Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
Research Article - (2015) Volume 4, Issue 2
Introduction: The clinically manifested hypothyroidism is associated with systolic and diastolic dysfunction. Studies investigating the left ventricular function in subclinical hypothyroidism (ScH) have shown controversial results. The aim of the study was to assess whether ScH is associated with the left ventricular systolic and diastolic dysfunction.
Material and methods: Seventeen consecutive patients with newly diagnosed ScH and 20 healthy euthyroid patients as controls were analyzed. The two groups were appropriate by: age, sex, and body mass index. Laboratory analyses were performed in all patients - determination of TSH, free thyroxin (FT4), free triijodothyronine (FT3), antibodies directed to thyroid peroxidase (TPOAb) and antitiroglobulin antibodies (TgAb), and the assessment of left ventricular systolic and diastolic function by M-mode, two-dimensional echocardiography, pulse, continuous and color-Doppler, advanced echocardiographic modalities Tissue Doppler (TDI) and two-dimensional speckle tracking.
Results: ScH patients had statistically significant lower ejection fraction, smaller ratio s/d (where s is the systolic velocity and d is the diastolic velocity through the pulmonary veins) and lower negative longitudinal global strain compared with the control group (62.1 ± 2.1 vs. 58.7 ± 6.2%, p<0.05, 1.27 ± 0.12 vs. 1.06 ± 0.20, p<0.001, -0.21 ± 0.01 versus -0.19 ± 0.01%, p<0.05, respectively). There was a statistically significant negative correlation of TSH with s/d and S/ TDI (r = 0.43 and r = 0.26, p<0.05, respectively). There was a statistically significant negative correlation of free thyroxine with myocardial performance index (r = -0.17, p<0.05), and a positive correlatin with s/d (r =0.48, p<0.05).
Conclusion: ScH was associated
Subclinical hypothyroidism (ScH) is a common endocrine disorder characterized by elevated serum TSH hormone with normal serum FT4 and FT3. Prevalence of ScH in adults is 1-10%, and in women over 60 years above 20% [1,2]. Positive thyroid antibodies increase the risk of progression to clinically manifest hypothyroidism [3]. Thyroid hormones have influence on the heart. Heart is sensitive to small continuous changes of serum thyroid concentrations in blood [3]. It is known that clinically manifest hypothyroidism is associated with systolic and diastolic left ventricular disfunction [1]. However, studies investigating the systolic and diastolic function of the heart in ScH showed controversial results. Some studies demonstrate mild diastolic dysfunction in patients with ScH [4-9], but not in others [10-13]. Diastolic dysfunction increases morbidity, leading to no effort tolerance and occurrence of heart failure.
New echocardiographic techniques for evaluating cardiac function are available. Today Tissue Doppler Imaging (TDI) echocardiography is a new and powerful method for evaluation of the regional and global systolic and diastolic ventricular function. It is considered superior to standard echocardiography because it eliminates the impact of hemodynamic parameters [14]. Standard echocardiography and TDI have limited opportunities in the early stages of heart failure. For this purpose we can use a new, non-invasive technique that assesses left ventricular mechanics by measuring longitudinal global strain (GLS). It shows the longitudinal deformation of the myocardium and is considered a more sensitive parameter for the assessment of left ventricular function [15].
The aim of the study was to evaluate the left ventricular systolic and diastolic function in ScH using M-mode, two-dimensional echocardiography, pulse, continuous and color-Doppler, and advanced echocardiography modalities Tissue Doppler and two-dimensional speckle tracking.
Patients
The cross-section study was conducted at the University Clinic of Endocrinology, Diabetes and Metabolic Disorders in Skopje, R. Macedonia. The study included the observation of two patient groups: control and ScH group. ScH group consisted of 17 consecutive patients with newly diagnosed ScH. The criteria for the diagnosis of ScH were: TSH>4.2 mU / L with normal serum FT4 10.3-24.45 pmol / L and FT3 4.2-8, 1 pmol/L. The control group consisted of 20 healthy, euthyroid persons with normal FT4, FT3 and TSH (0.2-4.2 mU / L). Both groups were appropriate for: age, sex and body mass index (BMI).
Exclusion criteria: The study did not include patients with a history of thyroid disease, condition after subacute thyroiditis, cardiovascular diseases, hypertension, and cigarette smokers or those taking drugs that affect the thyroid metabolism and heart rate. Patients with hypothalamic-pituitary disease, depressive psychosis, bipolar disorders, diabetes, chronic pancreatitis, hepatic, renal disease, ovulatory dysfunction, infertility, and pregnancy were also not included.
