Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Research Article - (2013) Volume 1, Issue 1
Children with Autism Spectrum Disorder (ASD) frequently exhibit gastrointestinal (GI) distress. They often have deficiencies of beneficial intestinal microflora, which may lead to inflammation or immune dysfunction, malabsporption, food intolerance, failure to thrive, gas, bloating, constipation or diarrhea. We conducted a survey of caregivers for ASD children with GI distress receiving Delpro®, a nutritional supplement consisting of a mixture of five probiotic strains formulated with the immunomodulator Del-Immune V® (Lactobacillus rhamnosus V lysate). Caregivers assessed ASD signs and symptoms before and after 21 days of treatment using the autism treatment evaluation checklist (ATEC). Almost half of the respondents (48%) reported decreases in diarrhea severity and 52% reported decreases in constipation severity (n=25). Caregivers reported an increase in stool frequency, from one movement every 1.5 days to every 1.3 days, although this change was not statistically significant. Overall, 88% reported a decrease in total ATEC score, signifying an improvement of ASD symptoms. Mean ATEC values decreased from 72.8 prior to treatment to 58.3 following treatment initiation. Participants also had significant improvements in all ATEC domains (speech/language/communication, sociability, sensory/cognitive awareness, and health/physical/behavior). Since this was a survey of caregivers for ASD children with GI distress receiving Delpro®, there was no control arm of no-treatment or placebo. Accordingly, these survey results need to be validated in controlled clinical trials. These data suggest that probiotic/immunomodulator Delpro® may have significant benefit in the treatment of GI distress and other ATEC signs and symptoms among this population.
Keywords: Autism; Probiotics; ASD; Constipation; Diarrhea; Immune dysfunction; Delpro; Del-Immune
Children with autism spectrum disorder (ASD) frequently exhibit gastrointestinal (GI) signs and symptoms [1-5]. Constipation is the most commonly reported GI symptom, with diarrhea, gas and bloating, abdominal pain, esophageal reflux, and vomiting also reported [2,5]. The etiology of these symptoms is not fully understood, and evidence exists suggesting that neuropsychological and inflammatory factors may be involved [6]. Unfortunately, assessment of GI distress—and therefore treatment—can be complicated among ASD children due to communication difficulties. Even children with daily bowel movements may have retention of stool that is not evident to caregivers or healthcare providers [1]. Children with ASD may show stool withholding behaviors related to sensory processing abnormalities [7]. Further, ASD children may also exhibit food selectivity, which may further affect GI symptoms [6,8,9]. There is also a reasonable body of evidence that children with ASD have altered gut flora compared to children without ASD and multiple nutritional deficiencies that can lead to immunological and neurological problems [10,11]. These differences in beneficial bacteria suggest an imbalance in the gut for ASD children. Also, ASD children may experience increased inflammation in the GI tract compared to children without ASD [2,12,13]. These GI symptoms, particularly constipation, gas, and bloating, may cause children to feel early satiety, which may affect food choice. The discomfort may also affect behavior and the ability to focus on other subjects.
While guidelines for the treatment of GI disorders among children without ASD exist, there is little guidance on how to address these issues among ASD children. Dietary interventions have also been reported to aid in alleviation of GI distress, although many reports are anecdotal [14,15]. Gluten and casein restricted diets have frequently been reported in the literature as potential interventions for a variety of ASD symptoms, including GI distress. Treatment of constipation for children has typically focused on the use of lubricants and laxatives. As previous studies indicate that probiotics can affect and restore GI microflora composition, probiotic supplements may be an option for ASD children with GI symptoms [16-18]. Regulation of the GI microflora balance may have important consequences for immune function in this compartment, as changes in intestinal microbiota can affect immune differentiation and may impact inflammatory bowel disease susceptibility [19].
Probiotics have been considered an option to address GI symptoms, both for patients with diarrhea and those with constipation [20]. We investigated the use of a daily probiotic/immunomodulator formulation for the treatment of GI distress in this population. Here, we coupled the probiotic supplement Delpro® with cell wall components from lysed Lactobacillus rhamnosus V as an immunomodulator (Del- Immune V®). After 3 weeks of Delpro® use, caregivers reported changes in stool frequency and tracked health and behavioral changes using a validated tool for the assessment of changes in ASD symptoms, the autism treatment evaluation checklist (ATEC). Caregivers reported significant improvements for ASD children with GI distress in all ATEC domains, improvements in diarrhea and constipation severity, as well as improvements in stool frequency.
