Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2016) Volume 6, Issue 4
Background: Pancreatic-adenocarcinoma is relatively uncommon, but has been proven to be an unyielding adversity. Although it is known the importance of exercise in improving quality of life in cancer patients, currently there are no available data identifying the inflammatory-response during exercise in pancreatic-cancer patients undergoing chemotherapy. Methods: A control-supported case study was performed on a 67 yr old man diagnosed with stage IV pancreaticcancer. Two 24-hour non-stop ultra-endurance walking races (24 hr Walk) completed by the patient prior to cancerdiagnosis (No Chemo, 6 months prior to the diagnosis) and after cancer-diagnosis during chemotherapy (Chemo) were compared. Comparison to control-participants without cancer (n=2, Ctrl 1 and Ctrl 2) was also conducted. Throughout 24 hr Walk blood-samples were collected every 6 hours and analyzed for intereukin-1β (IL-1β), interleukin-1ra (IL-1ra), interleukin-6 (IL-6), interleukin-8 (IL-8), interleukin-10 (IL-10), tumor necrosis factor-α (TNF-α), monochemoattractant protein-1 (MCP-1), C-reactive protein (CRP), alanine aminotransferase (ALT), pancreatic amylase (AmylP), and albumin. All training performed since the cancer-diagnosis was monitored. Results: No adverse events occurred neither during 24 hr walks nor during the training. The number of walk per week, distance, and speed diminished following the diagnosis of pancreatic-cancer. Changes in IL-1β, IL-6, IL-8, IL-10, TNF-α, MCP-1, ALT, AmylP, and albumin did not differ between No Chemo and Chemo. IL-1ra decreased in No Chemo, but increased in Chemo. CRP increased in both No Chemo and Chemo, and in the controls as well. Changes in ALT and AmylP in Ctrl 1 and Ctrl 2 differed to both No Chemo and Chemo. Conclusions: Understanding the inflammatory-response to exercise in cancer-patients may be useful to design and delivery adapted exercise-programs in this growing population. The inflammatory-response, hepatic, and pancreatic functionality during prolonged-exercise were not exacerbated by concurrent chemotherapy in a pancreatic-cancer patient.
<Pancreatic-adenocarcinoma is relatively uncommon [1], but has been proven to be an unyielding adversity [2]. Pancreatic-cancer accounts only ~3% of all cancer diagnoses and is the fourth cause of death for cancer in USA [2,3]. These rates are similar in Italy, where pancreatic-cancer accounts only 3% of all cancer diagnoses and is the fifth cause of death. This equates to 7% of all cancer deaths [4] with a total of ~10,000 lives lost to pancreatic-cancer in 2009 [5].
Exercise has demonstrated efficacy for the management of treatment related side effects and for improving quality of life (QOL) across common cancers such as breast and prostate-cancer [6]. However very little data exists exploring the potential impact of exercise in pancreatic-cancer patients despite the need to counteract commonly experience adverse effects including significant weight-loss, cancerrelated fatigue, nausea, and psychological distress [2,3,7]. In 2014, a study reported a case study involving a 49-yr old man with pancreaticcancer [8]. The exercise intervention included twice a week sessions of moderate-to-high intensity resistance and aerobic-training for 6 months. Exercise was well tolerated during adjuvant-chemotherapy for pancreatic-cancer and led to a range of improvements for this patient including considerably improved QOL.
Currently there are no available data identifying the inflammatoryresponse during exercise in pancreatic-cancer patients. In healthy adults, high intensity and/or prolonged-exercise leads to muscle and other tissue-damage causing an increased inflammatory-response, involving several types of blood cells and pro-inflammatory cytokines [9]. During prolonged-exercise, the pattern of inflammatoryresponse is different from the response to other kind of stress (e.g., hyperthermia, hemorrhagic-shock). Furthermore, even when same cytokines (e.g., interleukin-6, interleukin-10, MCP-1) are activated during both exercise and in cancer environment, they may have different function and trigger different mechanisms (Table 1). In fact, the response to prolonged-exercise is featured by a marked elevation in circulating cytokines including interleukin-1 receptor antagonist (IL-1ra), interleukin-6 (IL-6), and interleukin-10 (IL-10), which varies according to exercise-duration (Table 1) [9]. This is in contrast to the level of circulating interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α), which are commonly blunted or absent [10]. Exercise also induces counter-regulation of inflammation through secretion of immunosuppressant mediators, such as cortisol and anti-inflammatory cytokines. In addition, levels of positive acute-phase response-proteins, such as C-reactive protein (CRP), increase during a bout of exercise, whereas levels of negative ones, such as albumin and transferrin, decrease [11].
