Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Short Communication - (2015) Volume 3, Issue 2
Decline in fertility rate is alarming and it affects about 15.0 % of couples trying to conceive. Globally, 5.0-7.0% of the general male population is affected by infertility and the trend may increase in future. Diabetes mellitus, a state of chronic hyperglycemia, is found to be an effective cause associated with male infertility. Since both type I and type II diabetes influences male infertility, we aimed to identify the genetic link underlying diabetic male infertility. Y chromosome microdeletions were screened in 12 Type I & Type II diabetic infertile male patients of varying seminogram profile by employing Triplex (sY84, sY99, and sY156) and individual (sY86, sY100, sY134 and sY254) PCR. sY156 STS marker of AZFc region was invariably deleted in 5 diabetic infertile men in addition to sY86, sY100, sY134 STS markers. No functional gene has been assigned for the 923bp DNA fragment encoded by the sY156 STS marker. Rather, it belongs to a processed pseudogene TRIM60P8Y. Frequent deletion of the sY156 marker in AZFc region in diabetic infertile men is unclear. The result showed can be further substantiated with more number of samples.
<The world wide decline in fertility rate is alarming and it affects about 15.0% of couples trying to conceive. Globally, 5.0-7.0 % of the general male population is affected by infertility and the trend may increase in future, considering the apparent decline of sperm count in industrialized countries [1]. In India, the percentage of male infertility has currently increased to 60% now against 40% in 1980s (www.newindianexpress.com). Male infertility lies at the crossroads of genetic determinants and environmental effects. Although the exact genetic mechanisms of male infertility are still unclear, this multifactorial disorder is associated with a host of medical diseases. Despite enormous progress in the understanding of human reproductive physiology, the underlying cause of male infertility remains undefined in about 50% of cases, which are referred to as idiopathic infertility [2,3].
Diabetes mellitus, a state of chronic hyperglycemia, is found to be an effective cause associated with male infertility [4]. In 2014, WHO estimated the global prevalence of diabetes to be 9% among adults aged 18+ years. According to International Diabetes Federation, India ranks 79th position in the world with the comparative prevalence of 9.09%. It is a well-recognized cause of male sexual dysfunction at multiple levels including endocrine control of spermatogenesis, penile erection and ejaculation, and spermatogenesis [5]. The potential impact of the increase in diabetes in young men and its effect on their reproductive health has also had much less attention.
Genetic causes of infertility are an important etiological factor leading to irreversible, partial or complete spermatogenetic arrest which account for 10-15% of severe male factor infertility. Y chromosome microdeletions are a common molecular cause of spermatogenic failure. The microdeletions that occur in the AZF [AZoospermic Factor] region of the long arm of the Y chromosome affect genes that are involved in spermatogenesis. There are three recurrently deleted non-overlapping sub regions in the proximal, middle and distal Yq11 regions in the deleted interval designated as AZFa, AZFb and AZFc [6]. Since both type I and type II diabetes influences male infertility, we aim to identify the genetic link underlying diabetic male infertility and therefore attempt to assess the association of Y chromosome microdeletions in diabetic infertile men of Coimbatore district, Tamil Nadu, South India.
This study was conducted on subjects attending infertility clinics in Coimbatore District of Tamil Nadu, South India. Blood samples were collected from diabetic (Type I & Type II) infertile male patients (n=12) and a group of non-diabetic men with proven fertility (n=10), who served as control. All the procedures followed were in accordance with the ethical standards of the Institutional ethical clearance of PSG (Proposal number: 10/357).
DNA extraction and deletion mapping by Triplex PCR
DNA was extracted from 2 ml of peripheral blood using standard procedure [7]. Triplex PCR for Y chromosome microdeletions on diabetic and non-diabetic infertile and control men were carried out using STS (Sequence Tagged Sites) markers (sY84, sY99 and sY156) on the long arm of the Y chromosome. Primer sequences were collected from NCBI (National Center for Biotechnological Information). PCR (Polymerase Chain Reaction) for sY86, sY100, sY134 and sY254 STS markers were also performed separately. The sex-determining region of Y, SRY (STS sY14), was included as the internal control. DNA from fertile male subjects was taken as the positive control and the DNA from a female subject served as a negative control. The samples were subjected to PCR amplification using initial denaturation for 5 min at 94ºC and 35 cycles of 94ºC for 1 min, with the annealing temperature varying from 56ºC to 60ºC for 1 min and extension at 72ºC for 1 min. The final extension time was 5 min at 72ºC. The PCR products were analyzed on a 2% agarose gel containing ethidium bromide (0.5 μg /mL). An STS was considered absent only after at least three amplification failures in the presence of both the internal control (SRY) and the positive control. Semen analysis was also done and the patients were classified accordingly.
