Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2013) Volume 1, Issue 4
The activation and subsequent platelet aggregation plays a key role in the formation of arterial thrombosis and therefore is the key therapeutic target in the treatment of acute coronary syndromes. Dual antiplatelet therapy containing aspirin and P2Y12 ADP receptor antagonist forms currently the basis in acute ST – elevation myocardial infarction (STEMI) pharmacological treatment. Nevertheless, there is a wide variability in pharmacodynamic response to administration of clopidogrel, the most frequently used P2Y12 ADP receptor antagonist. High platelet reactivity after clopidogrel administration is associated with increased risk of in - stent thrombosis and points to the suitability of laboratory monitoring of antiplatelet therapy effectivity in clinical practice. Laboratory monitoring of antiplatelet therapy by ex vivo platelet function tests may help to identify individuals with poor antiplatlet response. Recently, there is growing number of data reporting a failure in antiplatelet response following clopidogrel administration, which is specifically associated with insulin resistance and diabetes mellitus. Prasugrel, a new, potent P2Y12 ADP receptor antagonist, provides faster and more consistent inhibition of platelet function compared with clopidogrel. Prasugrel therapy was repeatedly described as an effective method to overcome clopidogrel resistance and prasugrel resistance has not yet been reliably described. Article gives a review about prasugrel resistance and its role in acute coronary syndrome patients.
The activation and subsequent platelet aggregation plays a key role in the formation of arterial thrombosis and therefore is the key therapeutic target in the treatment of Acute Coronary Syndromes (ACS). Dual antiplatelet therapy containing aspirin and P2Y12 ADP receptor antagonist forms currently the basis in acute ST – elevation myocardial infarction (STEMI) pharmacological treatment. The current intervention of several complementary ways of platelet activation and aggregation is necessary to ensure effective treatment and prevention of coronary thrombosis. The introduction of P2Y12 ADP receptor antagonists has made a major advance in the ACS treatment. Thienopyridine clopidogrel given in the CURE study (Clopidogrel in Unstable Angina to Prevent Recurrent Events) in patients with ACS significantly reduced the incidence of cardiac death and nonfatal myocardial infarction or stroke compared with patients treated with aspirin alone [1]. A 600 mg clopidogrel loading dose leads to a faster onset of action and has a greater platelet inhibitory effect than a loading dose of 300 mg [2,3]. Nevertheless, there is a wide variability in pharmacodynamic response to administration of clopidogrel, which is linked to several factors, including genotype polymorphisms [4]. High platelet reactivity after clopidogrel administration is associated with increased risk of stent thrombosis and other ischemic events [5,6]. High variability in antiplatelet response to clopidogrel administration, points to the suitability of laboratory monitoring of antiplatelet therapy efficacy in patients with acute coronary syndrome. Laboratory monitoring of antiplatelet therapy by ex vivo platelet function tests may help to identify individuals with poor antiplatlet response [7]. High platelet reactivity after clopidogrel administration is also major reason for introduction of new P2Y12 ADP receptor antagonists with more favorable pharmacodynamic profile to clinical practice [8].
Diabetes mellitus (DM) is a strong, independent risk factor of acute STEMI. DM aggravates the course of ACS and increases the risk of its complications including cardiogenic shock and death [9]. Diffuse coronary involvement [10,11], diabetic cardiomyopathy, an imbalance of the autonomic nervous system, decreased ability to develop collateral circulation [12], metabolic disorders causing ineffective and increased oxygen consumption by myocardial tissue during ischemia and during increased load [13] and an abnormal function of platelets and the coagulation system are the main factors responsible for worse prognosis in diabetic patients with ACS. Although several large clinical trials have demonstrated the efficacy of clopidogrel in the treatment of ACS, there is growing amount of data about failure in antiplatelet response after clopidogrel administration, which is specifically associated with insulin resistance and DM [14,15]. This incomplete antiplatelet response may contribute to a worse prognosis of acute myocardial infarction in patients with diabetes mellitus. The reports about incomplete antiplatelet response are based on ex vivo testing of platelet reactivity in clopidogrel therapy, as well as on the sub - analysis of clinical trials among subjects with DM, which consistently showed worse clinical outcome and an increased incidence of stent thrombosis in patients with DM [16-20]. Platelet reactivity in clopidogrel treatment >50% is associated with higher risk of ischemic events after PCI [17].