Participants
Participants were recruited by Generation Rescue. Thirty-two caregivers representing 33 ASD children participated in the survey. There were no inclusion or exclusion criteria for this survey and participation was voluntary. Potential participants were informed of the intervention composition, safety profile, and study requirements. Informed consent was obtained for all participants.
Intervention
Participants received a six-month supply of Delpro®, a nutritional supplement (Pure Research Products LLC; Boulder, CO, USA). Each capsule contains 10 billion colony forming units (CFUs) of different probiotic strains (Lactocillus acidophilus, Lactobacillus casei, Lactobacillus delbruecki, Bifidobacteria longum, Bifidobacteria bifidum; 2 billion CFUs each) and 8 mg of Del-Immune V® powder. Del-Immune V® powder is a lysed, lyophilized powder, which contains peptidoglycan, muramyl peptides, and nucleotide-containing components or DNA motifs that is derived from L rhamnosus V strain. Participants were advised that the recommended dosage is one capsule three times daily, although dosing schedules were administered by caregivers. As Delpro® contains probiotics, participants were advised to discontinue any concomitant probiotic use.
Measures
Participants were asked to complete a 21-day stool frequency diary prior to Delpro® initiation and another 21-day stool frequency diary following completion of Delpro®. Respondents were also asked to provide ATEC scores prior to and following completion of the intervention. The ATEC is a tool developed by the Autism Treatment Institute used to evaluate autism severity in four categories: 1) speech/language/communication, 2) sociability, 3) sensory/cognitive awareness, and 4) health/physical/behavior [21,22]. In the ATEC scoring system, higher values are given for more severe disease and value decreases represent improvements in severity. ATEC scores are reported for two time points: any time prior to the 21-day therapy period and at 21-days post-treatment.
Statistical analysis
Descriptive statistics were used to analyze the data set. As the data set was of sufficient size and normally distributed, pre- and posttreatment ATEC scores were analyzed using a one-sided paired t test. All analyses were completed using Minitab 16 (State College, PA, USA).
Demographics
Of the thirty-three participants, 25 reported ATEC scores and 21 returned stool frequency diaries. The average age of the participants was 7.92 years (3-16 years). Fourteen were receiving concurrent prescription medications, 6 reported no concurrent prescription medication, and 5 did not report concurrent prescription medications. At baseline, 84% of participants reported “moderate” or “severe” constipation, as assessed by ATEC response. Fifty-six percent of respondents reported “moderate” or “severe” diarrhea.
ATEC results
Mean ATEC score significantly decreased following initiation of treatment, indicating a decrease in severity of ASD symptoms (Figure 1). Of the 25 respondents, 88% reported a decrease in total ATEC score. Of the remaining three respondents, one reported an increase in three ATEC domains, and two reported increases in two domains. Mean ATEC values decreased from 72.8 prior to treatment to 58.3 following treatment initiation (Figure 2, -19.9%; P<.05).
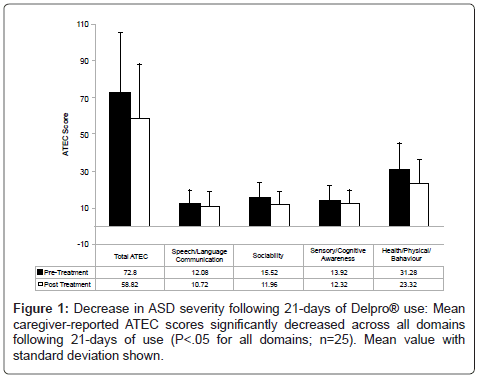
Figure 1: Decrease in ASD severity following 21-days of Delpro® use: Mean caregiver-reported ATEC scores significantly decreased across all domains following 21-days of use (P<.05 for all domains; n=25). Mean value with standard deviation shown.
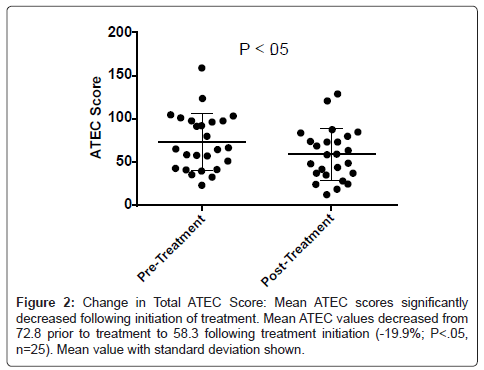
Figure 2: Change in Total ATEC Score: Mean ATEC scores significantly decreased following initiation of treatment. Mean ATEC values decreased from 72.8 prior to treatment to 58.3 following treatment initiation (-19.9%; P<.05, n=25). Mean value with standard deviation shown.
