Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2014) Volume 3, Issue 2
Background: Parathyroid gland (PTG) involvement by differentiated thyroid cancer (DTC) patients is rare and its influence on disease outcome has been less studied. We aimed to evaluate the frequency and patterns of PTG involvement in DTC patients and to evaluate the influence of PTG infiltration by DTC on treatment outcome in our cohort. Methods: Demographic, clinicopathologic characteristics and treatment outcomes of sixteen patients of PTG involvement were reviewed in a series of consecutive 823 DTC patients treated during July 2001 and December 2012 with thyroidectomy followed by radioactive iodine therapy and radiation therapy. Data regarding the occurrence of locoregional recurrence (LRC) or distant metastasis (DM), disease free survival (DFS) and overall survival (OS) rates were recorded. LRC, DMC, DFS and OS rates were also compared to matched controls (T3, T4a and M1) using the log-rank test. Results: Mean age of cohort was 57.5 years (42.9-72.1) with female gender preponderance (75%). Sixteen cases of DTC with PTG involvement were found among the 823 patients (1.94%). Fourteen cases (87.5%) had direct extrathyroid extension (ETE) to PTG and 2 (12.5%) had metastatic foci. Majority of involved PTG were located within the thyroid capsule (intracapsular) (50%). PTG involvement was associated with extrathyroidal extension in 13 cases (81.3%). Median size of primary thyroid cancer was 3 cm (2.2-5.4). Fourteen patients (87.5%) with PTG involvement had positive cervical lymph nodes and 12 patients (75%) had lymphovascular space invasion. At 5 years, LRR, DMC, DFS and OS rates were 87.1%, 66.3%, 64.3% and 58.3% respectively. DTC patients with PTG involvement had similar DFS as compared to pT4a (62.5% vs. 60.4%: p 0.08). Conclusion: PTG involvement in DTC patients is rare and is associated with older age, advanced stage and with ETE. In the presence of ETE, PTG involvement can be high.
<Keywords: Differentiated thyroid cancer, Parathyroid gland involvement, Frequency, Disease outcome
The incidence of parathyroid glands (PTG) involvement in differentiated thyroid carcinoma (DTC) and its prognosis are not well known, since the invasion of the PTG is not routinely sought during surgery [1]. Reported incidence rate of PTG involvement in PTC is 0.5%-7.9% depending on number of retrieved PTG post-thyroidectomy histopathological examination [2]. However the true prevalence of PTG infiltration is difficult to estimate during the thyroidectomy as special attention is paid to the preserve the PTG [3]. PTG infiltration has not been taken into consideration in the staging system for DTC possibly due to its rarity, but theoretically it can significantly affect the staging and prognosis in patients with DTC i.e. T4a if the invasion of PTG is through direct extrathyroidal extension (ETE) or M1 if the invasion is through hematogenous pathway without any direct ETE and such patients may be at high risk in terms of recurrence and survival [4-6]. However no data is available to determine the influence of PTG involvement by DTC on disease outcome.
We aimed to evaluate the frequency and patterns of PTG involvement in DTC patients and to evaluate the influence of PTG infiltration by DTC on disease outcome in our cohort.
After formal approval from institutional ethical committee, medical charts of consecutive 823 patients with confirmed pathologic diagnosis of differentiated thyroid carcinoma (DTC) were reviewed retrospectively, who were treated in our hospital during period of July 2001 and December 2012 using computer data based system. Patients with PTG involvement were retrieved in following manner; demographic data (age at diagnosis, gender and symptomatology).
Histopathological characteristics. After thyroidectomy, thyroid gland surgical specimens were fixed in formaldehyde 10% and multiple areas of the gland, tumor and capsule were sampled, embedded in paraffin and cut in 4 micrometer width sections and stained with hematoxylin and eosin (H&E) and immunohistochemistry with thyroid transcription factor-1 (TTF-1) to evaluate histological variants of DTC, size, nodal status, ETE, lymphovascular space invasion (LVSI) status, grade and extent of metastatic disease of DTC
A total number of retrieved PTG and size. PTG involvement was defined as the infiltration of the thyroid tumor into the PTG, in the presence or absence of direct ETE from the primary tumor.
Treatment modalities (surgery, adjuvant radioactive iodine (RAI) therapy and radiation therapy) and outcomes
Locoregional recurrences rates (LRR), locoregional control (LRC) and distant metastasis (DM) and distant metastasis control (DMC)
Disease-free survival (DFS) was defined as the duration between the completion of treatment and the date of documented disease recurrence, death resulting from the cancer, and/or last follow-up visit with disease (censored). Overall survival (OS) was defined as the duration between the completion of treatment and the date of patient death or last follow-up visit (censored). LRC, DMC, DFS and OS rates were compared to matched controls using the log-rank test. The Student’s unpaired t test was used to determine the significance of the difference between two groups. A p value of 0.05 was considered statistically significant.
