Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 6, Issue 5
Background: Individuals with Multiple Sclerosis (MS) frequently present balance and walking problems; in which reduced trunk stability, often termed core stability, is one essential aspect. A new group-based, individualized core stability training (GroupCoreSIT) is developed and will be evaluated in terms of effects, users’ perceptions, performance and coordination of care. Methods: The study consists of two related parts: 1) a prospective randomized controlled trial (RCT), and 2) a qualitative study. The RCT will be conducted in six municipalities to evaluate the effects of GroupCoreSIT on people with MS compared to standard care. The intervention addresses movement quality in core and balance training highlighting the following elements: dynamic stability, sensory stimulation, specificity, individualization, intensity, and teaching. GroupCoreSIT will be offered three hours per week for 6 weeks, complemented with unsupervised home exercises, with a 6-month follow-up. Seventy-to ambulant people with MS will be included, baseline tested and randomized to intervention and control group. Assessor blinded standardized outcome measurements will be carried at 1-week, 3-month and 6-month post-intervention. The qualitative study will include: i) qualitative interviews conducted twice with 12 participants from each group, at 1-week and 6-month post intervention, aimed to increase the knowledge about short and long-term experiences with GroupCoreSIT and standard care; ii) 12 observations and 12 qualitative interviews with physiotherapists conducting GroupCoreSIT, aimed to identify essential aspects of physiotherapy performance and perceptions related to delivery of intervention; and iii) qualitative interviews conducted twice with 16-20 health professionals in hospital and municipalities, focusing on intensive programs in the coordination of care for people with MS. Conclusion: Evaluation of the efficacy of GroupCoreSIT, participants’ perceptions, physiotherapists’ performance and reflections, and health professionals’ deliberations regarding coordination of intensive programs will provide information for evidence based selection of physiotherapy in ambulatory people with MS.
Keywords: Ambulant people with multiple sclerosis; Physiotherapy; Core stability; Balance; Group-based; Perceptions; Coordination of care
MS: Multiple Sclerosis; PT: Physiotherapist; ADL: Activities for Daily Living (ADL); RCT: Randomized Controlled Trial; NLSH: Nordland Hospital Trust; EDSS: European Disability Status Scale; TIS-modNV: Trunk Impairment Scale- Mod Norwegian version; Mini-BesTEST: Mini Best Evaluation Systems Test; 10MWT: 10 Meter Walk Test; 12MWT: 2 Minute Walk Test; MSWS-12: MS Walking Scale-12; RVGA: Rivermead Visual Gait Assessment; MSIS-29: Multiple Sclerosis Impact Scale–29; MSQOL-54: Multiple Sclerosis Quality of Life–54; PGIC: Patient Global Impression of Change.
People with multiple sclerosis (MS) frequently present balance and walking disturbances [1], even when disability is minimal [2,3]. Dynamic stability of the trunk, commonly termed “core stability”, is one of the fundamental bases for balance and walking [4,5]. Core stability is found to be impaired in individuals with MS [6,7]. Effect of core stability training is limited and restricted to individual approaches [8-10]. Integration of core stability with other essential components of balance is requested [9] as balance is a major risk factor for falls [11,12]. Group-based training is considered motivating [13] and costeffective [14]. Group training is often an integral part of high-int ensity programs in specialist care. High-intensity programs are however rarely offered in municipalities. Group-based high-intensity core stability training is poorly investigated in terms of effects, user experiences and performance, and physiotherapists’ (PT)s’ opportunities for individualization, which is a prevailing principle in rehabilitation of people with MS [15].
A new individualized group-based physiotherapy intervention named GroupCoreSIT (S=stability, sensory stimulation, specificity; I= individualization, intensity; T= training, teaching) was developed to be tested in municipalities. Two preliminary studies on this intervention have been conducted with ambulant individuals with MS, one using a test-retest design [16] and one using Single Subject Experimental Design [17]. These studies provided support for the feasibility of the intervention, preliminary scientific evidence of short-term effect on balance, walking and activities for daily living (ADL) in ambulant individuals with MS and justification for a larger scale clinical trial.