There were significant decreases observed following treatment initiation in all four of the ATEC categories (Figure 3). Mean speech/language/communication ATEC scores decreased from 12.1 prior to treatment to 10.7 following treatment initiation (average decrease of -11.3%; P<.05), with 56% of respondents reporting improvements. Sociability ATEC scores decreased by an average of 22.9% following treatment initiation, from 15.5 to 12.0, with improvements reported among 75% of respondents (P<.05). Sensory/Cognitive Awareness ATEC scores were decreased by an average of 11.5% from 13.9 to 12.3, following treatment initiation with 72% of respondents reporting improvements (P<.05). In the health/physical/behavior domain, ATEC scores decreased by an average of 25.5%, from 31.3 prior to treatment to 23.3 following treatment initiation; 92% percent of respondents reported improvements in this domain (P<.05).
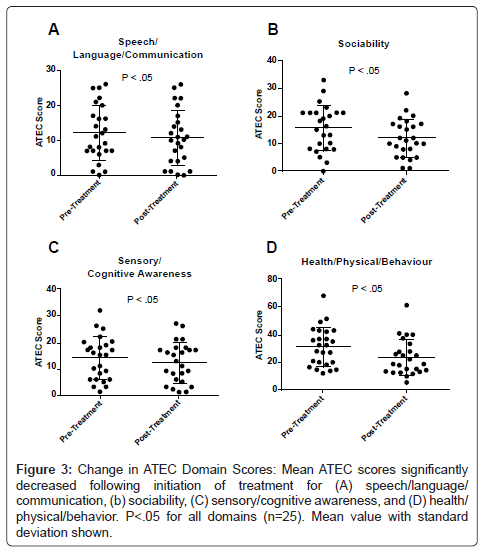
Figure 3: Change in ATEC Domain Scores: Mean ATEC scores significantly decreased following initiation of treatment for (A) speech/language/communication, (b) sociability, (C) sensory/cognitive awareness, and (D) health/physical/behavior. P< . 05 for all domains (n=25). Mean value with standard deviation shown.
Change in GI distress
Twenty-one respondents completed pre-treatment stool logs and 18 completed post-treatment stool logs. The stool frequency increased from one movement every 1.5 days pre-treatment to every 1.3 days post-treatment, with an average of 4.6 movements per week prior to treatment and 5.3 per week during treatment (not significant). The fourth ATEC category (health/physical/behavior) includes two questions specific for GI distress, measuring severity of diarrhea and constipation. Forty-eight percent of respondents reported decreases in diarrhea severity and 52% reported decreases in constipation severity (Table 1). The majority of the remaining respondents reported a decrease or no change in severity, with only one participant reporting an increase in constipation severity and two patients reporting an increase in diarrhea severity. Of those participants who had a decrease in their fourth domain ATEC score, 52% reported a decrease in diarrhea and 57% reported a decrease in constipation severity. Both of the participants who reported an increase in fourth domain ATEC scores also reported no change in constipation severity. Only one respondent who had an increase in this domain score reported an increase in diarrhea severity.
| Severity Change | Diarrhea | Constipation | ||
|---|---|---|---|---|
| n | % | n | % | |
| Decrease | 12 | 48.0 | 13 | 52.0 |
| No Change | 8 | 32.0 | 9 | 36.0 |
| Increase | 2 | 8.0 | 1 | 4.0 |
| Not Reported | 3 | 12.0 | 2 | 8.0 |
| Pre-Delpro® | Post-Delpro® | Pre-Delpro® | Post-Delpro® | |
| Average ATEC Score | 1.0 | 0.4 | 2.4 | 1.6 |
Table 1: Change in Diarrhea and Constipations Severity.
The majority of decreases in the constipation and diarrhea components of the health/physical/behavior component were observed among patients reporting more severe constipation or diarrhea. Compared with 52% of respondents at baseline, 20% reported severe constipation following treatment initiation. No patients reported severe diarrhea after Delpro® use, compared with 20% of pre-treatment patients.