| Pancreatic cancer | During strenous/intense exercise | |
|---|---|---|
| IL-1β | Enhances the adhesion of pancreatic-carcinoma cell lines to the microvascular endothelium | ↓ slightly |
| IL-1ra | Inhibits IL-1 release during acute phase inflammatory response | ↑ Inhibits IL-1β; enhances systemic levels of cortisol |
| IL-6 | Enables tumor growth and inhibits apoptosis; alters lipid and protein metabolisms, inhibits biosynthesis by adipocytes and causes atrophy and increased catabolism of muscle protein | ↑ Acting as an energy sensor for mobilizing extra-cellular substrates; inhibits TNF-α, and IL-1β; increases IL-1ra and IL-10; maintains high plasmatic levels of cortisol. Related to duration of exercise. |
| IL-8 | Promotes angiogenic response in endothelial cells; increases proliferation and survival of endothelial and cancer-cells; potentiates cell migration of the tumor site | ↑ High local expression; would bechemoattraction on neutrophils and macrophages; stimulate angiogenesis |
| IL-10 | Pro-inflammatory effect enhancing release of IL-1 and TNF-α | ↑ Enhances systemic levels of cortisol |
| MCP-1 | Potent angiogenic factor by recruiting tumor-infiltrating macrophages and subsequently the production of angiogenic growth factors | ↑ Promotes muscle regeneration and functional recovery through regulation of monocyte/macrophage recruitment or activation |
| TNF-α | Enhances tumor growth and metastasis; enhances the adhesion of pancreatic-carcinoma cell lines to the microvascular endothelium | = or ↑/↓ slightly Facilitates the migration of immune cells in injured tissue. Results of systemic endoxemia induced by decrease in blood flow to the splanchnic bed. Related to duration and intensity of exercise. |
| CRP | Marker for acute chronic inflammation; induced by rise in IL-6 values; exerts inhibitory effects on tumor proliferation; angiogenesis and distant metastasis | ↑ Marker of acute phase response |
In recent literature, it has been reported that IL-1, IL-6, and TNF-α promote inflammation-associated carcinogenesis and influence chemo-resistance in pancreatic-tumors [12]. Specifically, these interleukins induce the activation of several transcription factors culminating in the formation of numerous pro-inflammatory molecules that recruit and activate various leukocyte populations into the tumor microenvironment [12]. These and other inflammatory mechanisms contribute to pancreatic-cancer development (Table 1) [13]. The principal cytokines involved in pancreatic-cancer are: interleukin-1β, IL-ra, IL-6, interleukin-8 (IL-8), IL-10, monocyte chemoattractant protein 1 (MCP-1), TNF-α, and CRP. Furthermore there is increasing evidence that systemic inflammation may mediate a number of metabolic processes that contribute to cancer-cachexia [14,15]. A study demonstrated that a proportion of pancreatic-cancer patients who lose weight have an elevated hepatic acute-phase proteinresponse (APPR), which correlates to both increased resting energy expenditure and duration of survival [14]. The principal regulator of APPR in human hepatocytes is thought to be IL-6 [14].
Cancer and its treatment impact systemic levels of inflammation, as does exercise. Although exercise has been found to effectively improve QOL, decrease fatigue levels, and improve physical-functioning, very little information is available exploring the inflammatory-response of pancreatic-cancer patients to exercise. The duration and intensity of exercise influences the inflammatory, but it is unclear if there are any interaction effects of prolonged-exercise cancer and its treatment. Therefore, the first aim of this study was to investigate whether the inflammatory-response to prolonged-exercise, such a 24-hour nonstop ultra-endurance walking, is impacted by chemotherapy for the treatment of pancreatic-cancer.
Subjects
Pancreatic-cancer patient: This case study involved an Italian 67- yr old man (mass 63.5 kg, height 178 cm, BMI 20) with a histological diagnosis of pancreatic-cancer. The patient was married, retired for 9 yrs, and physically active. Since his retirement, he took part in several multi-stage treks, such as Monti Liguri mountain way route (400 km) and Via Alpina mountain way route (>1,300 km), and 12-, 24-, 36-, and 48- hour non-stop ultra-endurance walking events. In 2013, he undertook one 36-hour non-stop ultra-endurance walking in March (Catania, Sicily), and two 48-hour non-stop ultra-endurance walking events in May and June (Affi, Veneto, and Barrea, Abruzzo, respectively), and the Mons Gibel Tour, a 20-day trekking along Etna’s periplo (Sicily), in July (Table 2).
