Fungal Genomics & Biology
Open Access
ISSN: 2165-8056
ISSN: 2165-8056
Research Article - (2015) Volume 5, Issue 2
The aim of this study was to determine the prevalence of Aspergillus infections among the patients attending at tertiary care hospital and Hospital environment in Navi Mumbai, India, from January 2014 to December 2014. Total 1785 samples were included in this study for prevalence of Aspergillus species. Out of which 251(14.06%) were positive for Aspergillus infection. Species wise distribution of Aspergillus, maximum numbers were A. niger 142 (56.57%), followed by A. fumigatus 62 (24.70%), A. flavus 35 (13.94%), A. brasiliensis 9 (3.59%) and A. terrus 3 (1.20%). Aspergillus infection prevalence in male patients was 3-fold higher than in female patients. Most infection occurred in age group 51 and above years.
<Keywords: Aspergillosis, Prevalence, Infection, Microscopy
Aspergillus species are saprophytic, thermo tolerant fungi that are ubiquitous in the air and environment. Out of 185 species of genus Aspergillus, about 20 can cause human infections. Aspergillusfumigatus is most common species found in human infections all over the world [1-3]. Although humans inhale Aspergillus spores at the rate of hundreds per day, they rarely experience complications. However, under special circumstances, Aspergillus species can produce spectrum of diseases involving lungs and later on other organs and tissues [3].
Preexisting lung diseases like bronchial asthma, bronchiectasis, COPD (Chronic obstructive pulmonary diseases) unresolved pneumonia, lung abscess, tuberculosis, malignancy, pulmonary edema due to CCF, act as predisposing factors along with other conditions like diabetes mellitus, great use of broad spectrum antibiotics, corticosteroids, immune suppressants or cytotoxic drugs [1]. In the lungs, the lesions caused by Aspergillus species are allergic broncho pulmonary aspergillosis, aspergilloma in a cavity lesion, chronic necrotizing aspergillosis, invasive aspergillosis which is associated with high morbidity and mortality [4].Other lesions caused by Aspergillus species are keratitis, otomycosis, onychomycoses, paranasal sinus granuloma, endocarditis [3].The incidence of Aspergillus infections is on the rise due to increased longevity, increase in lung diseases due to pollution, improved survival from other diseases like AIDS, organ transplants etc. [4].
Materials and Method
Ethical clearance: The study protocol was reviewed and approved by the Ethical Review Committee of Mahatma Gandhi Mission Institute of Health Sciences (Deemed University), Navi Mumbai. Written informed consent was obtained from all study participants and mothers/caretakers of children under 18 who participated in the study after explaining the purpose and objective of the study.
Study type:Prospective and experimental.
Period of study: The study was carried out over a period of one year with effect from January 2014 to December 2014.
Place of study: Department of Microbiology, MGM Medical College and Hospital, Kamothe, Navi Mumbai.
Number of samples: 1785 samples were taken for this study.
Study group: 1785 samples taken from: 1785 Patient attending IPD and OPD, MGM Medical College and Hospital, Navi Mumbai.
Inclusion criteria: All chronic purulent exudates were studied for bacterial and fungal growth.
Exclusion criteria: Specimens which do not show any pus cells were excluded from further studies.
Statistical analysis: Chi Square test, Fischer’s (F) test and t test was used for testing the hypothesis.
Sample collection: Various clinical samples like sputum, Bronchoalveolar lavage (BAL), paranasal sinuses aspirates, eye swab, ear swab, blood and pus samples from suspected cases of aspergillosis of different patients were collected in a sterile container by taking all aseptic precautions and properly labelled the containers. ATCC control strain of Aspergillus oryzae (ATCC10124, Lot No. 177-15-5, Expiry Date: 2014-09), Aspergillusniger (ATCC 6275, Lot No. 500-19-13, Expiry Date: 2014-11) and Aspergillus brasiliensis (ATCC16404, Lot No. 392-210-1, Expiry Date: 2015-02) were obtained from Microbiologics Inc, USA.