Following initiation of a daily probiotic and immune modulator co-formulation Delpro®, we observed significant improvement in GI symptoms and ATEC-reported results among ASD children as measured by caregiver survey response and ATEC results. Respondents reported specific improvements in constipation and diarrhea, as well as an increase in stool frequency. Caregivers also reported that the children with ASD had significant improvements in all of the ATEC domains (speech/language/communication, sociability, sensory/cognitive awareness, and health/physical/behavior). While adverse events were not recorded in ATEC survey or the stool frequency logs, none of the respondents reported cessation of the intervention.
The stool frequency increased slightly following use of Delpro®, from one movement every 1.5 days to every 1.3 days, although this change was not significant. Additionally, two questions in the health/ physical/behavior ATEC domain specifically address diarrhea and constipation. Of the 22 participants reporting ATEC scores for these two questions, 73% reported an improvement of severity in GI distress. Only one participant reported worsening of constipation severity and two respondents reported an increase in diarrhea severity. For diarrhea, 48% of participants reported improvements; for constipation, 52% of participants reported improvements. It is important to note that the majority of participants in this study reported severe constipation or diarrhea at baseline; many of these participants had a decrease in symptom severity and these improvements were observed rapidly within a three-week time span.
As ATEC scores were recorded at one time point for each period, day-to-day variability may impact these results. However, caregivers also submitted comments with their ATEC scores; these comments suggest that the intervention was generally well-tolerated and frequently resulted in prolonged participant improvements in function (Table 2). As this is a survey, it is difficult to determine if these changes directly resulted from the use of the probiotic/immunomodulator, although respondents generally commented that improvements in health and behavior correlated with Delpro® use. However, there are variables which were not followed which might have impacted these results. For example, respondent diet was not assessed and it is unknown if dietary restriction or changes occurred during the survey course. Children with ASD frequently have food selectivity and dietary interventions are common among this population. Variation in respondent diet was not assessed and this variable may have impacted the survey results [23]. As the duration of the pre- and post-treatment sections of this survey were relatively short at 21 days, though, the impact of this and other variables may have been minimized.
| Participant Number | Comments |
|---|---|
| 1 | •Delpro definitely helped with constipation issues as well as improved heartburn, no need for Nexium. •My son's stomach problems tend to be severe, prevented him from going to school. Was able to attend school more. •Violent tantrums seemed to decrease because he was in less pain. •I have tried a lot of probiotics for my son but Delpro was the only one I have ever seen any improvement. |
| 2 | •[Participant’s] bowel movements helped because he went from hardly going to going almost once a day. •[Participant] has way more focus now than before. |
| 3 | •None |
| 4 | •While so far Delpro has not seemed to help with BMs, I do think that it will take longer than 21 days to truly tell if it has helped. •I do believe that the immunity booster has helped her. She had a very sore throat and a coated white tongue and after 3 capsules of Delpro, it totally disappeared. •While not a cure for illness, I really like this addition and feel it has helped to lessen the severity of colds/viruses which is a benefit for us. |
| 5 | •BMs are more normal. Child is less bloated-decreased appetite to a more appropriate level. •Less stimming behaviors, less obsession with food. •Child was very irritable for first few days, feel that 3 capsules would be too strong for a smaller child. |
| 6 | •It has not helped with constipation or BMs-caused excess gas/bloating. •It has not made any difference behaviorally. •I think that [participant] will need more than 21 days to show improvement on Delpro. I am going to watch very closely while he uses the additional supply to see if the Del-Immune component helps during the winter/fall months, as this is typically when he is sick almost the entire time. •I feel that the immunity booster is helping lessen the severity of viruses. |
| 7 | •Caused a lot of excess gas but did not really make a difference in BMs except in initial week. •I did not see any clear improvements with behaviors. •I think that it will take longer than the 3 weeks to determine if the product is really effective. •I feel that the immunity booster, while not totally preventing illness, has helped to lessen the severity and duration of viruses which has been helpful. |
| 8 | •He seems to be more willing to go to the bathroom and has even gone on his own recently. •His behavior seems about the same. •His stools are not nearly as big and hard. They are now floating, not sinking. |