He was diagnosed with a pancreatic-adenocarcinoma in September 2013 (stage IV; PS 0; 55 mm and 27 mm invasive components in pancreas body; liver involvement with multiple invasive components, 6-month life expectancy). Cancer-diagnosis came when the patient, after a long summer, fully scheduled with periods of consecutive walking events noticed he was not re-gaining weight and experienced a sudden, strong stomach ache (Table 2).The patient did not have history of pancreatitis, diabetes or any other conditions involving pancreas. At the diagnosis, the cancer was not resectable and the treatment involved adjuvant-chemotherapy, which commenced one week after the diagnosis. Each chemotherapy cycle included seventeen days of therapy, which was administered in a series of nine cycles (Table 2). On the first day of each cycle, the patient received a dose of Epirubicine, 62 mg, and Cisplatinum, 76 mg, given by intra-arterial infusion. On the second day, the patient received a dose of Gemcitabine, 1,800 mg, given by intravenous infusion. From the third day and for the consecutive 14 days the patient took Capecitabine per os, two pills of 500 mg, twice a day. Due to low platelet-count the treatment plan was modified from cycle five as detailed in (Table 2).
Control-subjects: Two men without cancer were monitored to provide a control-comparator for the inflammatory-response to prolonged-exercise. One control-subject was a 55-yr old man (Ctrl 1, mass 89.8 kg, height 180 cm, BMI 28) and the other control-subject was a 41-yr old man (Ctrl 2, mass 69.0 kg, height 173 cm, BMI 23). Both the control-subjects were healthy, physically active, and experienced in this kind of ultra-endurance walking events. Despite of the difference in age and BMI, these subjects were chosen, because their experience in non-stop ultra-endurance walking is quite similar to the experience of our main subject. All procedures were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments. Informed consent was obtained from all individual participants included in the study.
24 hr non-stop ultra-endurance walking
Chemo: 24 hr walk completed during chemotherapy for the treatment of pancreatic cancer occurred on 4th and 5th March 2014 (Cogorno, Italy). 24 hr walk occurred twenty days after the sixth chemotherapy cycle, when the patient did not take neither Gemcitabine nor Capecitabine (Table 2).
No chemo: In order to make the study as much complete as possible we evaluated further inflammation, hepatic, and pancreatic functionality data of the pancreatic-cancer patient during a comparator event prior to cancer-diagnosis and treatment. The data were collected during a previous 24 hr walk in March 2013 (Catania, Italy). Clearly this comparison is limited by the fact that the events occurred 1 year apart. However, the similarity of the prolonged-exercise condition conducted before and after pancreatic-cancer diagnosis and treatment provides a highly valuable comparator condition for this case study.
Controls: Ctrl 1 was monitored during a 24 hr walk in January 2014 (Verona, Italy). Ctrl 2 was monitored during a 24 hr walk in March 2013 (Catania, Italy).
Home-based walk training