Prasugrel is a new, potent, P2Y12 ADP receptor antagonist. Prasugrel provides more consistent inhibition of P2Y12 ADP receptor and has lower intraindividual variability in efficacy compared with clopidogrel. Benefit of prasugrel therapy seems to be the highest in patients with diabetes mellitus [21]. Prasugrel therapy was repeatedly described as an effective method to overcome clopidogrel resistance [22,23] and up to very rare case reports of incomplete antiaggregant response after prasugrel administration [24]; prasugrel resistance has not been reliably described.
Stent thrombosis (Figure 1) is a morbid complication following Percutaneous Coronary Intervention (PCI). It is more frequently encountered in acute coronary syndrome patients and in patients with diabetes mellitus, bifurcation stents or in those who discontinue prematurely dual antiplatelet therapy [20,25,26]. Stent undersizing, inadequate stent expansion or stent apposition increases risk of stent thrombosis. Although periprocedural intravascular ultrasound examination may help in the correct sizing and implantation of stents, this has not been shown to improve outcomes. Drug Eluting Stents (DES) were created to reduce restenosis, however, delayed endothelialization of these stents results in longer duration of exposure to the thrombogenic stent structures, what possibly increases the incidence of stent thrombosis [27]. DES implantation is not generally recommended in primary PCI (pPCI) of culprit coronary lesion [28].
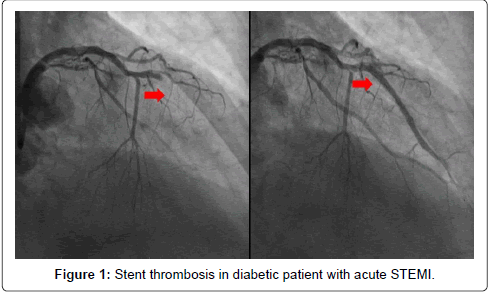
Figure 1: Stent thrombosis in diabetic patient with acute STEMI.
Stent thrombosis is a medical emergency. Dual antiplatelet therapy significantly reduces stent thrombosis risk. The antiplatelet inhibitory effect of the thienopyridine ADP receptor antagonists varies widely among individuals. Variability of antiplatelet response (antiplatelet therapy resistance) may lead to antiplatelet therapy insufficient efficacy and subsequent risk of thrombotic events. High on – treatment platelet reactivity has been associated with a substantial hazard for post – PCI cardiovascular events, including stent thrombosis [29].
Dual antiplatelet therapy significantly improves the outcome of acute STEMI treatment and reduces both short - term as well as long - term mortality in patients with acute STEMI [30]. Clopidogrel administered in the CURE study in patients with ACS significantly reduced the incidence of cardiac death and nonfatal myocardial infarction or stroke compared with patients treated with aspirin alone [1]. Variability in pharmacodynamic response/resistance to clopidogrel is currently widely discussed problem in clinical practice. High platelet reactivity after clopidogrel administration is associated with increased risk of stent thrombosis and other ischemic events [5,6]. Variability of antiplatelet response to clopidogrel is associated with several factors, such as variability of clopidogrel absorption, variability of the active metabolite creation, or variability in P2Y12 receptor antagonist activity [4]. These factors may be influenced by both genetic polymorphisms, together with several environmental factors, such as different drug interactions at the level of CYP P 450 2C19 and 3A4, or at the level of P - glycoprotein [4,31,32]. However, variability in antiplatelet response to clopidogrel may be also associated with other, currently not well understood factors. Recently, there is growing number of data reporting a failure in antiplatelet response following clopidogrel administration, which is specifically associated with insulin resistance and diabetes mellitus [14,15].