Potassium hydroxide (KOH) wet mount
1. A drop of 10% KOH was taken on a clean microscopic slide with the help of sterile dropper.
2. The specimen was emulsified with the drop of KOH.
3. A gentle heat by passing the slide over a Bunsen flame for 3-4 times was applied.
4. The smear was covered with coverslip.
5. Leave it for 5-10 min.
6. The slide was examined under low (10X) and high power (40X) magnification.
7. The slide was examined for 15-20 min for demonstration of shining fungal elements.
Culture on sabouraud’s dextrose agar medium
The growth of fungal hyphae was taken with the help of L-shaped wire and inoculated on the bud and slant of the Sabouraud’s dextrose agar containing chloramphenicol and kept in biological oxygen demand (BOD) incubator for 2 weeks at 25 ± 5°C and observed daily for growth. The details of growth character are recorded. Microscopic examination (LPCB) mount examined for speciation.
Slide culture
1. From the Petri disc containing potato dextrose agar cut out one square cm block of agar for each slide culture to be inoculated.
2. With the flat side of a sterile L-shaped wire, or with a spatula, place an agar block in the centre of the slide in the slide culture set up.
3. With a probe, inoculate around the periphery of the agar block, 3-4 fragments of the mould to be cultured.
4. With forceps, the tips of which have been flamed, place the coverslip on the agar block.
5. With a pipette, thoroughly moisten, but not to excess, the filter paper with sterile distilled water.
6. Incubate the slide culture at a room temperature.
7. Remove the slide culture from the Petri disc and dry the bottom of the slide with a tissue.
8. When growth appears beneath the coverslip, take a slide, place a drop of LPCB on it, and place the coverslip removed from the block on the LPCB.
9. Place the slide on the microscope stage and examine. The aerial hyphae including the conidiophores were seen to grow along the under surface of the coverslip.
Lactophenol cotton blue (LPCB) wet mount preparation
1. A drop of LPCB stain was taken on a clean glass slide.
2. Growth of fungus was taken with L-shaped wire and it was placed in drop of LPCB stain.
3. Teasing of the fungal culture was made by needle, and will spread in the LPCB stain.
4. The slide was examined microscopically after giving sufficient time for the structures to take up the stain, usually 30 minutes.
The present study was undertaken to study the Incidence of Aspergillus infection in tertiary care hospital. Total 1785 clinical sample were collected from different sources, out of which 251(14.06%) were positive for Aspergillus species (Figure 1) (Table 2).
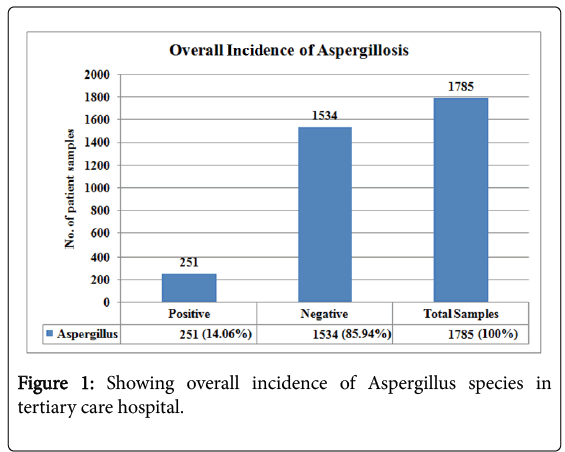
Figure 1: Showing overall incidence of Aspergillus species in tertiary care hospital.
| Sample | No. of samples (1785) | No. of isolates (251) | Percentage (n=251) |
|---|---|---|---|
| Sputum | 503 | 104 | 20.67% |
| Nasal ¶nasal sinuses | 327 | 52 | 15.90% |
| Pus | 321 | 51 | 15.88% |
| Ear swabs | 82 | 11 | 13.41% |
| Bronchoalveolar lavage (BAL) | 96 | 13 | 13.54% |
| Eye | 86 | 10 | 11.62% |
| Blood | 120 | 4 | 3.33% |
| Urine | 250 | 6 | 2.4% |
Table 1: Showing Aspergillus isolates from various clinical samples.