The patient did not stop to perform his habitual physical activity (PA) after the cancer-diagnosis. A GPS-receiver (Dakota 20, Garmin, Olathe, USA) was used to monitor his training-program prior to 24 hr walk. The average speed (km/h) and total distance walked (km) was tracked for all walks performed. There was no prescribed exerciseschedule, the participant just completed his habitual walking-activity. He had been walking at least once a week for some hours (depending on both his perceived physical effort and the weather conditions) prior to the cancer-diagnosis. Additionally, white blood cells, platelets (PLT), and hemoglobin concentration were measured immediately before, and 10 days after, the initiation of each chemotherapy cycle (Table 2).
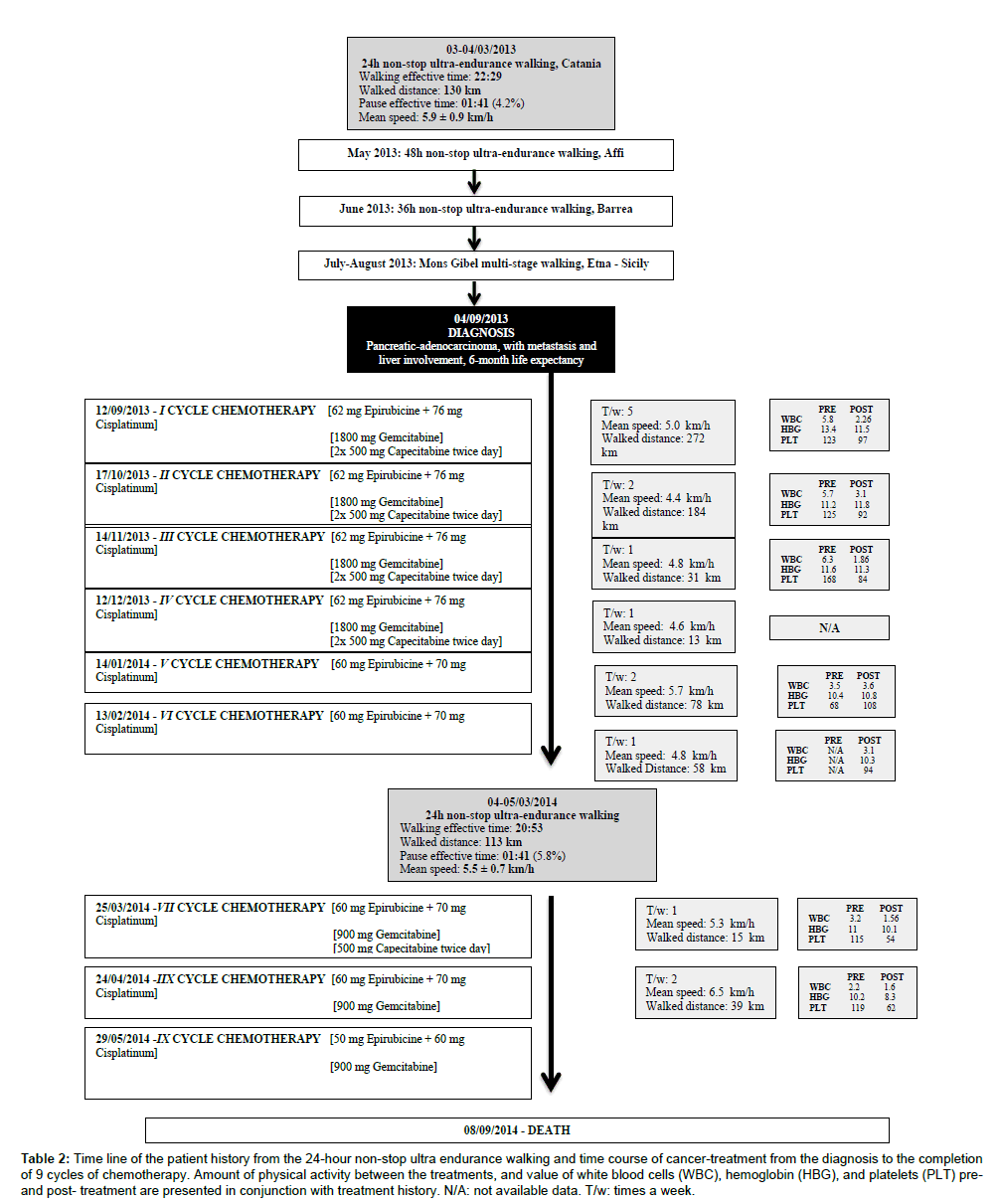
Table 2: Time line of the patient history from the 24-hour non-stop ultra endurance walking and time course of cancer-treatment from the diagnosis to the completion of 9 cycles of chemotherapy. Amount of physical activity between the treatments, and value of white blood cells (WBC), hemoglobin (HBG), and platelets (PLT) preand post- treatment are presented in conjunction with treatment history. N/A: not available data. T/w: times a week.
Data collection and analysis
The data collection and analyses technique was consistent across all prolonged-exercise events evaluated in this study. All the assessments were conducted one hour before the event start and every 6 hours ( ± 30 minutes) during the event. Total distance walked (km) and walking speed (km/h) were monitored throughout the entire event using a GPS-receiver (Dakota 20, Garmin, Olathe, USA).
Blood-samples (20 ml) drawn from the median anterobrachial vein were collected as each assessment and immediately transported to the laboratory for analysis. The plasma-samples were separated with standard centrifugation, according to manufacturer’s instructions (i.e., 1,300 g for 15 min, at room temperature). The plasma of Ctrl 2 subject was collected in Catania and sent later to the analysis laboratory of Verona to be processed together with the other samples by the same person. Concentration of IL-1β, IL-1ra, IL-6, IL-8, IL-10, MCP-1, and TNF-α were determined by means of the commercially available MILLIPLEX multi-analyte panel (Merck Millipore, Darmstadt, Germany) following the manufacturer’s recommendation. CRP was measured on a Cobas c501 (Roche Diagnostics GmbH, Mannheim, Germany), using proprietary reagents. As the patient had pancreaticmetastasis with liver involvement, pancreatic and hepatic functionality were measured in addition to the inflammatory markers. Specifically alanine aminotransferase (ALT), pancreatic amylase (AmylP), and albumin were measured on a Cobas c501.
Statistical Analyses
Pearson’s correlation analysis has been performed in order to reveal the direction and level of significance of the observed results. Statistical analysis was performed with SPSS version 21 for Windows 8.1.
Home-based walk training
No adverse events occurred during any of the training walks. Since the diagnosis, the subject completed 61 walks in a period of 8 months. In this period, he covered a total distance of 701 km. At the beginning of chemotherapy, he walked almost every day. As treatment progressed there were months during which he walked less than once a week (Table 2). Reasons for avoiding walks were chemotherapy-related side effects such as fatigue or a poor PLT level, and/or bad weather condition.
Chemo
No adverse events occurred during Chemo. Reasons for breaks included metabolic measurements, glycaemia and ketones tests, food intake, and toilet breaks. He walked a total of 113 km (Table 2).