Diabetes mellitus is a strong, independent risk factor for acute STEMI [9]. One of the possible explanations for poorer prognosis of diabetic patients with ACS may be also an insufficient efficacy of treatment in patients with this metabolic disorder. Several recently published studies showed worse clinical outcome and an increased incidence of stent thrombosis in diabetic patients [16-20]. Diabetic patients treated with clopidogrel have significantly higher platelet aggregation after stimulation with ADP compared with nondiabetic subjects and significantly higher number of non-responders to clopidogrel administration can be also seen in the group of diabetic patients [19]. Platelet reactivity in clopidogrel treatment >50% is consequently associated with higher risk of ischemic events after PCI [17]. Patients with diabetes have lower clinical effect from clopidogrel treatment, what was consistently referred in results of several published randomized trials with clopidogrel [1,33-35]. However, the mechanism of clopidogrel resistance in patients with diabetes remains unclear. Erlinge et al. [15] showed a significantly higher incidence of insufficient antiplatelet response in group of patients treated with clopidogrel compared with those with prasugrel therapy. Diabetic patients were more frequently represented in the group with inadequate platelet response to clopidogrel. It is interesting, that in this trial, platelets of diabetic patients with inadequate antiplatelet response after clopidogrel administration responded well to ex vivo administration of clopidogrel active metabolite. This finding indicates a low level of resistance on P2Y12 ADP platelet receptor and supports potential interaction between DM and pharmacokinetic processes of clopidogrel metabolism. High variability of antiplatelet response to clopidogrel administration supports the effort to identify individuals with poor response by laboratory methods [7] and is one of the reasons for introduction of new ADP P2Y12 receptor antagonists with more favourable pharmacodynamic profile to clinical practice [8].
Assessing the individual level of platelet inhibition by implementing platelet function testing might help to reduce ischemic events. To assess the predictive level of platelet reactivity on ADP receptor antagonist treatment, numerous platelet function tests are currently available. Light Transmission Aggregometry (LTA) with specific inducer (ADP) represents nowadays a “golden standard” in antiplatelet response testing (Figure 2). Maximal aggregation in response to ADP with LTA testing >50% had been associated with higher risk of ischemic events [29,36]. PFA – 100® (Siemens Healthcare Diagnostics, Tarrytown, New York, USA) and Verify Now® (Accumetries, San Diego, California, USA) assay - methods both based on modified aggregometry - allow quick platelet function testing in the setting of the point of care. Verify Now® allows rapid assessment of platelet response on aspirin, P2Y12 ADP receptor antagonist and glycoprotein IIb/IIIa antagonist treatment in one blood sample [37]. Vasodilator - stimulated phosphoprotein (VASP) phosphorylation assessment represents a specific method for ADP receptor antagonist activity assessment (Figure 3). Using flow cytometry it is now possible to quantify the amount of phosphorylated VASP and thereby to measure the amount of unblocked ADP receptor [38]. Advantage of this examination is its specificity for ADP receptor intracellular signaling pathway and sample stability. The disadvantages are instrumental and financial requirements.
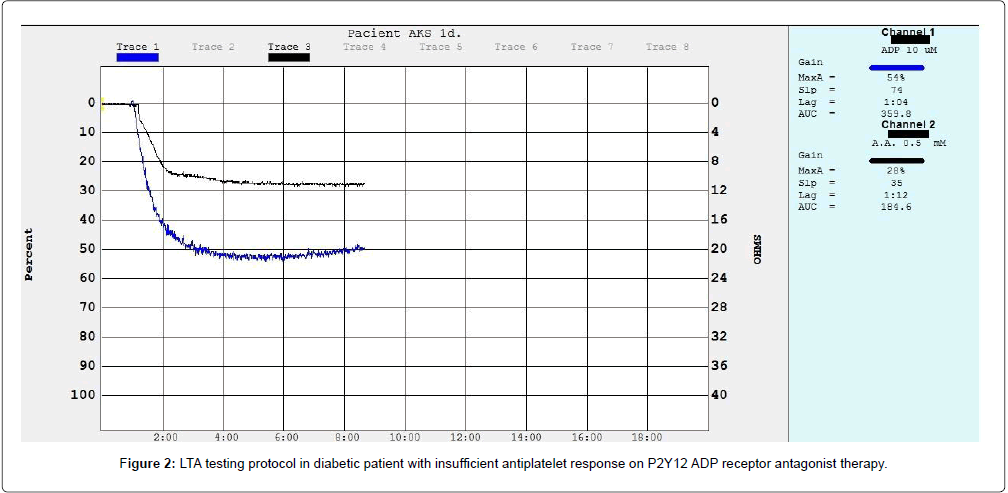
Figure 2: LTA testing protocol in diabetic patient with insufficient antiplatelet response on P2Y12 ADP receptor antagonist therapy.