| 9 | •[Participant’s] BMs are pretty regular; however, they were soft. The Delpro helped keep them more firm. •[Participant] seemed to giggle a lot and be more happier. •I especially like the fact that it tastes pleasant because I have to open the capsules and sprinkle on food. It’s great that I don’t have a hard time getting him to take it. |
| 10 | •None |
| 11 | •None |
| 12 | •We were using probiotics before 50 billion CPU's. He got a lot more moody and upset and in more pain. Since we were using a higher dosage, we encountered problems when we reduced the dosage. |
| 13 | •For the first days his bowel movement were better, but then they went back to be very hard stools. •When the hard stool came back his behavior was bad, a lot of stimming and hitting himself. •Except for the hard stool toward the middle of the study there were no other problems during the study. |
| 14 | •Helped make BM's regular and more solid-minimal stomach aches. •More happy on days didn’t have BM or missed pills very agitated and angry. Has helped him be happier with 0- minimal stomach aches. |
| 15 | •It was hard to tell if there were much change but at times it did seem to help. •I think there was a small percentage of positive change though. |
| 16 | •Definitely saw improvements in stool firmness, consistency and more normal color. • Yeast was easier to manage, there were some holidays in between the log, so there were some flare-ups, but easy to manage. •Most noteworthy was the cradle cap he has had on his head, just came flaking off. The majority of it is gone. •I am glad to have participated in the study as I have seen huge improvements from where we were before starting. |
| 17 | •The bowel movements were more regular than before. |
| 18 | •Was helpful with BMs because consistently was getting normal looking daily stools except 1 day. •She's overall from weeks prior been a happier girl and laughing at everything. •Since being out of the probiotic we've started having some runny stools again which seemed to go away when taking Delpro; of course she's been sick with a cold too, so not sure what to relate things to. |
| 19 | •I think that his body is still adjusting to the product. •He is getting easier to deal with no temper outburst. •The product was easy to take. •I think he will be more regular with another batch. |
| 20 | •Son had a hard time pushing out BM's before, with Delpro it seemed to come out a lot easier with him straining to push. •Son was somewhat lethargic seem to be opening up more and seems more relaxed. •Bowel movements were consistent and had a more natural appearance than before. |
| 21 | •I'm really grateful for this study/opportunity. •We've been working on his poop for 2 years and this is the only thing that's really made a huge difference. |
| 22 | •My daughter was always constipated and barely had a BM a day. If she did it was a couple of pellet-sized. Now she is going 2-3 times a day to have a BM! This is a dramatic change. •My daughter was usually quiet and wanted to be by herself. Now when she goes potty she is more happy and tells me she has to go and what she has to do, she is more happy and at ease. •Every child's body is different and I expected a withdrawal or tantrums but instead my daughter was more livelier after Delpro regulated in her system. |
| 23-25 (Reported Together) | •The boys seemed to be more attentive while doing Delpro and more cooperative. They both got sick at the same time soon after starting Delpro and I wondered if they were detoxing or something because no one else in the house got sick. •[One paticipant’s] constipation got better and she wasn't stimming as much. •A few days I didn't give the Delpro and they all became lethargic. They didn't feel like working at school and didn't want to get up in the morning. •I will say that my children all have severe yeast issues and I think that while they were on the Delpro the signs and symptoms of severe yeast decreased. Specifically the clearer head, which for my oldest son is his worst symptom. •I can say that I saw tremendous improvement with my sons when they took the Delpro and I would continue giving them Delpro because of those results. |
Table 2: Caregiver Comments Following Treatment with Delpro®.
While definitions between studies differ, the weight of evidence suggests that constipation and other GI symptoms are more common among children with ASD. One pediatric constipation clinic in the United Kingdom reported that ASDs were an order-of-magnitude more frequent than the general population [24]. A large US survey found that ASD children were more than seven-times more likely to have frequent diarrhea/colitis compared to children without developmental disorders [25]. The causes of GI distress among children with ASD have not been definitively determined. Frequent constipation could be impacted by neuropsychological factors, such as withholding. GI inflammation has also been reported in ASD children. There have been reports of enterocolitis among ASD children, but a review of these studies found frequent study inconsistencies and misinterpretation of biopsies and other studies have not supported these findings [26,27]. Variability in the literature on this subject may be due, in part, to heterogeneity in both GI symptoms and autism itself.