No Chemo
No adverse events occurred during No Chemo. He walked a total of 123 km. Reasons for breaks included metabolic measurements, food intake, and toilet breaks.
Control
Ctrl 1 covered 107 km and Ctrl 2 covered 150 km.
Inflammation, pancreatic, and hepatic functionality markers
The inflammatory-response during the prolonged-exercise events is presented in Table 3, Figures 1 and 2. IL-1β (Figure 1, panel B) and TNF-α remained stable throughout 24 hr walk in No Chemo. Concentrations of these two markers at baseline and throughout the whole walk were higher in No Chemo. In comparison, in Ctrl 1 and Ctrl 2 IL-1β remained stable, while TNF-α tended to decrease with the time by ~1.7 fold. IL-1ra tended to decrease slightly over the time for No Chemo, meanwhile it increased in Chemo by 2.3 fold, and in Ctrl 1 and Ctrl 2 by ~18.4 fold. Starting from different baseline values, IL-6 increased in all the subjects: by 6.7 fold in No Chemo, by 7.7 fold in Chemo, and by ~26.6 fold in Ctrl 1 and Ctrl 2. IL-8 increased in all subjects: by 1.7 fold in No Chemo, by 0.2 fold in Chemo, and by ~1.6 fold in Ctrl 1 and Ctrl 2. IL-10 increased only in No Chemo and Chemo, in both cases by 2 fold. Differently from No Chemo and Chemo, in Ctrl 1 and Ctrl 2 IL-10 did not increase over the time (Figure 1, panel A). MCP-1 increased until the 18th hour, and then it decreased slightly in all the subjects. CRP increased in all the subjects: by 6.6 fold in No Chemo, by 4.2 fold in Chemo, and by ~21.5 fold in Ctrl 1 and Ctrl 2.
| Basal | Peak | Mean (SD) | Basal | Peak | Mean (SD) | Basal | Peak | Mean (SD) | Basal | Peak | Mean (SD) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IL-1p pg/ml | 3.5 | 4.4 | 3.8 ± 0.4 | NSC | 2.9 | 2.9 | 2.9 ± 0 | sc | 2.9 | 2.9 | 2.9 ± 0 | nsc | 2.9 | 2.9 | 2.9 ± 0 | sc |
| IL-lra pg/ml | 25.8 | 28.6 | 26.9 ± 2.4 | ↓NSC | 18.9 | 28.6 | 19.8 ± 5.8 | sc | 4.9 | 142.2 | 102.1 ± 56 | ↑nsc | 4.9 | 7.3 | 4.5 ± 1.9 | ↑.71-0.47.3 4.5±1.9(.40) |
| IL-6 pg/ml | 7.2 | 40.5 | 22.3 ± 12.4 | ↑ .75 (.14) | 5.3 | 36.4 | 22.1 ± 12.9 | ↑.96(.01) | 1.24 | 25.2 | 12.5 ± 10.4 | ↑nsc | 1.2 | 45 | 20.5 ± 15.9 | ↑nsc |
| IL-8 pg/ml | 14.7 | 24.3 | 18.9 ± 3.4 | ↑.89 (.04) | 22.9 | 30.7 | 26.2 ± 4.7 | ↑.79(.12) | 10.4 | 10.4 | 4.2 ± 3.4 | ↓nsc | 10.3 | 16 | 12.7 ± 2.6 | ↓sc |
| IL-10 pg/ml | 10.9 | 20.9 | 14.6 ± 4.0 | ↑.89 (.04) | 4.2 | 7.7 | 5.8 ± 1.8 | ↑.85 (.06) | 3.1 | 5.2 | 3.4 ± 0.9 | ↑nsc | 3.0 | 3.0 | 3.0 ± 0.0 | =nsc |
| TNF -a pg/ml | 10.2 | 10.9 | 10.4 ± 0.4 | SC | 6.47 | 8.8 | 7.3 ± 1.0 | = .85 (.06) | 21.8 | 21.8 | 12.7 ± 5.1 | ↓nsc | 21.8 | 21.8 | 18.6 ± 2.3 | ↓.89 (.45) |
| MCP-1 pg/ml | 1565 | 3433 | 2441 ± 715 | SC | 1848 | 2324 | 2111 ± 200 | ↑.83 (.07) | 1280 | 2668 | 1840 ± 636 | ↑nsc | 1280 | 2483 | 1745 ± 576 | ↑ nsc |
| Albumin pg/ml | 39.7 | 40.6 | 38.8 ± 0.6 | SC | 1741.2 | 41.2 | 38.8 ± 1.2 | = SC | 47.3 | 50.2 | 47.8 ± 1.5 | ↑.94 (.09) | 47.3 | 48.0 | 46.4 ± 1.6 | ↑.91 (.47) |
| ALT UIL | 4 | 5 | 3.8 ± 0.8 | SC | 6 | 6 | 4.8 ± 0.8 | = -.75(.14) | 16 | 10.4 ± 5.8 | ↑nsc | 9 | 6.8 ± 3.3 | ↑NSC | ||
| AmiiP UIL | 17 | 17 | 15.6 ± 1.1 | =.95(.01) | 10 | 10 | 8.6 ± 1.1 | =- .83 (.08) | 195 | 195 | 61 ± 74.9 | ↓nsc | 195 | 195 | 100.8 ± 62.7 | ↓NSC |
| CRP mg/L | 36 | 21.8 | 8.38 ± 7.84 | ↑.85 (.06) | 3.4 | 13.1 | 6.5 ± 4.2 | =- .83 (.08) | 1.2 | 23.3 | 7.4 ± 9.3 | sc | 1.2 | 28.3 | 10.4 ± 11.8 | ↓NSC |
Table 3: Cytokines, hepatic and pancreatic function markers variation.