Ethical aspects: All patients gave informed consent to participate in the study after careful explanation of the testing protocol. The study was in accordance with the Declaration of Helsinki and approved by the Ethics Committee at the Medical Faculty in Skopje.
Methods
At the first visit the following laboratory analyses were done in all patients: TSH, FT4, FT3, TPOAb, and TgAb. By using M-mode, 2D, Doppler and Pulse Wave Tissue Doppler Imaging (PW TDI) echocardiography the left ventricular systolic and diastolic function were assessed.
Laboratory tests: Blood from the antecubital vein after 09.00 am was taken. TSH, FT4 and FT3 were determined by super-sensitive chemiluminescent immunoassay (Immulite 2000, Siemens Medical Solutions Diagnostics, Los Angeles, CA, USA). The functional sensitivity for TSH was 0.004 μIU/mL, for FT4, 0.3 ng/dL and FT3 0.4 ng/dL. TPOAb and TgAb were determined by imunometric assay (ECLIA-Roche Elecsys 2010, Hitachi, Switzerland), and they were considered positive if values were above 34 IU/mL and above 113 IU/L, respectively.
Echocardiographic measurements: Echocardiographic examination was performed by using a Vivid 7 ultrasound machine of General electronics at the University Clinic of Cardiology. The analyses of the parameters were made with off-line analysis of the memory image at the work station. To obtain certain parameters all echocardiographic modalities were used: M-mode, two-dimensional (2D) echocardiography, pulsed, continuous and color-Doppler, and advanced echocardiographic modalities Tissue Doppler and two-dimensional speckle tracking. Conventional long and short axis, apical 2, 3, and 4-chamber view were used, according to the recommendations of the American Society of Echocardiography (ASE) [16].
Using 2D long axis, in M-mode echocardiography according to the recommendations of ASE, the following parameters were measured: the LV end-systolic (LVESD) and end-diastolic diameters (LVEDD), the left ventricular posterior wall (PW), interventricular septum thickness (IVS), left atrial diastolic diameter (LA), and derived indexfractional shortening (FS).
The assessment of global LV systolic function was determined by using the “Biplane” disc method (the modified rule of “Simpson”). This method is also recommended by the ASE [15]. Ventricular volumes were calculated in two apical windows (apical 4-chamber and apical 2-chamber view) at end-diastole and end-systole. Then, using computer software, the following were determined: LV end-systolic (LVESV) and end-diastolic (LVEDV) volumes, ejection fraction (EF), and the area of the left atrium (LA area).
Transmitral Doppler inflow and tissue-pulsed Doppler (TDI) were obtained in the apical 4-chamber view. The following parameters were measured: transmitral early diastolic peak flow velocity (E), late diastolic flow velocity (A), their ratio (E/A), E velocity deceleration time (DT), and the duration of the atrial contraction (A dur). Guided by 2D 4-chamber view, a 5 mm sample volume was placed from the site of the septal and lateral insertion of the mitral cusps, using TDI. In order to minimize artifacts minimal intensity (gain) Doppler and low wall filter were used. Thus the angle between the ultrasound wave and the analyzed myocardial segment was not greater than 30°. We measured the maximum systolic velocity (S), peak early diastolic velocity (e’), and peak atrial diastolic velocity (a’). Using E and e’ parameters, the following derivate parameters which showed LV diastolic function were calculated: ratio E/e’ lat., where e’ lat. was the speed of early diastolic myocardial relaxation measured lateral, E/e’ sep., where e’ sep. was the speed of early diastolic relaxation measured septal, E/e’ average, where e’ average was the average value of e ‘lat. and e’ sep., isovolumetric contraction time (IVCT), isovolumetric relaxation time (IVRT), and ejection time (ET). All parameters were determined as the average of measurements in three heart cycles. Myocardial performance index or Tei index (MPI) was calculated by the formula Tei index = IVCT + IVRT / ET.
The flow through the pulmonary veins (PV) was determined in the apical 4-chamber view using color flow Doppler. The following parameters were determined: systolic velocity through the pulmonary veins (s), diastolic velocity through the pulmonary veins (d), their ratio (s/d), and retrograde pulmonary venous flow during the atrial contraction-atrial reversal (Ar).