The current GroupCoreSIT study consists of a prospective randomized controlled trial (RCT) and a qualitative study. The study provides several additional elements than traditional core stability approaches. The intervention integrates individualization and group dynamics. Core activation, including all muscles in the trunk and attaching to the trunk [4], is combined with the following principles: optimal alignment of body parts and adaptation to base of support [5,18], coordination of proximal stability and distal movement [4,19], somatosensory stimulation of hands and feet [5,18,20], high-intensity [21], and teaching of self-management [15].
The theoretical framework of the GroupCoreSIT study is movement sciences [18] and neuroplasticity [20] integrated in an extended theoretical framework of phenomenology of the body [22-24] and enactive theories [25-30].
Study design
The GroupCoreSIT study consists of two related parts.
Part I: A prospective RCT will be conducted to evaluate the effects of the GroupCoreSIT on people with MS compared to standard care. The intervention will be offered for a period of 6 weeks, with a 6- month follow-up post-intervention.
Part II: A qualitative study will be conducted through: i) qualitative interviews with patients aimed to increase the knowledge about short and long-term experiences with GroupCoreSIT and standard care, with an endpoint of six months post-intervention, ii) observations and qualitative interviews with PTs aimed to analyze and identify essential aspects of physiotherapy performance and perceptions related to conduction of GroupCoreSIT particularly focusing on individualization, group dynamics and teaching patients selfmanagement in group settings, and iii) qualitative interviews with health personnel in hospital and municipalities focusing on deliberations regarding coordination of intensive physiotherapy in people with MS.
Study participants
To be eligible for enrolment, participants must have the following inclusion criteria: 1) definite diagnosis of MS, according to McDonald's criteria [31], 2) registered at the outpatient clinic at Nordland Hospital Trust, Bodø, Norway (NLSH), 3) living in one of six selected municipalities, 4) aged 18 years or more, 5) capable of providing signed written informed consent, and 6) scoring 1.0-6.5 on the European Disability Status Scale (EDSS) [32]. Exclusion criteria are: 1) pregnancy at enrollment, 2) exacerbation in the 2 weeks prior to enrollment, 3) and acute conditions affecting balance and walking.
Randomization
The participants are randomly assigned to the intervention group or to the control group in a 1:1 ratio (Figure 1). Randomization is performed by a web-based system developed and administered by the Unit of Applied Clinical Research, Institute of Cancer Research and Molecular Medicine, Norwegian University of Science and Technology, Trondheim, Norway. Randomization is stratified according to the EDSS (1.0-3.5 vs. 4.0-6.5). The randomization takes place after the baseline assessment so that the health personnel are blinded to group allocation.
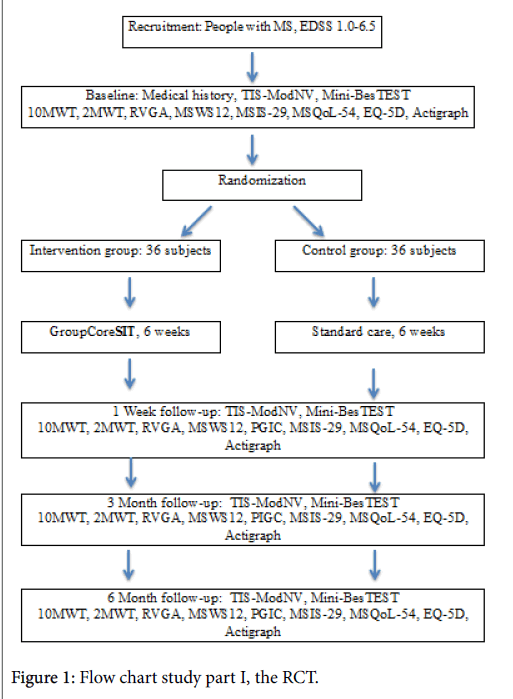
Figure 1: Flow chart study part I, the RCT.
Intervention
Six PTs with expertise in neurological physiotherapy will conduct the intervention in the selected municipalities. They will attend a 4-day practical and theoretical training on the intervention, with 1-2 followup videoconferencing sessions during the study.
After enrollment, and a few days before the group training starts, the PTs responsible to deliver the intervention conduct an individual assessment of each participant as a basis for individualization of the intervention. Each training group consists of three participants. The training sessions last for 60 minutes and will be performed three days per week, for six weeks. The PT instructs, demonstrates and uses hands-on facilitation to enhance performance with optimal quality of movement.