Albumin remained stable in all subjects during the whole walk. We have to point out that albumin in both No Chemo and Chemo was lower than in Ctrl 1 and Ctrl 2. Although starting from different baseline values, ALT remained stable in No Chemo and Chemo, while increased by ~12 fold in Ctrl 1 and Ctrl 2 (Figure 2, panel A).. Furthermore, starting from different baseline values, AmylP remained stable in both No Chemo and Chemo, while decreased by ~5.2 fold in Ctrl 1 and Ctrl 2 (Figure 2, panel B)
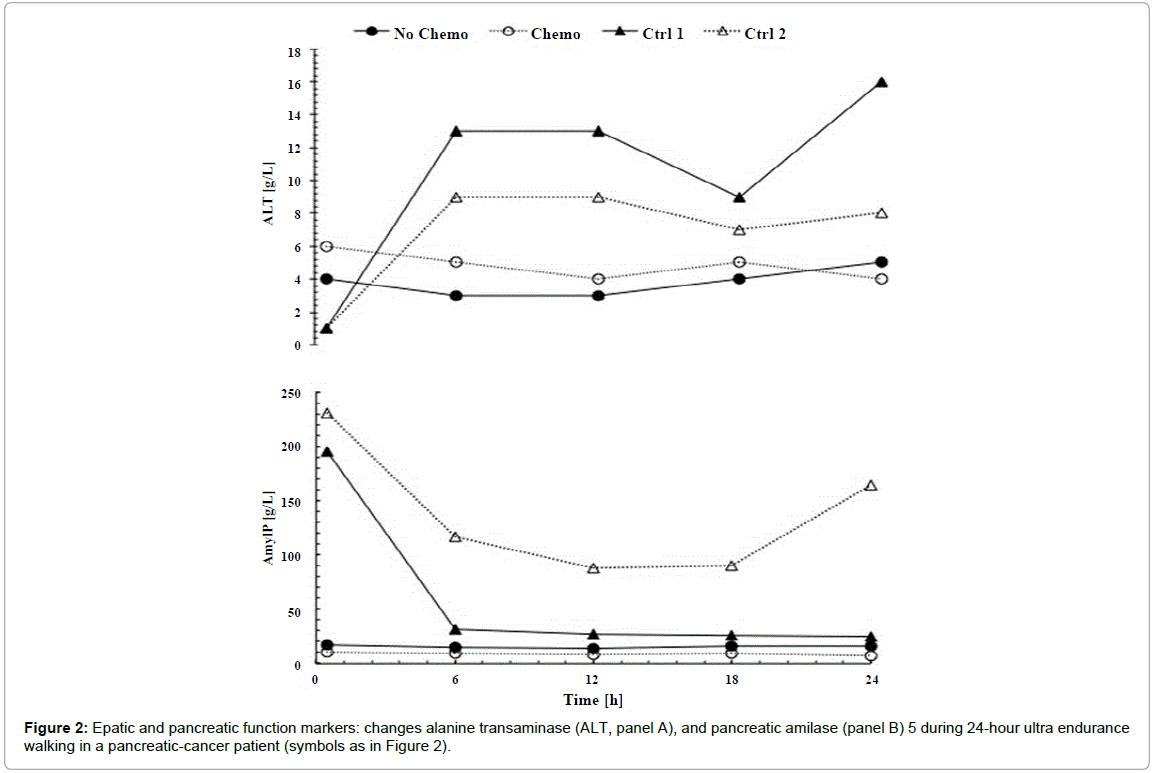
Figure 2: Epatic and pancreatic function markers: changes alanine transaminase (ALT, panel A), and pancreatic amilase (panel B) 5 during 24-hour ultra endurance walking in a pancreatic-cancer patient (symbols as in Figure 2).