Speckle tracking dimensional echocardiographic technique is advanced, independent of the angle of measurement, compared with other echocardiographic parameters. Speckle tracking modality is integrated in the new echocardiographic systems for fast automatic assessment of ventricular function. For getting this parameter three apical sections 2, 3, and 4-chamber view were used, labelling endocardium and automatic assessment global deformation of LV was obtained.
The values of EF, FS and S from TDI give us information about the global systolic function, global strain gives us information about the longitudinal LV function, and parameters of mitral and pulmonary veins flow from TDI gave us information about the diastolic function. Myocardial perfusion index is a parameter that provides information about global, systolic and diastolic function.
Statistical analysis
Statistical analysis was performed using Statistics Package 7.0 for Windows program. Data are presented as the average ± standard deviation or percentages. Independent t-test was used for the comparison of quantitative data between the two groups. For the comparison of categorical variables the chi-square test, Yates correction was used. The correlation between the tested parameters was determined using Pearson correlation. p<0.05 was taken as statistically significant.
The main demographic and hormonal parameters of all patients are presented in (Table 1). In both groups there was no difference in age, sex, and body mass index. As expected, the two groups differed statistically significantly in the value of TSH (p<<0.001). But ScH patients had statistically significant lower values of FT4 and FT3 (p<0.001 and p<0.05, respectively). Also, patients with ScH had a statistically significant higher incidence of positive TPOAb and TgAb.
| Control group (20) | ScH group (17) | pvalue | |
|---|---|---|---|
| Age (years) | 39,1 ± 10,4 | 41,1 ± 8,2 | 0,53 |
| Sex (m:f) | 3:17 (30%) | 2:15 (11,8%) | 0,58 |
| BMI (kg/m2) | 24,3 ± 3,6 | 26,6 ± 3,4 | 0,06 |
| TSH (mU/L) | 2,9 ± 0,9 | 8,2 ± 1,9 | <0,001 |
| FT4 (pmol/L) | 15,3 ± 2,1 | 11,7 ± 1,6 | <0,001 |
| FT3 (pmol/L) | 6,1 ± 2,9 | 4,2 ± 0,7 | <0,05 |
| TPOAb | 3/20 (15%) | 13/17 (76,5%) | <0,001 |
| TgAb | 2/10 (20%) | 10/13 (76,9%) | <0,05 |
Table 1: Demographic and hormonal characteristics of the analyzed parameters (Presented data are mean ± SD and percentage).
Left ventricular measurements and volumes were normal between the two groups (Table 2), but left ventricular EF was statistically significantly lower (p<0.05) in ScH group. The ratio between E/A was lower and DT longer in patients with ScH, but the differences were not statistically significant. MPI was also higher in patients with ScH, but without statistical significance. The ratio s/d was statistically significantly lower in patients with ScH (p<0.001, Table 2). The left ventricular longitudinal global strain was statistically significantly lower in patients with ScH (p<0.05, Table 2). There was a statistically significant negative correlation of TSH with s/d and s/TDI (r = -0.43 r = -0.26, p<0.05) (Figures 1 and 2). There was a statistically significant negative correlation of free thyroxine with MPI (r = -0.17, p<0.05) (Figure 3) and a positive correlation with s/d (r = 0.48, p<0.05) (Figure 4).
| Control group (20) | ScHgroup (17) | p value | |
|---|---|---|---|
| LA(mm) | 32,2 ± 2,7 | 30,2 ± 7,2 | 0,25 |
| LVEDD (mm) | 46,0 ± 4,5 | 44,2 ± 8,8 | 0,42 |
| LVEDvol (ml) | 79,2 ± 12,3 | 77,0 ± 13,5 | 0,60 |
| LVESvol (ml) | 32,3 ± 6,9 | 32,4 ± 5,3 | 0,95 |
| EF (%) | 62,1 ± 2,1 | 58,7 ± 6,2 | <0,05 |
| FS (%) | 34,2 ± 2,5 | 32,6 ± 3,5 | 0,11 |
| IVS (mm) | 10,5 ± 0,9 | 10,7 ± 1,0 | 0,51 |
| PW (mm) | 8,6 ± 0,9 | 8,4 ± 1,1 | 0,60 |
| E/A (m/sec) | 1,21 ± 0,4 | 1,06 ± 0,3 | 0,22 |
| DT (msec) | 159,3 ± 32,6 | 162,5 ± 35,2 | 0,77 |
| E/e' sep (sm/s) | 5,9 ± 1,5 | 6,4 ± 2,2 | 0,55 |
| E/e' lat (sm/s) | 6,1 ± 1,1 | 6,2 ± 1,2 | 0,78 |
| E/e’ average (sm/s) | 6,0 ± 1,3 | 6,3 ± 2,0 | 0,43 |
| Ar (ms) | 101,5 ± 13,1 | 94,5 ± 14,1 | 0,12 |
| IVCT (msec) | 61,5 ± 10,3 | 61,2 ± 14,4 | 0,95 |
| IVRT (msec) | 68,5 ± 7,9 | 66,0 ± 12,5 | 0,46 |
| MPI | 0,45 ± 0,07 | 0,48 ± 0,04 | 0,18 |
| s/d | 1,27 ± 0,12 | 1,06 ± 0,20 | <0,001 |
| global strain (%) | -0,21 ± 0,01 | -0,19 ± 0,01 | <0,05 |
| s/TDI (m/sec) | 0,08 ± 0,02 | 0,08 ± 0,01 | 0,81 |
Table 2: Structural and functional echocardiographic parameters of the left ventricle in both groups (Presented data are mean ± SD).