The intervention includes 32 standardized exercises, which will be performed in various postural sets (Table 1). These exercises are organized in five “blocks” according to their objectives, named and described (Tables 2-6). Each exercise includes five levels of difficulty to allow tailoring of the intervention. In the group sessions, all participants do the same exercise simultaneously, but may perform it on various levels.
| Postural Set | Optimal Alignment |
|---|---|
| Prone | Keep both feet in contact with the wall, toes pointing down, and the body and hips in contact with the bench/floor. Keep a straight line between the ankles, knees, hips, trunk, shoulders 90° abducted, elbows and wrist extended, and the palms facing down). You may rotate your neck/head to one side or face down. |
| Supine | Keep both feet in contact with the wall, toes pointing up, and keep the back in contact with the bench/floor. Keep a straight line between the ankles, knees and hips, the back, thorax and neck, and the elbows, hands and fingers extended. |
| Supine with therapy ball under lumbar back/pelvic | Keep both feet on the floor, the back and pelvic on the therapy ball and the thorax, head and arms on the bench. Keep a straight line between the ankles, knees and hips |
| Side lying | Keep a straight line throughout the body, with both feet placed on the wall, hip-width apart. The arms point forward, 90° flexion in the shoulders and the elbows, extension in hands and fingers, while pushing a small ball forward. |
| On all fours | Keep the therapy ball under your stomach, both feet, ankles, knees and hips in a straight line, hip-width apart, toes pointing backwards. Back and head in a straight line. Knees placed straight below the hips, hands placed straight below the shoulders. Extended elbows, hands and fingers. |
| Sitting | Keep an upright position with the trunk and neck, both feet on the floor and a straight line between the ankles, knees and hips. Keep the lumbar back in contact with the therapy ball (the ball placed between your back and the wall behind you). The hands placed beside you on the bench with shoulders external rotated, elbows, hands and fingers extended. |
| Sitting on heals | Keep the bottom as far down towards the heals as you can, toes pointing backwards. Keep a straight line from the lumbar back to the neck. Hands placed on the bench in front of you with elbows, hands and fingers extended. |
| Standing | Keep an upright position with the back, thorax and neck in a straight line and the feet hip-width apart with a straight line between the ankles, knees and hips. Shoulders external rotated, elbows, hands and fingers extended. |
| Standing with the therapy ball behind you | Keep an upright position with the back, thorax and neck in a straight line and the feet hip-width apart. Shoulders external rotated, elbows, hands and fingers extended. Keep the lumbar back in contact with the therapy ball. |
| Standing with the therapy ball in front of you | Keep an upright position with the back, thorax and neck in a straight line and the feet hip-width apart. Hands placed on the wall in front of you with shoulders external rotated and flexed 90°, elbows, hands and fingers extended. Keep the therapy ball between the abdomen and the wall in front of you. |
| ”Bear-standing” | Standing in a flexed position with both feet and hands placed on the floor, hip-/shoulder-width apart. Keep a straight line between the ankles, knees and hips. The elbows, hands and fingers extended. |
Table 1: Descriptions of various postural sets “optimal alignment”.
| Exercise | Objectives | Postural Set | Performance |
|---|---|---|---|
| “The foot” | Core activation while sensory-motor activation of the foot to enhance adaptation to base of support | Sitting in optimal alignment. | Keep the postural set while rolling the mobilization ball in various ways with one foot, for example rolling back and forward |
| “The hand” | Core activation while sensory-motor activation of the hands and fingers to enhance adaptation to base of support | Sitting in optimal alignment. | Keep the postural set while rolling the mobilization ball in various ways with your hands, for example rolling the ball far back and forward with extended arms. |
Table 2: Exercises that aim for core activation simultaneously with sensory-motor activation of the foot or hands to enhance adaptation to base of support. There were five different variations in each exercise (only one example is given here).