In this control-supported case study, we report novel findings regarding the inflammatory-response, pancreatic, and hepatic functionality during prolonged-exercise in a pancreatic-cancer patient prior to cancer-diagnosis and after diagnosis during chemotherapy. Additionally, we compared the inflammatory-response of the pancreatic-cancer patient with two healthy control-subjects (with pooled-data from two different events). To our knowledge, there are no previous evaluations of the inflammatory-response monitored during an exercise in a pancreatic-cancer patient undergoing treatments that impact systemic inflammation. The majority of studies investigating the impact of ultra-endurance exercise on biochemical variables have focused mainly on experienced healthy-athlete [9-11,16-21].
Through the monitoring of self-administered training conducted by the patient following the cancer-diagnosis, there is evidence that long-distance walk training was relatively well tolerated. It is clear that the development of pancreatic-cancer and the resulting administration of chemotherapy influenced the quantity (times/week) and quality (covered distance) of training achievable (Table 2). Our observation is confirmed by recent evidence suggesting that cancer-type, disease stage, and treatments may moderate the exercise-response [3]. Therefore, considering the influence of chemotherapy on exerciseresponse becomes necessary for professionals when planning exercise intervention for cancer-patients.
Many baseline inflammatory, hepatic, and pancreatic functionality markers did not differ considerably between No Chemo, Chemo, and Ctrl 1 and Ctrl 2. However, the inflammatory-response, hepatic, and pancreatic functionality throughout 24 hr walk were, for the most part, not considerably exacerbated by concurrent chemotherapy in a pancreatic-cancer patient (Table 3). There were some differences in the response of various variables throughout 24 hr walk highlighting the impact of chemotherapy on the systemic inflammatory-response of our subject [16]. This is supported by the fact that the inflammation response of Chemo was more similar to Ctrl 1 and Ctrl 2 than to No Chemo (Figure 1), but also because cytokines were much lower in Chemo than in No Chemo (Table 3). This is hypothesized to be due to the anti-angiogenesis effect of chemotherapy [22].

Figure 1:Inflammation markers: changes in interleukin 10 (IL-10, panel A); interleukin 1β (IL-1 β, panel B), 1 during 24-hour ultraendurance walking in a pancreaticcancer
patient (No Chemo, ●), the same patient undergoing chemotherapy (Chemo, ○), and two control-subjects (Ctrl 1, ▲; and Ctrl 2, Δ).
While there are no previous studies focused on the inflammatoryresponse in pancreatic-cancer during exercise or prolonged-exercise to compare our results with, these observations are partially confirmed by several studies focused on healthy-subjects. A study investigated 9 well-trained male endurance-athletes during a 24-hour ultraendurance exercise bout (including running, cycling, and kayaking) [19]. In these athletes IL-1β and TNF-α did not change, but IL-6, IL-8, and CRP increased significantly between pre- and post-exercise [19]. Furthermore, another study considered blood-samples from 15 male athletes, who finished a 246 km ultra-distance race in less than 36 hours, and observed IL-6 and CRP to dramatically increase after the race [11]. Further researchers investigated a comparable series of cytokines as assessed in the current study in 20 athletes immediately after an Ironman triathlon-competition [20]. No changes were observed in IL-1β and TNF-α while a range of other inflammatory markers had increased significantly at the end of the race (IL-1ra, IL-6, IL-8, IL-10, MCP-1, and CRP [20].
In our study the observed pattern of cytokines release during prolonged-exercise in Chemo, and Ctrl 1 and Ctrl 2 might reflect a partial suppression of pro-inflammatory response, rather than an antiinflammatory response. This is highlighted by the non-change of IL- 1β and TNF-α, which would be elevated in the case of an endotoxicresponse [10]. Moreover, IL-6 is most often classified as an antiinflammatory cytokine released during exercise, because it seems to be triggered by muscle-damage, adrenaline, and energy-imbalance [10]. Indeed, IL-6 reacts to the drop in glycogen-storage during conditions of continued metabolic energy demands, as for example during a 24 hr walk [10]. Furthermore, exercise-induced increase in IL-6 is commonly followed by increased concentration of other anti-inflammatory cytokines such as IL-1ra. Exercise-related IL-6 would suppress TNF-α release [23]. Furthermore, the elevation of IL-8, MCP-1 and CRP in our subject may reflect the muscle inflammatory reaction possibly related to muscle degenerative events, rather than a cancer-related proinflammatory reaction [20].