Cox regression model was used to evaluate the effect of the potential prognostic factors on locoregional, distant control, and disease free survival. Bonferroni correction was applied to overcome multiplicity problem. Statistical analyses were performed using the computer program SPSS (Statistical Package for the Social Sciences, version 17.0, SPSS Inc, Chicago, IL).
Clinical characteristics
We found 16 cases of DTC with PTG involvement among the 823 patients, for a rate of 1.94%. Characteristics of patients are given in Table 1. Mean age of cohort was 57.5 years (42.9-72.1) with female gender preponderance (75%). PTG involvement was predominantly seen in papillary thyroid carcinoma (93.7%), and was associated with extrathyroidal extension in 13 cases (81.3%). Median size of primary thyroid cancer was 3 cm (2.2-5.4). Fourteen patients (87.5%) with PTG involvement had positive cervical lymph nodes and 12 patients (75%) had lymphovascular space invasion.
| Variable | N (%) |
|---|---|
| Age (years) Age below 40 years Age above 40 years |
57.5 (42.9-72.1) 6 (37.5%) 10 (62.5%) |
| Gender Male Female |
4 (25.0%) 12 (75.0%) |
| Histology Papillary Follicular |
15 (93.7%) 1 (6.3%) |
| Primary tumor size Below 2 cm Above 2 cm |
2 (12.5%) 14 (87.5%) |
| T1 T2 T3 T4 |
- 2 (12.5%) 6 (43.7%) 8 (50.0%) |
| Extra-thyroidal extension Yes No |
13 (81.3%) 3 (18.7%) |
| Lymphovascular space invasion Yes No |
12 (75.0%) 4 (25.0%) |
| Nodal status N0 N1 |
2 (12.5%) 14 (87.5%) |
| Other sites of metastasis M0 M1 Lungs Bones |
11 (68.7%) 5 (31.3%) 4 (80.0%) 1 (20.0%) |
| Adjuvant Radioactive iodine ablation Dose 100 mCi 150 mCi 200mCi |
16 (100) 1 (6.3%) 8 (50.0%) 7 (43.7%) |
| Adjuvant Local Radiation therapy (IMRT) Dose Dose per fraction |
7 (43.7%) 60 Gy (59.4-66) 200 cGy |
Table 1: Patients characteristics (IMRT = intensity modulated radiation therapy, mCi=mill curie, Gy=Gray)
Histopathological characteristics
A Total of 113 patients (13.7%) among 823 DTC patients had advertent or inadvertent Parathyroidectomy. Among 191 histopathologically examined parathyroid gland specimens, the frequency of PTG involvement was 8.38%. Out of 16 cases, 14 (87.5%) had direct infiltration of PTG and 2 (12.5%) had metastatic foci in PTG from hematogenous spread. Majority of involved PTG were located within the thyroid capsule (intracapsular) (50%) (Table 2).
| Variables | Number (%) |
|---|---|
| Parathyroidectomy Patients Number 1 2 3 4 Location Extracapsular Intracapsular Intrathyroidal |
113/823 (13.7%) 2 (1-4) 62 (54.8%) 29 (25.7%) 17 (15.1%) 5 (4.4%) 42/113 (37.2%) 49/113 (43.4%) 22/113 (19.5%) |
| Parathyroid glands infiltration Direct Hematogenous |
14/16 (87.5%) 2/16 (12.5%) |
| Gross size of parathyroid glands | 4.1 millimeter (3.4-4.3) |
| Location of involved parathyroid glands Extracapsular Intracapsular Intrathyroidal |
7 (43.8%) 8 (50.0%) 1 (6.2%) |
Table 2: Parathyroidectomy specimen characteristics
Treatment outcomes
Median follow-up period was 4.62 years (3.5-9.2). All 16 patients received adjuvant RAI therapy and seven (43.7%) patients received further locoregional radiation therapy after thyroidectomy. Among sixteen DTC patients with PTG involvement, two patients had locoregional recurrence (LRR). Median time for first LRR was 18 months. LRR were seen in patients without neck irradiation. Overall 5 year LRR rate was 87.1%.
Five patients with PTG involvement and initially M0 developed distant metastasis (DM). Four (80%) had lung metastasis and one (20%) had bone metastasis. Median time to develop initial DM was 17 months. At 5 years, distant metastasis control (DMC) was 66.3%.
At 5 years, disease free survival (DFS) and overall survival (OS) rates were 64.3% and 58.3%. DFS rates were significantly lower in patients with DTG involvement as compared to remaining cohort of pathological negative PTG; however OS rates were found similar (Figures 1A and 1B). Further subgroup analysis showed that DTC patients with PTG involvement (13 patients) had worse DFS rates as compared to matched control T3a without PTG involvement (174 patients), no difference DFS rates between T4a with PTG infiltration (7 patients) and matched control T4a without PTG invasion (32 patients) and better DFS rates of DTC with PTG involvement (10 patients) as compared to matched control metastatic DTC without PTG metastasis (137 patients) (Figures 2-4).