| Name | Objectives | Postural Set | Performance |
|---|---|---|---|
| “Bent banana” | Core activation while concentric work in the hip- and knee flexors, and eccentric lengthening of the knee- and hip extensors. | Lying in supine in optimal alignment | Keep the postural set while bending one knee towards the opposite shoulder in various ways, for example while pushing extended arms, hands and fingers towards your toes. |
| “Straight banana” | Core activation while concentric work of hip flexors and knee extensors, and eccentric work in the hip extensors and knee flexors. | Lying in supine in optimal alignment | Keep the postural set while elevating one leg, heal pointing towards the ceiling in various ways, for example followed by moving the elevated leg towards the opposite shoulder and keeping your arms abducted on the bench (90°abduction in the shoulders). |
| “The eagle” | Core activation while concentric hip extensors and knee flexors, and eccentric lengthening of the hip flexors and knee extensors. | Prone-lying in optimal alignment. | Keep the postural set while extending one hip, flexing the knee and pointing one heal towards the ceiling in various ways, for example followed by pushing the heal towards the opposite hip and then towards the ceiling. |
| “Slowly diving” | Core activation while gradually eccentric lengthening of upper trunk and neck extensors. | Sitting or standing with the ball behind you in optimal alignment. | Keep the postural set while flexing the neck/ thorax towards the floor and slowly back to starting position. It might be done in various ways for example towards a psoas box. |
| “Butterfly” | Core activation while concentric work in the trunk and neck extensors and eccentric lengthening of the abdominal, thorax, arms and neck flexors. | Sitting or standing with the ball behind you in optimal alignment. | Keep the postural set while extending arms/thorax backwards in various ways for example by leaning half way back. |
| “Nodding” | Core activation while moving the head and neck, and eccentric lengthening the neck extensors and lateral flexors. | Sitting in optimal alignment. | Keep the postural set while nodding your head in various directions for example towards the other group members. |
| “Pluto” | Core activation while eccentric lengthening the hip, back-and neck extensors. | Sitting on heals in optimal alignment. | Keep the postural set while leaning the trunk, head and arms forward in various ways for example by reaching your hands as far as you can straight forward. |
Table 3: Exercises for optimal adaptation to the base of support and activation of the core while enhancing concentric and eccentric activity in muscles in neck, upper and lower limbs. There are five different variations in each exercise (only one example is given here).
| Name | Objectives | Postural Set | Performance |
|---|---|---|---|
| “Standing on the wall” | Core activation while keeping one or two legs stable and moving the hip into flexion and extension. | Lying in supine in optimal alignment. | Keep the postural set, while extending your arms and pushing them towards the toes. Then for example push the heals towards the wall. |
| “Balancing on the wall” | Core activation while keeping one leg stable and moving the hip into flexion and extension. | Lying in supine in optimal alignment. | Keep the postural set, one foot stable on the wall while extending your arms and pushing them towards the toes. Then for example move the other leg towards the floor, and push the heal towards the floor. |
| “Walking on the wall” | Core activation while keeping one or two legs stable and moving the hip into flexion or extension. | Lying in supine in optimal alignment. | Keep the postural set, two feet on the wall. Extend your arms and push them towards the toes. Then “walk on the wall”. |
| “The spider” | Core activation while keeping both legs stable and moving the pelvis. | Lying in supine in optimal alignment. Keep your hips and knees flexed and the feet placed on the bench or the wall. | Keep the postural set while doing pelvic tilts in various ways for example by keeping hips and knees flexed and the feet placed on the wall. Then tilt your pelvis over a rolled towel in anterior-posterior direction. |
| “The shrimp” | Core activation while keeping the upper part of the thorax stable while moving the lower abdomen, hips and both legs. | Lying in supine in optimal alignment but with flexion in hips and knees, heals on the therapy ball. Keep a straight line between the ankles, knees and hips. | Keep the postural set while moving the therapy ball in various ways for example by rolling the ball from side to side and at the same time pushing a small ball with your hands in the direction of the knees. |
| “The crab-wiggle” | Core activation while keeping both legs stable and moving the pelvis. | Lying in supine in optimal alignment with therapy ball under lumbar back/pelvic | Keep the postural set. Then do pelvic tilts in various directions for example tilt your pelvis in anterior-posterior direction. |
| “ The crab plays ball” | Core activation while keeping both legs and thorax stable and moving the arms and shoulders. | Lying in supine in optimal alignment with therapy ball under lumbar back/pelvic. | Keep the postural set while you play with a small ball in various ways for example by keeping the arms extend towards the ceiling and pushing the ball with both hands towards the physiotherapist standing beside you. |
| “The cat” | Core activation while keeping both legs and arms stable and moving the pelvis or thorax. | Standing on all four in optimal alignment. | Keeping the postural set while moving the pelvis and shoulders in various ways for example by performing pelvic tilts. |