Semen analysis report of diabetic infertile men
Semen analysis of diabetic infertile men ranged from azoospermia to oligozoospermia whereas normozoospermic men revealed normal count (>20 × 106/ml). Of 12 semen samples analyzed, 6 were oligoasthenozoospermic; 2 each of oligozoospermia, asthenozoospermia and azoospermia.
PCR analysis for Y chromosome microdeletions
We, for the first time made an attempt to study the influence of diabetes mellitus on Y chromosome microdeletion of diabetic infertile men. Control men showed no deletion of STS markers used for amplifying AZF a, b, c regions (Figures 1-5). Among the 6 oligoasthenozoospemic men, three showed deletion in AZFc region (sY156) (Figure 6) and two in AZFb region. One patient shows deletion of sY134 STS (Figure 4) marker while the other showed deletion of sY100 STS marker (Figure 9). One azoospermic diabetic infertile man showed deletion in all the three regions (sY86, sY100, sY156) (Figures 6,8,9) whereas another showed deletion of AZF b and c (Figure 6) (sY100, sY156) region only (Table 1). To our astonishment no deletion was found in oligozoospermic and asthenozoospermic diabetic men (Figures 6-9). Control men showed no deletion of STS markers used for amplifying AZF a, b, c regions. Deletions of STS markers were in correlation with severity of infertility and sY156 was frequently deleted in severe infertile cases (Table 1). In this study, least number of total Y chromosome deletions was observed in AZFa (8.33%) and AZFb (33%) region whereas maximum deletion was seen in AZFc (41.6%) region. This is in agreement with the earlier studies which showed that the incidence of deletion in the AZFc region was high compared with the AZFa and AZFb regions [8-11].
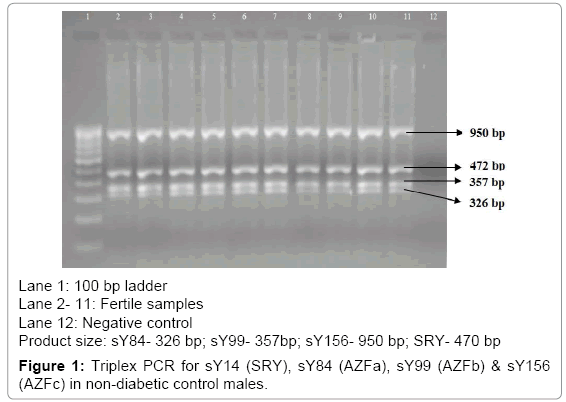
Figure 1: Triplex PCR for sY14 (SRY), sY84 (AZFa), sY99 (AZFb) & sY156 (AZFc) in non-diabetic control males.
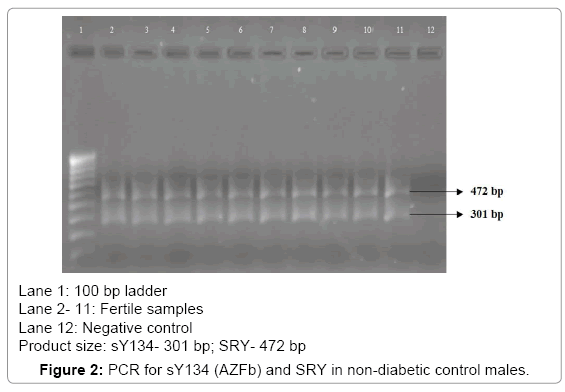
Figure 2: PCR for sY134 (AZFb) and SRY in non-diabetic control males.
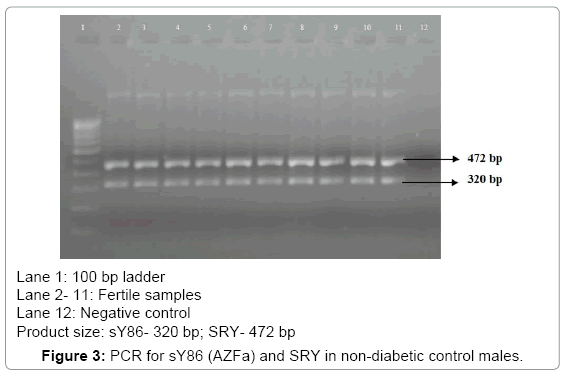
Figure 3: PCR for sY86 (AZFa) and SRY in non-diabetic control males.