Figure 1a: Disease free survival
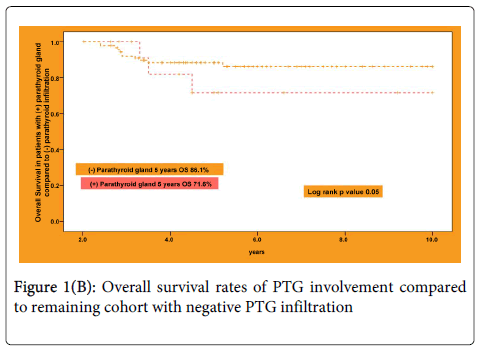
Figure 1b: Overall survival rates of PTG involvement compared to remaining cohort with negative PTG infiltration

Figure 2: Cumulative disease free survival probability of stage T3 with and without parathyroid involvement (matched control group)
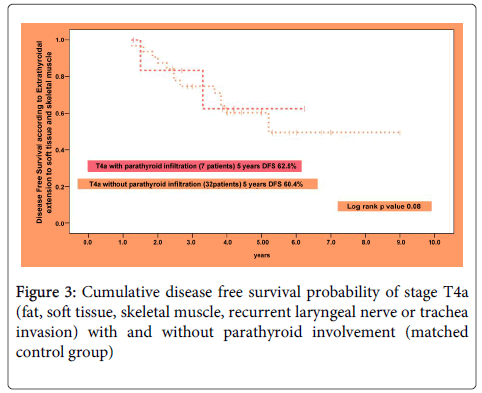
Figure 3: Cumulative disease free survival probability of stage T4a (fat, soft tissue, skeletal muscle, recurrent laryngeal nerve or trachea invasion) with and without parathyroid involvement (matched control group)
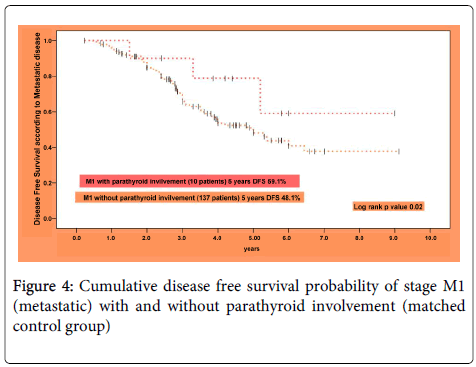
Figure 4: Cumulative disease free survival probability of stage M1 (metastatic) with and without parathyroid involvement (matched control group)
In Cox regression model, PTG involvement in DTC was found an independent significant prognostic factor for LRC [hazard ratio (HR) 2.3 95% confidence interval (95% CI) 1.9-3.1], DMC (HR 2.1; 95%CI 1.8-3.0) and DFS (HR 2.7; 95%CI 1.9-3.1).
The infiltrative or metastatic PTG involvement is a rare entity in patients with DTC. In our cohort, the frequency of PTG was 1.94%, which is consistent with other reported results [1-3]. However, the frequency was much higher among patients with histologically proven advertent or inadvertent Parathyroidectomy (8.38%). Further in our cohort, PTG was found to be associated with older age, advanced stage, higher LVSI, high number of positive cervical lymph nodes and metastasis. These results are consisted with study by Kakudo K et al. [3].
In majority of our cases, PTG were found directly infiltrated by primary tumors (14/16), of whom 81.3% cases had ETE and seven cases had ETE with fat, skeletal muscle, recurrent laryngeal nerve and trachea infiltration. These findings suggest that PTG involvement by DTC can occur at early or advanced stage of primary tumor because of immediate extracapsular or intracapsular location of PTG, as seen in our cohort that involved PTG were located outside of capsule in seven cases and within capsule in eight cases [7]. Metastatic foci (hematogenous spread) were seen two patients (one papillary and one follicular). Possible hypothesis is that blood supply to PTG is mainly from inferior thyroidal vessels and lymph drainage is also made via thyroid gland vessels [8].
In our cohort, five year DFS and OS rates were found better; 64.3% and 58.3% respectively. Further our results showed that DTC patients with PTG involvement had similar DFS as compared to pT4a (infiltration to fat, skeletal muscle, recurrent laryngeal nerve and trachea). Such group of patients can benefit from additional postoperative radiotherapy following RAI therapy [9,10]. However the current staging system for DTC does not include the PTG as pT4a (direct infiltration of PTG) or M1 (metastatic involvement of PTG) due to the rarity of the event [5]. Clinical behavior is similar to primary pT4a and such patients may benefit from additional locoregional radiotherapy to improve LRC and DFS rates.
PTG involvement in the presence of ETE is high and we believe that in presence of ETE (preoperative or perioperative) advertent single Parathyroidectomy can be performed to exclude PTG involvement without any risk symptomatic temporary or permanent hypocalcemia postoperatively [11]. However in our study we did not see postoperative temporary or permanent hypocalcemia in our cohort.
In conclusion, PTG involvement in DTC patients is rare and has been less studied. DTC patients with PTG involvement are associated with older age, advanced stage and with ETE. However more multi-institutional studies are warranted to determine frequency of PTG involvement and its impact on treatment outcome.