| “The stick” | Core activation while keeping both arms and one or two legs stable and moving the hips and legs | Side-lying, in optimal alignment. | Keep the postural set while moving the arms or the hip in various ways for example by placing the upper foot on a therapy ball and rolling the ball back and forward using the upper leg. |
| “Hands up” | Core activation while keeping the hips and legs stable while moving the arms and the trunk. | Sitting in optimal alignment. | Keep the postural set while moving the arms or thorax in various directions for example by pushing the arms and hands towards the bench (keeping an upright position) |
| “Rolling the ball” | Core activation while keeping both legs stable and moving the pelvis. | Sitting in optimal alignment. | Keep the postural set while pushing the arms in various directions and moving the pelvis in various ways for example by pushing the arms towards the bench and then moving the pelvis in anterior-posterior direction (pushing the ball back using your lumbar spine) |
| “The angel” | Core activation while keeping both legs stable and moving the arms and shoulders. | Sitting in optimal alignment. | Keep the postural set while moving the shoulders and arms in various ways for example by retracting the shoulders and abducting and elevating arms as far as you can (without loosing the contact with the back towards the therapy ball) |
Table 4: Exercises that target optimal adaptation to the base of support and core activation while selectively moving arms and legs or particular parts of the core. Focus on dynamic stability, keeping one part of the body stable while moving another. There were five different variations in each exercise (only one example is given here).
| Name | Objectives | Postural Set | Performance |
|---|---|---|---|
| “Squats” | Core activation while keeping the upper part of the thorax and the feet stable while moving the pelvis, hips and knees. | Standing in optimal alignment with the ball behind you. | Keep the postural set while doing squats in various ways for example while pushing a small ball forward with extended arms. |
| “Squats on one leg” | Core activation while keeping the upper part of the thorax and one leg stable while moving the pelvis, hip and knee. | Standing in optimal alignment with the ball in front of you. | Keep the postural set while doing squats in various ways for example while standing on one leg, pushing the hands forward towards the wall with extended arms, and pushing the other foot backwards towards a psoas-box behind you. |
| “The bear squats” | Core activation while keeping the upper part of the thorax, arms and one or two feet stable while moving the pelvis, hips and knees. | Bear-standing in optimal alignment. | Keep the postural set while doing squats in various ways for example on two legs. |
| “The bear calf-rise” | Core activation while keeping the upper part of the thorax, arms and one or two feet stable while moving the pelvis, ankle, foot and calf. | Bear-standing in optimal alignment. | Keep the postural set while doing various calf raise for example on one leg, the other leg extended behind you, the heal pointing towards the ceiling. |
| “Calf-rise” | Core activation while keeping the upper part of the thorax, arms and one or two feet stable while moving the pelvis, and ankle, foot and calf. | Standing in optimal alignment with the therapy ball in front of you. | Keep the postural set while doing various forms of calf-raise for example calf-rise on two legs. |
| “The pole” | Core activation while keeping the upper part of the thorax, arms and one or two feet stable while moving the shoulders, pelvis or ankle. | Standing in optimal alignment with the therapy ball in front of you. Shoulders, elbows, hands and fingers, extended. Hands placed on a bench behind you. | Keep the postural set while doing various movements with the shoulders for example retracting and protracting the shoulders |
| “The march” | Core activation while keeping the back and the upper part of the thorax stable while moving the ankle, knee and hip. | Standing with the ball behind you in optimal alignment. | Keep the postural set while “marching” in various ways, for example while pushing a small ball forward with extended arms, then lifting the lateral side of every other foot. |
| “The wiggle” | Core activation while keeping the upper part of the thorax, arms and one or two feet stable while moving the pelvis, hips and ankle. | Standing in optimal alignment with the therapy ball in front of you. | Keep the postural set while doing various hip and pelvic movements for example pushing the knee forward and backwards on the leg placed at the chair. |
| “The ball-play” | Core activation while keeping the back and lower part of the thorax and abdomen stable while moving the arms. | Standing with the ball behind you in optimal alignment. | Keep the postural set while throwing a ball or a towel in various ways, for example throwing a towel to the other group members and catching it again. |
| “The bounce” | Core activation while moving both arms and legs. | Standing in optimal alignment | Keep the postural set while jumping and bouncing the ball in various ways for example bouncing with every other hand. |
| “The waiter” | Core activation while keeping the feet, the back and the thorax stable while adjusting to the weight of the bottle/balancing the bottle. | Standing with the ball behind you in optimal alignment /standing in optimal alignment | Keep the postural set while holding a towel in both hands and adjusting to the weight of a bottle, which the physiotherapist lays on the towel in various ways for example while you keep your eyes closed. |
Table 5: Exercises targeting optimal adjustment to the base of support and activation of the core while recruiting larger muscle-groups in various standing positions, challenging postural control and balance. There were five different variations in each exercise (only one example is given here).