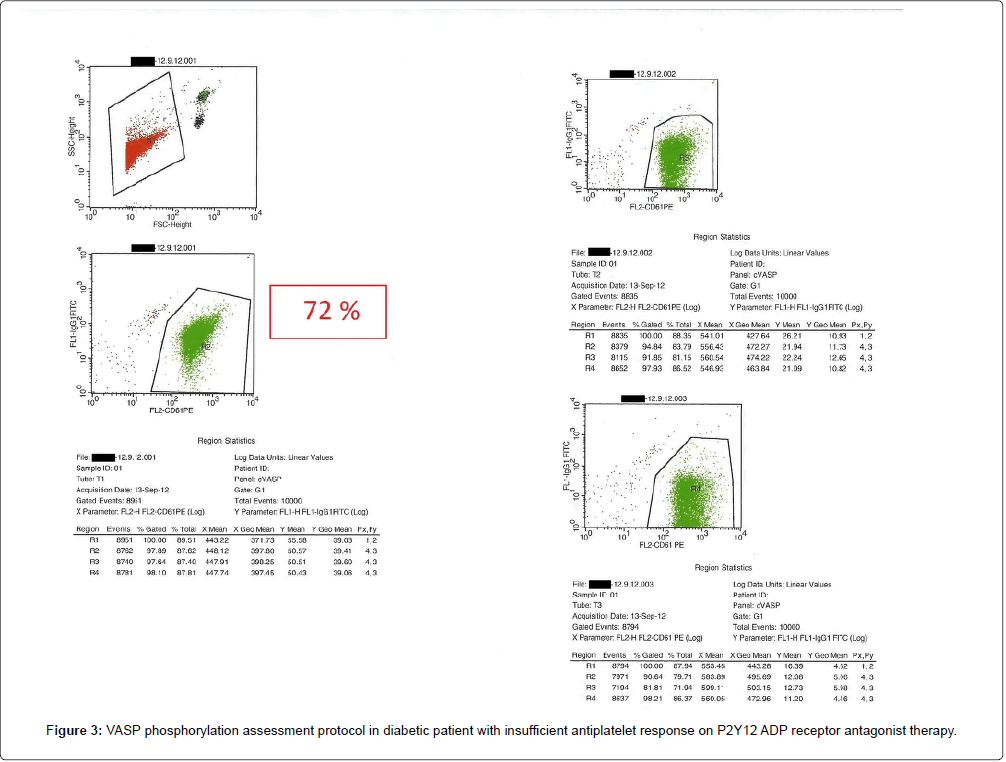
Figure 3: VASP phosphorylation assessment protocol in diabetic patient with insufficient antiplatelet response on P2Y12 ADP receptor antagonist therapy.
Platelet function monitoring may possibly help for guiding a switch over to different available P2Y12 ADP receptor antagonists or the use of adjuctive antiplatelet therapy to overcome high platelet reactivity in identified patients in order to reduce the risk of stent thrombosis and repeated myocardial infarction.