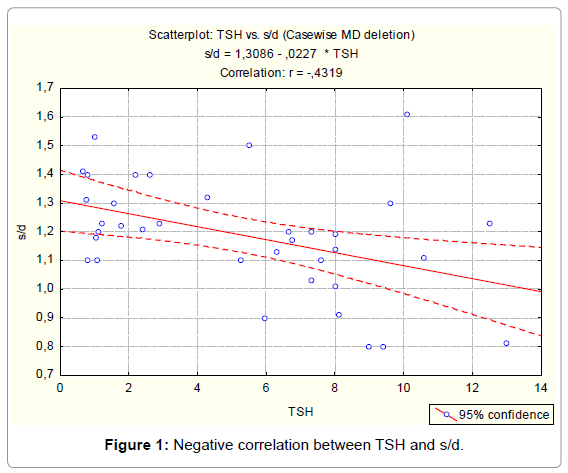
Figure 1: Negative correlation between TSH and s/d.
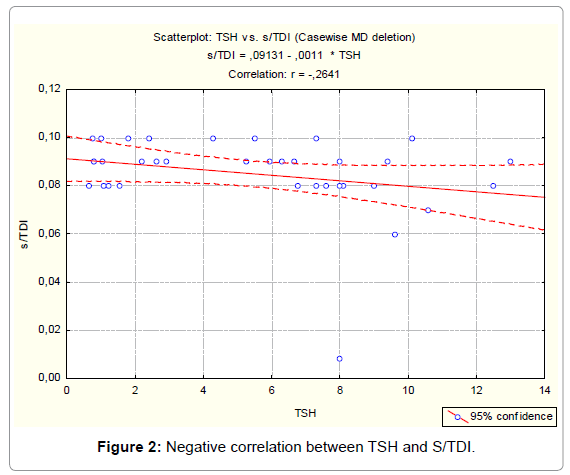
Figure 2: Negative correlation between TSH and S/TDI.
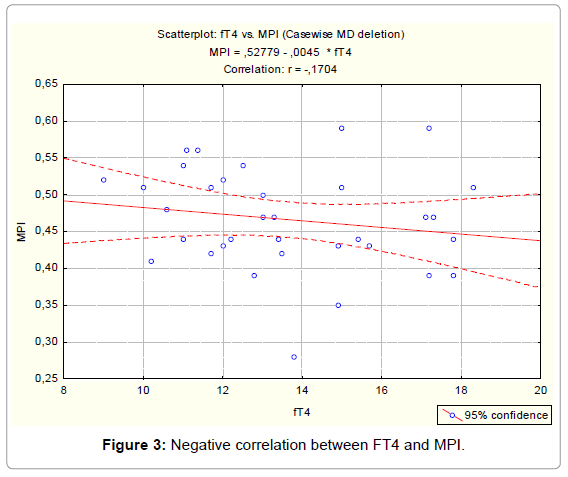
Figure 3: Negative correlation between FT4 and MPI.