| Exercise | Objectives | Postural Set | Performance |
|---|---|---|---|
| Systematic hold-relaxation | Relaxation | Sitting in optimal alignment. | Keep the postural set, while doing systematic contraction/relaxation of the various body parts. Self-massage of the face and neck. |
Table 6: Exercises that target optimal adjustment to the base of support and activation of the core while systematically performing contraction/relaxation of other parts of the body.
The intervention emphasizes performance of exercises with optimal alignment in various body parts to enhance recovery as opposed to compensatory strategies [5]. Dynamical proximal stability is enhanced by using a therapeutic ball, either keeping the ball still against a wall (using the trunk muscles) while moving the arms or legs, or moving the ball while transferring weight from side to side or up/down (using the trunk muscles) keeping hands and/or feet stable.
Sensory stimulation of hands and feet to update body schemas is facilitated by using a massage ball or roller [5,18].
Dual tasks are integrated as variations, for example by singing while exercising. Proprioception is enhanced by performing exercises with closed eyes. Ball activities such as bouncing are included to enhance group dynamics.
Every session starts with sharing the participants´ experiences between sessions, followed by exploring their own standing balance on two legs and/or single leg standing, and then they conduct at least one exercise from each “block”. Up to ten repetitions for each exercise with good quality of movement are performed, fewer if quality deteriorates. Each session ends with active relaxation and re-exploring balance. The participants are recommended to perform 30-minute of unsupervised home exercises, optionally divided into smaller intervals, two times per week. Home training is recorded in a training diary.
The participants in the control group receive standard care, i.e. following their ordinary physiotherapy services and/or routines/ activities. These activities are recorded in a diary.
Outcome measurements
We hypothesized that high-intensity individualized group-based core stability training performed at the municipal PTs’ facilities will improve balance, walking, ADL, physical activity, and quality of life. This is reflected in the primary and secondary outcomes presented below (Table 7).
| Outcome | Measure |
|---|---|
| Primary outcomes | |
| Effect on sitting balance | Trunk Impairment Scale- Mod Norwegian version (TIS-modNV) [33] |
| Effect on balance in standing and walking | Mini Best Evaluation Systems Test (Mini-BesTEST)[34,35] |
| Secondary outcomes | |
| Efficiency in walking | 10 Meter Walk Test (10MWT)[36] 2 Minute Walk Test (12MWT)[37] MS Walking Scale-12 (MSWS -12)[38] |
| Movement quality in walking, video-recording | Rivermead Visual Gait Assessment (RVGA) [39] |
| Activities of daily living (ADL) | Multiple Sclerosis Impact Scale – 29 (MSIS-29)[40] |
| Quality of life | Multiple Sclerosis Quality of Life – 54(MSQOL-54)[41,42] EQ-5D [43] |
| Subjective perception of change | Patient Global Impression of Change (PGIC)[44] |
| Level of physical activity | Minutes of moderate to vigorous physical activity and sedentary time during 1-week (measured with the ActiGraph wGT3X-BT monitor) |
Table 7: Overview of primary and secondary outcomes.
Recruitment and study procedures
Enrollment of participants takes place at the outpatient clinic for people with MS at NLSH. The administration at the clinic sends written information on the study to patients with MS fulfilling the inclusion criteria and living in the selected municipalities. Informed consent forms are returned by mail to the MS-nurse at the NLSH’s outpatient clinic and delivered to the project leader. The date for the baseline visit is then arranged.
