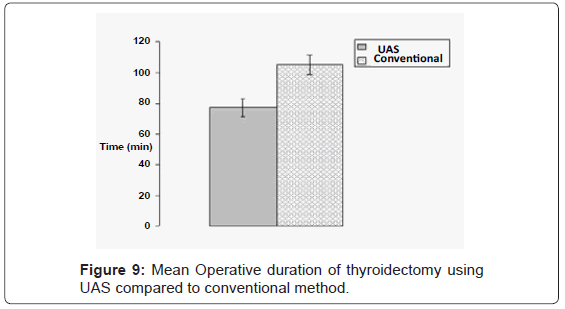
Figure 9: Mean Operative duration of thyroidectomy using UAS compared to conventional method.
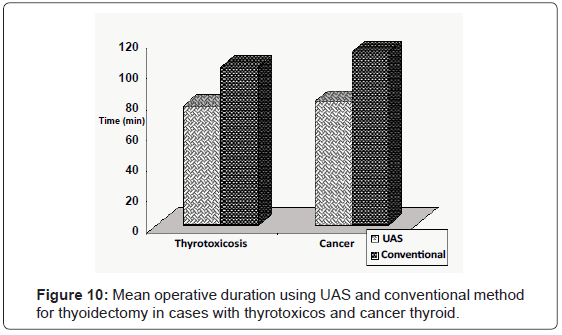
Figure 10: Mean operative duration using UAS and conventional method for thyoidectomy in cases with thyrotoxicos and cancer thyroid.
Similarly, intraoperative blood loss showed a significant (P<0.05) reduction in group A, (85 ± 5.4, range 75-95 gm) compared to amount recorded in group B (125.3 ± 7.8, range 110-140 gm) (Figure 11).
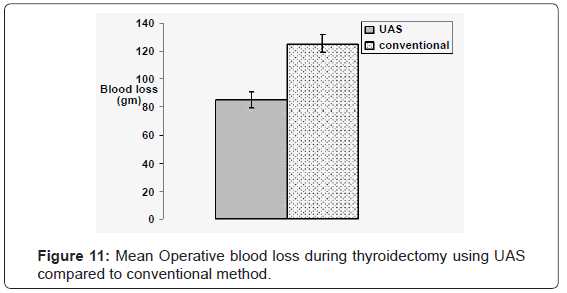
Figure 11: Mean Operative blood loss during thyroidectomy using UAS compared to conventional method.
There was a positive significant correlation between the reduction of intraoperative blood loss and operating time in both groups despite being more significant in group A, (r=0.655, P=0.002 & r=0.595, P=0.011 in groups A& B, respectively) (Figure 12).
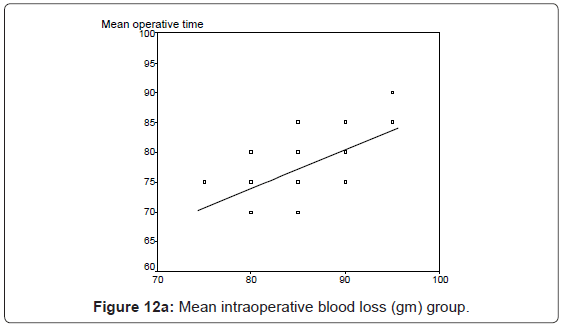
Figure 12a: Mean intraoperative blood loss (gm) group.
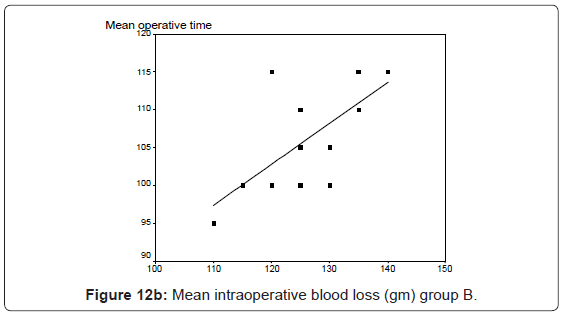
Figure 12b: Mean intraoperative blood loss (gm) group B.