There is evidence to warrant the investigation of probiotic formulations and immunomodulators for the treatment of GI distress in this population. Children with ASD appear to have an altered microbiome in the GI tract compared to children without ASD. One study investigating gut microflora differences in ASD children found that children with ASD had a higher incidence of Clostridium histolyticum group bacteria compared with healthy controls [28]. Finegold et al. [29] also report significant differences in fecal microflora between autistic and control children. They also observed a greater count of clostridia in stool from ASD children, with nine closdridial species found only among the ASD children [30]. ASD children have been shown to have lower levels of Bifidobacterium compared to controls, and higher levels of Lactobacilli [29,31]. These differences in beneficial bacteria suggest an imbalance in the gut for ASD children. Children with ASD who have GI issues have been shown to have microbial dysbioses in the mucoepithelium and this dysbioses is associated with gene expression differences for some carbohydrate metabolism genes [32]. As previous studies indicate that probiotics can affect and normalize GI microflora composition, probiotic supplements may be an option for ASD children with GI symptoms [16-18]. A recent pilot study found that Bifidobacterium breve was effective in increasing the stool frequency among a small group of constipated children without ASD [33]. Another study of ASD children receiving probiotics found changes in the levels in urine of metabolites associated with Candida species, suggesting an alteration of the gut microflora [34]. Accordingly, a recent survey found that almost 20% of providers treating ASD patients encourage probiotic use, and almost 60% accept their use [35]. Probiotic microorganisms in formulation should be capable of meeting efficacy and safety criteria and the probiotic mix used in this study was based on studies of industrial strains of Lactobacilli and Bifidobacterium [36]. These strains were determined to be capable of surviving gastric juice and at different bile concentrations. Regulation of the GI microflora balance may have important consequences for immune function in this compartment, as changes in intestinal microbiota can affect immune differentiation and may impact inflammatory bowel disease susceptibility [19].
Based on these data and the reported GI inflammation and immune dysfunction in ASD children, the therapy used in this survey also included an immunomodulator. Jyonouchi et al. [37] reported that peripheral blood mononuclear cells from young children with ASD and GI symptoms had increased production of TNF-alpha and IL-12 compared to children with ASD without GI symptoms. de Magistris et al. [38] reported increased GI inflammation among ASD children compared to children without ASD, as assessed by fecal calprotectin. However, other studies have observed no differences in rectal nitric oxide and fecal calprotectin between ASD children and controls, so it remains undetermined whether inflammation is a common feature among ASD children with GI symptoms [39]. In addition to the probiotic component of Delpro®, participants received lysed cells of L rhamnosus V (Del-Immune V®), which has been shown to increase serum levels of interferons (IFNs), including IFN-alpha/beta and IFN-gamma. Del-Immune V has also been shown to increase TNF-alpha and natural killer cells in mice [40]. Lysed probiotic cells have also demonstrated ability to stimulate IFNs, as well as other cytokines including IL-1, IL-6, IL-8, IL-10, and IL-12. [41-44]. While these components have been shown to affect cytokine production, the consequences of these changes in the gut among this population is still undetermined, bit warrants further research.
It is important to recognize that this report is subject to several limitations. As improvements were caregiver reported, there is no standardization of stool consistency. Since this was a survey of caregivers for ASD children with GI distress receiving Delpro®, there was no control arm of no-treatment or placebo. Further, participants volunteered for this study, which may have introduced a selection bias. While the sample size was small, statistical analyses were able to discern significant improvements in all ATEC measures. Moreover, the lack of regular scheduled ATEC assessments limits the interpretation of these results, which need to be verified by controlled trials. Survey respondents also may have been on concurrent medications, although all participants were advised not to use concomitant probiotics. As with all evaluations of interventions for ASD or associated symptoms, ASD heterogeneity and variety in GI symptoms may have a significant impact on the effectiveness of the intervention. Further, children with ASD frequently have food selectivity and dietary interventions are common among this population. Variation in respondent diet was not assessed and this variable may have impacted the survey results. As the duration of the pre- and post-treatment sections of this survey was relatively short at 21 days, though, the impact of this variable may have been minimized.” Despite these limitations, the results reported here are in agreement with those reported in the literature for a similar intervention. A 2010 trial of cell wall lysed probiotic tincture use for 35 days among ASD ten children showed a decrease in enteric bacteria levels and a decrease in severity in all ATEC domains [45]. Future studies may examine the effect of Delpro® on stool changes.
With autism rates rising dramatically in recent years, there is an ever-increasing need to identify remedies for common issues among children with ASD. In a recent pilot study of ASD children on a glutenfree, casein-free diet, caregivers reported improved GI symptoms and behavior patterns [46]. Nutritional supplements may be well-positioned to help with the commonly reported gastrointestinal problems among children with ASD. According to the findings in this study, the probiotic/immunomodulator formulation Delpro® holds promise as a potential remedy for children with ASD and GI dysfunction or abnormal stool testing. Future controlled trials of Delpro® will assess this potential.
We would like to thank all of the families who participated in this survey. Medical writer Michael Linde assisted in the pr eparation of this manuscript.