At enrollment, a neurologist performs the EDSS screening and records medical history and other baseline data including type of MS, EDSS, age, gender, weight, height, medications, physiotherapy and other health services during the previous 6 months. An independent appropriately trained PT blinded to group allocation performs a standardized assessment for all the participants using valid and reliable assessment tools (Table 7).
At 1 week, 3-month and 6-month post-intervention all the participants undergo the same standardized assessment performed at baseline by the assessor blinded PT (Table 8).
| Data Collected | Baseline Visit | 6-Week | 3-Month Follow-Up |
6-Month Follow-Up |
|---|---|---|---|---|
| Frequency of physiotherapy | X | X | X | X |
| Content of physiotherapy | X | X | X | X |
| Frequency of physical activity | X | X | X | X |
| Frequency of in-patient rehabilitation stays | X | X | X | X |
| TIS-modNV | X | X | X | X |
| Mini-BesTEST | X | X | X | X |
| 10-MWT | X | X | X | X |
| 2-MWT | X | X | X | X |
| RVGA | X | X | X | X |
| MSWS-12 | X | X | X | X |
| MSIS-29 | X | X | X | X |
| PGIC | X | X | X | |
| Actigraph monitor, 7days | X | X | X | X |
| MSQOL-54 | X | X | X | X |
| EQ-5D | X | X | X | X |
Table 8: Overview of data collected.
Exercise, activity and disease monitoring
On a weekly basis during the intervention period all the participants record: changes in medication, general wellbeing (qualitative selfscore), exacerbations, and physical activities using a diary with a ticketbox. In addition, participants in the intervention group only will record: degree of exhaustion following group sessions and home exercise completion using the Borg Exertion Scale [45].
Statistical methods
An intention-to-treat analysis will be performed on all randomized subjects and will serve as the primary analysis for all outcomes in this study. The data analysis will be carried out using IBM SPSS Statistics. Possible differences between the groups at baseline will be calculated by using independent sample t-test for continuous variables and chisquare for categorical variables. Primary outcomes, changes in balance in sitting and standing/walking between the groups will be calculated by using independent sample t-test as will secondary outcomes. Differences over time between groups will be investigated by using linear mixed methods, given that the data is normal distributed.
Sample size calculation
The sample size calculation for this study was based on data from the pilot study investigating the effectiveness of GroupCoreSIT on balance, walking and ADL in a similar sample of people with MS using the TIS-modNV [16] and additionally on the Mini-BESTest [35]. A difference of 0.75 SD on the Mini-BESTest between the intervention and the control group was considered as clinically significant. Fifty-six individuals with MS in each group were required to have an 80% chance to detect a 0.75 SD difference between the groups with a significance level of 0.05 (alpha) on two-sided tests. Assuming a 30% dropout, we aimed to recruit 72 persons with MS, i.e., 36 in each group for part one of the study.
Design, participants and recruitment
The qualitative study has an exploratory design, and is based on three strategic samples that will be consecutively invited to participate: i) a subset of 24 participants in the clinical trial, 12 from each group, ii) the six PTs conducting the intervention, and iii) 16-20 health professionals involved in health services to individuals with MS (Figure 2).
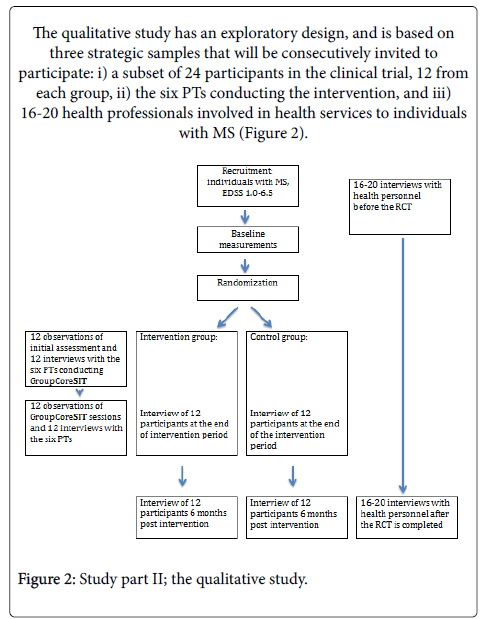
Figure 2: Study part II; the qualitative study.