Prasugrel, a new, potent, irreversible tienopyridine P2Y12 ADP receptor antagonist, provides faster and more consistent inhibition of platelet function compared with clopidogrel [21]. The response to prasugrel is not affected by CYP2C19 inhibitors, loss of CYP2C19 gene function, or decreased function of P - glycoprotein [39]. The TRITON - TIMI 38 study [21], which compared prasugrel and clopidogrel in patients with ACS without prior ADP receptor antagonist therapy showed, that prasugrel significantly reduced the incidence of the combined primary endpoint (cardiac death, nonfatal MI, stroke), the risk of myocardial infarction and the risk of stent thrombosis. Benefit of prasugrel treatment was the most significant in group of diabetic patients, in whom prasugrel therapy significantly reduced the risk of ischemic events, including the risk of recurrent MI and the risk of stent thrombosis, without increasing the risk of serious bleeding complications. Prasugrel therapy was repeatedly described as an effective method to overcome clopidogrel resistance [22,23]. Silvano et al. described a rare case of resistance to both clopidogrel and prasugrel in non - diabetic patient with acute STEMI due stent thrombosis [24]. However, this patient did not receive prasugrel loading dose and was treated only with prasugrel maintenance dose. Abnormal metabolism of antiplatelet drugs due to reduced activity of CYP P 450, the main enzyme complex responsible for the active tienopyridine antagonists metabolite formation [40-42], was considered to be the most probable mechanism of drug resistance in this case. Reduced activity due to genetic variability of CYP P450 2C19 and 3A4 was subsequently verified by genetic testing [24]. Except of this rare case of insufficient antiplatelet response to prasugrel, prasugrel resistance has not been reliably described. Nevertheless, results of recently published studies [43,44] suggest, that real prevalence of insufficient antiplatelet response after prasugrel administration may by higher, than is traditionally considered. Bonello et al. [44] pointed on the fact that up to 25 % of patients with ACS did not reach effective antiplatelet response even after 6 - 12 hours from prasugrel loading dose administration. The exact mechanism how diabetes affects the tienopyridine antagonist activity is currently not known. Erlinge et al. [15] pointed on the fact that platelets of diabetic patients with poor antiplatelet response to clopidogrel responded well to ex vivo administration of the active clopidogrel metabolite. This finding suggests a low level of resistance on platelet P2Y12 ADP receptor in diabetes and supports a potential interaction of diabetes with pharmacokinetic processes of clopidogrel metabolism. Whether diabetes affects pharmacokinetic processes of prasugrel metabolism as well, or an insufficient efficacy of prasugrel in diabetic patients is caused by another mechanism remains recently unclear and further studies will be needed for the final clarification of this issue.
Sufficient antiplatelet treatment effectively decreases the risk of stent thrombosis. On the other hand, high on – treatment platelet reactivity had been repeatedly associated with the risk of thrombotic events after PCI. Time to peak platelet inhibition after ADP receptor antagonist administration varies in patients with DM in contrary to nondiabetic patients. Insufficient efficacy of antiplatelet therapy may be one of the factors participating in the worse prognosis of acute STEMI in diabetic patients. Insufficient efficacy of antiplatelet therapy in diabetic patients may appear also when new antiplatelet drugs are used. Insufficient efficacy of prasugrel appears to be mostly marked in first hours after loading dose administration. It is questionable whether better results of studies with glycoprotein (GP) IIb/IIIa receptors antagonists in patients with diabetes [45] were at least partially achieved due to the overlap of insufficient efficacy of dual antiplatelet therapy in the first hours after its administration. Monitoring of antiplatelet therapy efficacy using laboratory platelet function tests may help to identify patients with insufficient antiplatelet response and allow an early initiation of effective approach. Routine introduction of antiplatelet therapy efficacy testing especially in high risk diabetic ACS patients should become at least an object of consideration in the near future.
This study was supported by project APVV (Slovak Research and Development Agency) 0222-11, by project CEPV II (ITMS 26220120036) which is co - financed from EC sources, by research project of Slovak Society of Cardiology 2012 – 2015 and by Young Heart Science association.