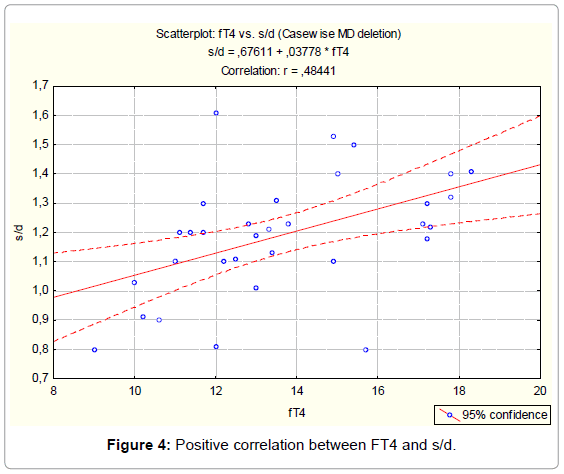
Figure 4: Positive correlation between FT4 and s/d.
Several studies compared left ventricular echocardiography parameters between patients with ScH and a control group. Biondi et al. [5] showed no differences, but Monzani et al. [6] showed left ventricular diastolic dysfunction in patients with ScH (prolonged IVRT, lower ratio E/A). Vitale et al. [7] using TDI showed diastolic dysfunction in patients with ScH. The parameters which present diastolic dysfunction in our study were not different, except for the ratio s/d which was statistically significantly lower in patients with ScH. The ratio s/d estimated by pulse Doppler represents diastolic function. Most of the flow through the pulmonary veins in the left atrium takes place during ventricular systole (s wave) and the smaller component in diastole (d wave), so s ≥ d, and ratio s/d ≥ 1. d are influenced by changes in the left ventricular filling and compliance. By reducing compliance and increasing the pressure of the atrium, s decreases, and d increases, so the ratio s/ d<1 [16]. Recent meta-analysis [17] involving 675 patients with ScH, younger than 60 years, versus a healthy control group, appropriate for age and sex, showed a statistically significant left ventricular diastolic dysfunction. In this study, the parameters E/A, DT, IVRT, E/e’ sep., E/e ‘ lat., and E/e ‘ average were not different between the two groups. The absence of statistically significant differences in parameters of diastolic function may be due to mild diastolic dysfunction which probably exists in ScH, so certain parameters are not sensitive enough to show that. It can also be explained by the small group of patients analyzed and the inclusion of patients with higher TSH values in the control group, which still does not meet the criteria for enrolling to ScH group. The average value of TSH in the control group was 2.9 mU/L, which is higher than the median value 1.4 mU/L found in The Third National Health and Nutrition Examination Survey (NHANES III) (1988-1994; n = 13,344), with 13 344 healthy participants [18]. That study [18] proposed the upper value of 2.5 mU/L for TSH [19].
Global systolic function of the left ventricle is estimated by EF. In this study EF, although normal in both groups, showed statistically significantly lower value in patients with ScH. Ilic et al. [20] showed identical reduction of the EF in patients with ScH. The effect of ScH on the left ventricular systolic function is more controversial. Ripoli et al. [21] showed 4% differences in EF, but without statistical signification. Ilic et al. [20] showed a statistically significant difference in EF, although the difference was smaller, only 2%. In this study, the difference in EF of 3.4% was statistically significant. However, TDI analyses in other studies [13,22,23] showed disruption in LV systolic function in patients with ScH.
Longitudinal global strain assesses global longitudinal systolic ventricular function by measuring the deformation of the myocardium in the longitudinal direction during systole and diastole. It is considered a sensitive parameter of subtle changes in contractility compared to EF. Therefore GLS is considered superior in early detection of myocardial dysfunction. In our study GLS was statistically significantly lower in patients with ScH. Identical as our results, Sunbul et al. [15] found longitudinal myocardial dysfunction in 23 patients with ScH and their improvement after thyroid replacement therapy. Ilic et al. [20] and Tadic et al. [23] also showed a decrease of GLS in patients with ScH.
The statistically significant negative correlation of TSH with s/d and S/TDI directly confirms the relationship of TSH with the left ventricular diastolic function. In both groups MPI was high, higher in the ScH group, but without statistically significant difference. There was a statistically significant negative correlation of FT4 with MPI in the group with ScH. MPI is a parameter that evaluates both systolic and diastolic function. Despite the criteria for diagnosis of ScH, patients with ScH compared to control group, had statistically significant lower FT4. The limitation of the study was the small group of analyzed patients, but they were young without cardiovascular risk factors. However, prospective studies with a larger group of patients and follow-up after thyroid replacement therapy are needed to confirm the presence of left ventricular systolic and diastolic dysfunction in ScH.
Subclinical hypothyroidism was associated with a statistically significant reduction in global systolic and global longitudinal systolic function of the left ventricle. The application of the thyroid replacement therapy in ScH is justified and can prevent future cardiovascular disease.