It is well established that several cytokines have different roles in pancreatic-cancer and during prolonged-exercise (Table 1). IL-10 was expected to increase in both No Chemo and Chemo. But we found an increase in IL-10 only in Chemo. This might be due to the different role of this cytokine in different situations. In fact in a cancer-environment, IL-10 would act like anti-apoptotic and tumor-growth factor [24], but during exercise it would act like anti-inflammatory cytokine, increasing the cortisol-level and inhibiting TNF-α. Furthermore, in Chemo IL-1ra level did not increase. The high level of IL-1ra at the baseline in No Chemo would reflect a great inflammation caused by infection, tissue injury, or disease. Meanwhile, trend of IL-1ra in No Chemo at baseline and over 24 hr walk would be explained by the acute-phase protein role of this cytokine in cancer [25]. Consequently, we suppose that during No Chemo the anti-inflammatory response to the exercise was overtaken by pro-inflammatory response to pancreatic-cancer, since it was not yet weakened by chemotherapy.
Albumin is involved in protein-synthesis by the liver. Although No Chemo and Chemo presented very low albumin-level, it remained almost unchanged throughout the duration of 24 hr walk. Even in Ctrl 1 and Ctrl 2, albumin levels did not change significantly during 24 hr walk. ALT (another enzyme involved in hepatobiliary functionality) remained almost unchanged in both No Chemo and Chemo, but increased significantly in Ctrl 1 and Ctrl 2. Our results are partially supported by previous studies. A study investigated biochemical and hematological changes in a 61-yr old healthy man before and after a 120-km swim in open-water [17]. Albumin did not change between pre- and post- swimming, while ALT increased by 4.5 fold. Furthermore another study considered blood-samples of 11 ultra-marathon runners, who ran at least 100 km in 24 hours [21]. Albumin values remained unchanged in both these studies, while ALT increased from 35.1 to 118.4 U/L (3.4 fold) between pre- and post-running. However, although Ctrl 1 and Ctrl 2 ALT increased by 12 fold, its highest level was 12 U/L, a very low value compared with values recorded by a previous study [21]. Consequently, the obtained results lead us to hypothesize that prolonged-exercise such as a 24 hr walk does not provide enough stimulus to significantly stress hepatic functionality in pancreatic-cancer patients or healthy-subjects. Indeed, even if albumin and ALT for the patient were consistently lower than those observed in the control-subjects, these variables were not exacerbated during 24 hr walk. Despite starting from different levels, AmylP (enzyme involved in pancreatic functionality) remained almost unchanged in No Chemo and Chemo, but decreased dramatically in the first 6 hours in Ctrl 1 and Ctrl 2. We hypothesize that the large AmylP at the beginning of the walk in Ctrl 1 and Ctrl 2 was due to the fact that they were not fasting prior to this blood-sample collection-point. However, although AmylP in No Chemo and Chemo was lower than in Ctrl 1 and Ctrl 2, it did not get worse throughout 24 hr walk.
There are several limitations within this study. First of all we have only one pancreatic-cancer patient, who may represent an extreme outlier, so the results could refer mainly to the specific response to exercise of this person and may not be generalizable to other pancreatic-cancer patients. Control-subjects were younger than the pancreatic-cancer patient and they have different BMI, so the inflammation response might be influenced by this difference in age and fat-distribution. Furthermore, we decided to add control-subjects prospectively using data previously collected. Another limitation is that we conducted inflammatory response analysis only in plasma, without considering pro-inflammatory cytokine messenger RNA, which may limit the interpretation of the results. Despite these limitations, this case study provides the first examination of the inflammatory-response of prolonged-exercise in a cancer-patient. While the design is limited to a case study, it is strengthened by comparisons between prolongedexercise events conducted prior to and during chemotherapy as well as with control-subjects without cancer.
This is the first study focused on the inflammation response to exercise of a pancreatic-cancer patient. Ultra-endurance non-stop walking was associated with a change in inflammatory-response in a pancreatic-cancer patient chemotherapy-free and with chemotherapy, as well as in healthy-subjects. Nevertheless, even if an ultra-endurance non-stop event was characterized by a moderate intensity, this was not enough to trigger a pro-inflammation response when the pancreatic cancer patient was with chemotherapy. In addition, although the cancer had already compromised the pancreatic and hepatic functionalities of the pancreatic cancer patient, prolonged exercise was not so intense stimulus to significantly exacerbate systemic inflammation. Therefore, our results highlight the possibility for pancreatic cancer patients undergoing chemotherapy to make moderate exercise, even for prolonged time, without encountering negative side effects and without triggering a pro-inflammatory response. Further studies are needed in order to understand the mechanism of inflammation response to regular exercise in cancer patients undergoing chemotherapy.
Written informed consent was obtained from the patient’s wife and from both control subjects for publication of this case report. A copy of the written consent is available for review by Editor of this journal.
This manuscript is dedicated to the memory of the subject, M. S., who, in the meanwhile, has passed away due to his disease. M. S. will remain forever an example of active person and keen collaborator in many research projects.