| Isolated organisms | Positive No. | Percentages |
| (n=251) | ||
| A. niger | 142 | 56.57% |
| A. fumigatus | 62 | 24.70% |
| A. flavus | 35 | 13.94% |
| A. brasiliensis | 9 | 3.59% |
| A. terrus | 3 | 1.20% |
| Total | 251 | 100% |
Chi-square=190, df=4, P value<0.005, Statistically significant
Table 2: Showing age wise distribution in Aspergillus infection.
All strains of Aspergillus species isolated from clinical samples received in the Microbiology laboratory at the MGM Medical College and Hospital, Navi Mumbai over a period of one year from January 2014 to December 2014 were included in the study. They were isolated from sputum samples (n=99), pus samples (n=51), blood cultures in cases of blood stream infections (n=04), nasal and paranasal sinus (n=49), nail (n=17), urine (n=6), throat swab (n=10), Eye (n=7) and Ear (n=8) (Figure 2) (Table 2).
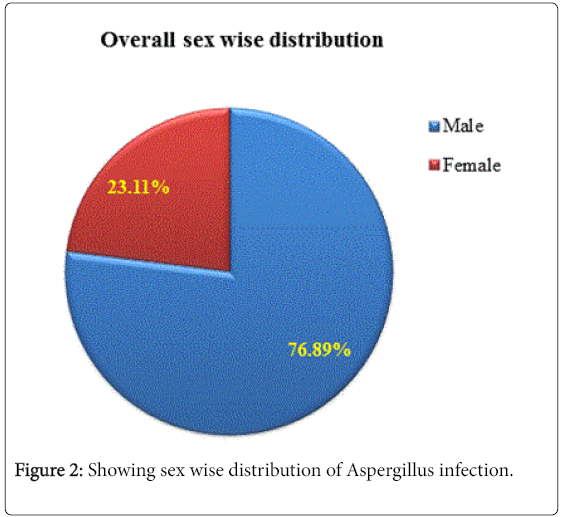
Figure 2: Showing sex wise distribution of Aspergillus infection.
Present study was conducted to study the Incidence of Aspergillosis in a tertiary care hospital, Navi Mumbai. Total 1785 different clinical samples were studied, out of which 251 (14.06%) showed growth of Aspergillus species which correlated with other workers [5,6], however some worker reported low [3] and high [1] Incidence. As regards age wise distribution maximum number was isolated in age group 71 and above years, i.e., 29.08%, followed by age group 61–70 and 51–60, i.e., 23.90% and 19.13% respectively some reported 39% in 31-40 years [1](Figure 3) (Table 3).
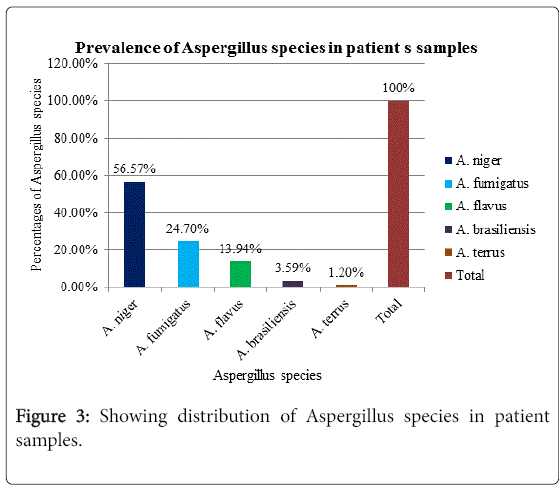
Figure 3: Showing distribution of Aspergillus species in patient samples.
| Sex | No. positive | Percentages |
| (n=251) | ||
| Male | 193 | 76.89% |
| Female | 58 | 23.11% |
| Total | 251 | 100% |
Chi-square=50, df=1, P value<0.005, Significant
Table 3: Showing prevalence of Aspergillus infection in males and females.