Mean total surgeons’ satisfaction score was 8.6 ± 0.9 in group A while was 6.6 ± 2.1 in group B, with a significant difference in favor of satisfaction by using UAS (Figure 13). Mean scores of sense of ease of surgery, need of blood vessel ligation and dryness of the surgical field were significantly higher with the use of UAS compared to the use of the conventional method (Table 2).

Figure 13: Mean total surgeons’ satisfaction of using UAS vs.conventional method for thyroidectomy.
| Group | Ease of surgery | Need of blood vessel ligation | Dryness of the surgical field | Total score |
|---|---|---|---|---|
| UAS | 2.8 ± 0.4* | 2.96 ± 0.2* | 2.8 ± 0.4* | 8.6 ± 0.9* |
| Conventional | 2.2 ± 0.8 | 2.4 ± 0.5 | 1.9 ± 0.9 | 6.6 ± 2.1 |
*: significant versus conventional method
Table 2: Mean ( ± SD) satisfaction scores in both groups.
No case in either group developed intraoperative nerve injury or had manifestations of hypoparathyroidism. Only one case in UAS group developed postoperative seroma, while in conventional group 2 cases developed seroma.
The mean operative time was significantly shorter in group A (77 ± 5.8; range 70-90 minutes) compared to that recorded in group B (105.7 ± 6.5; range 95-115 minutes). These results agreed with Markogiannakis et al. [7] and Vach et al. [8] who reported that the time of operation is reduced as compared with the classical operation and with Mantke et al. [9], who reported that operative time was shorter in the UAS group than in the conventional technique group (64.68 min versus143.12) and with Ortega et al. [10] who reported a shorter operative time in the UAS group compared with the conventional technique group for both lobectomy and total thyroidectomy.
The use of UAS was advantageous in cases with primary thyrotoxicosis and cancer thyroid, where its use could significantly (P<0.05) reduce the operative time in comparison to group B. These data coincided with Miccoli et al. [11] who reported that the mean operative time was significantly reduced in the UAS for cases requiring total thyroidectomy for cancer thyroid.
Intraoperative blood loss showed a significant (P<0.05) reduction in group A, (85 ± 5.4 gm) compared to the amount recorded in group B (125.3 ± 7.8 gm). This result goes in hand with Shemen [12], Vach et al. [8], Marchesi et al. [13] and Agcaoglu et al. [14] who reported that using the ultrasonic device significantly improves surgical duration and blood loss.
Mean total surgeons’ satisfaction score was 8.6 ± 0.9 in group A while was 6.6 ± 2.1 in group B, with a significant difference in favor of satisfaction by using UAS. This agreed with Raestrup et al. [15] who reported better and easier dissection using UAS with minimal bleeding during thyroidectomy. Mean scores of sense of ease of surgery, need of blood vessel ligation and dryness of the surgical field were significantly higher with the use of UAS compared to the use of the conventional method. These results go in hand with Siprestein et al. [16] who studied the accuracy of and satisfaction by use of the UAS versus conventional knot tying for vessel ligation in thyroid surgery and reported higher satisfaction rate and better dissection and need of blood vessel ligation with the use of UAS.
All patients passed a smooth postoperative course with no nerve injury or hypoparathyroid affection and only one case of seroma in UAS group and 2 in conventional group. These results coincided with that reported by Calò et al. [17], Vach et al. [8] and Ortega et al. [10] who did not observe a statistically significant difference as regards complications (i.e. early postoperative hemorrhage, paresis of the laryngeal recurrent nerve or permanent hypocalcaemia) between UAS and conventional thyroidectomy.
It could be concluded that the use of UAS scalpel for thyroidectomy is feasible and could minimize the intraoperative bleeding with shorter duration of surgery and had achieved significant surgeons’ satisfaction and its use for thyroidectomy is recommended especially in cases with high risk of bleeding and that require extensive dissection as in thyrotoxicosis and cancer thyroid.