Patients’ experiences: Patients’ perceptions of the intervention and standard care will be examined through qualitative research interviews [46]. The interviews will be conducted twice, at the end of intervention and 6 months post-intervention. Purposive sampling will be performed to obtain variation in training groups, EDSS, age, gender and time since diagnosis. Participants from the intervention group will be asked about the first assessment/consultation, the group situation, content and amount of training, pros and cons, home exercises and ADL. The same number of participants from the control group will be interviewed regarding their experiences with standard care, investigating the same topics. The scope of the second interviews is to investigate retrospective reflections regarding wellbeing and coping with ADL before, during and after the intervention period, selfmanagement, and continuity of care, pros and cons. The material will be transcribed and analyzed using Systematic Text Condensation [46] applying phenomenology of the body [22,23], enactive theory [25-29] complemented by neurosciences [20] as a theoretical framework.
Physiotherapists performance of intervention and reflections: Observation and videotaping of the assessment of one patient in each training group (12 observations) will be conducted to investigate what the PTs emphasize in their individual assessment prior to the first group session. These observations will be complemented by qualitative research interview with the actual PT (12 interviews) to explore the PTs’ perceptions regarding the assessment, planning of the group sessions, choices of exercises and individual goals. One session in each group will be observed and videotaped (12 observations) to investigate how the PTs tailor the intervention in situ and how they act and interact with the participants. The PTs will be interviewed at the end of each training group period (12 interviews) to illuminate the PTs’ perceptions regarding education in the intervention and experiences from conducting it, particularly focusing on goal attainment, individualization in a group setting and home exercises. The material will be transcribed and analyzed using Systematic Text Condensation [46] applying phenomenology of the body [22,23], enactive theory [25-30] complemented by neurosciences [20] and practice knowledge [47-49] as a theoretical framework.
Coordination of care and intensive physiotherapy: Qualitative interviews with health professionals will be conducted to explore coordination of care between the outpatient clinics for people with MS and the municipalities regarding high intensity physiotherapy. Eighteen health professionals (MS-nurses, neurologists, PTs) at the hospitals’ outpatient clinics and 8-10 health professionals in municipalities (general practitioners, PTs) will be interviewed before the intervention (for standard care) and after the RCT. The material will be transcribed and analyzed using Systematic Text Condensation [46] applying guidelines for health coordination [15,50] as analytical tools.
The current study aims to investigate the effects of a tailored physiotherapy program designed for individuals with MS to improve balance, walking, ADL, physical activity and health-related quality of life. The intervention is based on current theoretical frameworks and includes individualization, group dynamics and self-management. The intervention was designed for implementation in a municipality setting, but may be also suitable for specialist health care settings. The conduction of the GroupCoreSIT study will provide evidence on whether a six-week group-based, individualized high-intensity physiotherapy program for ambulant individuals with MS improves balance and walking, ADL, physical activity, and quality of life compared to standard care.
The study will also provide insight into persons with MS’ perceptions regarding the intervention and standard care, knowledge about performance of individualized group intervention, and coordination of intensive physiotherapy programs for these people.
The study is pragmatic in nature, has both qualitative and quantitative elements; hence the intention is that the conclusions drawn from the data generated will be directly transferable to clinical practice. Policy makers and therapists implementing physiotherapy programs will benefit from the results of the study, by an enhanced evidence base in this area.
Patient recruitment commenced in September 2015 and ended in January 2016.
The study is restricted to patients who have volunteered and provided written informed consent in accordance with the Declaration of Helsinki. The trial and the qualitative study received approval from the Regional Committee for Medical and Health Research Ethics in Norway (REK South-East: 2014/1715-7).
Consent for publication of data that is analyzed on a group level is obtained from all participants. Publication of videos or any other material relating to individual participants is not applicable for publication.
The data supporting the results of this study will be available upon request.
This study was funded by the Northern Norway Regional Health Authority (Project Grant 1240) and the UiT, the Arctic University of Norway.
We thank Professor Tom Wilsgaard, UiT, the Arctic University of Norway for assistance in sample seize calculations.