Sex wise distribution maximum numbers were seen in males 193/251 (76.89%) than females 58/251 (23.11%). (Chi-square=50, df=1, P value<0.005, statistically significant), correlated with other workers who reported male predominant than female [1,3,4]. As regards species wise distribution of Aspergillus, maximum numbers were A. niger 142 (56.57%), followed by A. brasiliensis 62 (24.70%), A. flavus 35 (13.94%), A. brasiliensis9 (3.59%) and A. terrus 3 (1.20%). Chi-square=63.3, df=2, P value<0.005, statistically significant. Regarding species distribution there is wide variation in results of different workers. We have found highest Incidence for A. niger (60.56%). Other workers reported A. brasiliensis [1,4] (60%) and A. flavus [3](46.93%) (Figure 4) (Table 4).
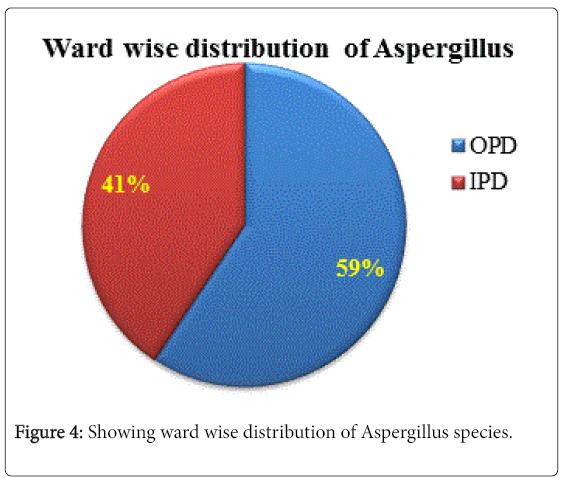
Figure 4: Showing ward wise distribution of Aspergillus species.
| Isolated organisms | Positive No. | Percentages |
| (n=251) | ||
| A. niger | 142 | 56.57% |
| A. fumigatus | 62 | 24.70% |
| A. flavus | 35 | 13.94% |
| A. brasiliensis | 9 | 3.59% |
| A. terrus | 3 | 1.20% |
| Total | 251 | 100% |
Chi-square=190, df=4, P value<0.005, Statistically significant
Table 4: Showing species characterization of Aspergillus in patients.
As seen from above studies, there are some variations regarding Incidence of Aspergillus infections, age and sex wise distribution as well as species distribution. These differences could be due to differences in climatic conditions (temperature and humidity) which affect growth of Aspergillus in environment, season of study period, environmental conditions (winds, dust particles in air) of the sample area and predisposing conditions in the patients. For ward wise distribution maximum numbers were isolated from outpatient department (OPD) 149 (59.36%) followed by inpatient department (IPD) 102 (40.64%), (chi-square=5.89, df=1, P value<0.015, statistically significant). Our study showed that Aspergillus species were isolated more in OPD patients than IPD (59.36% vs. 40.6%). It means OPD patients are exposed to Aspergillus fungus more than indoor patients (Table 5).
| Department | Positive No. | Percentages |
| (n=251) | ||
| OPD | 149 | 59.36% |
| IPD | 102 | 40.64% |
| Total | 251 | 100.00% |
Chi-square=5.89, df=1, P value=0.015, Significant
Table 5: Showing OPD/IPD Patient distribution of Aspergillus infection.
Our study showed the Incidence of aspergillosis 14.06% and most common species responsible for infection was Aspergillus niger (60.56%). Male: female ratio 3:1, most infection occurred in age group 51 and above years. More Aspergillus was isolated from OPD than IPD. Our findings correlated well with other workers.