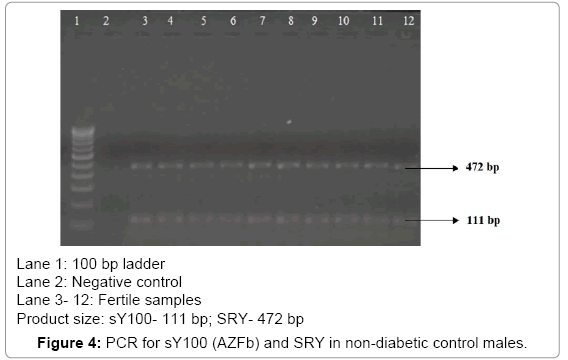
Figure 4: PCR for sY100 (AZFb) and SRY in non-diabetic control males.
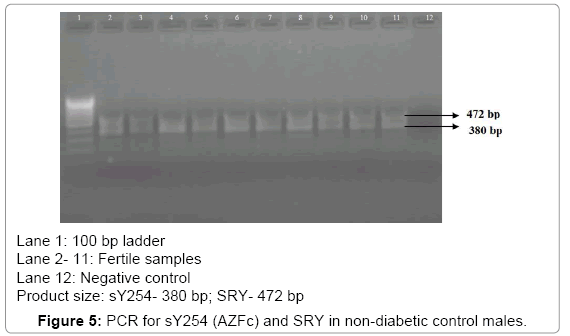
Figure 5: PCR for sY254 (AZFc) and SRY in non-diabetic control males.
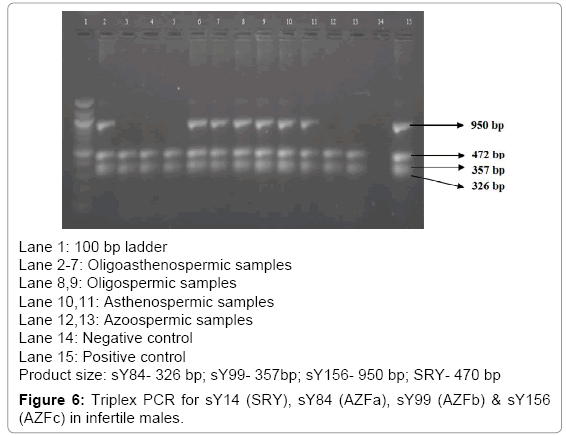
Figure 6: Triplex PCR for sY14 (SRY), sY84 (AZFa), sY99 (AZFb) & sY156 (AZFc) in infertile males.
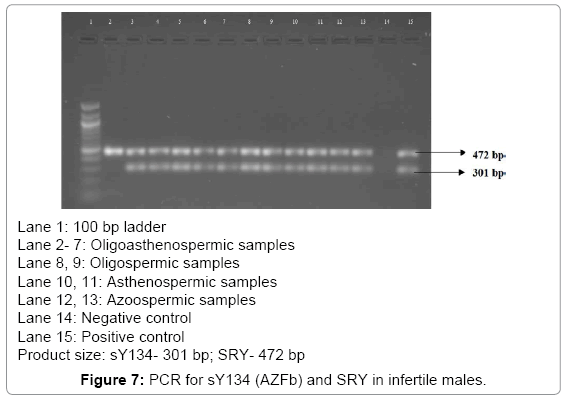
Figure 7: PCR for sY134 (AZFb) and SRY in infertile males.
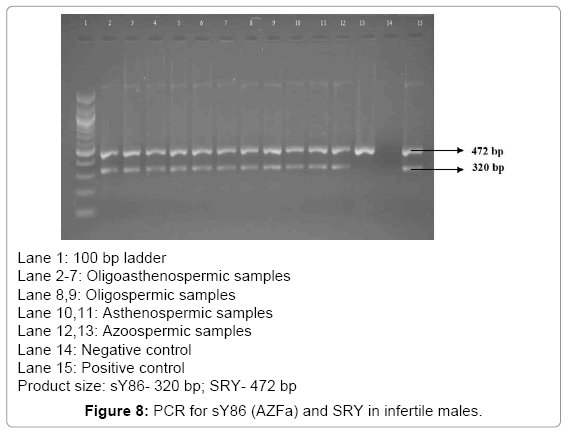
Figure 8: PCR for sY86 (AZFa) and SRY in infertile males.
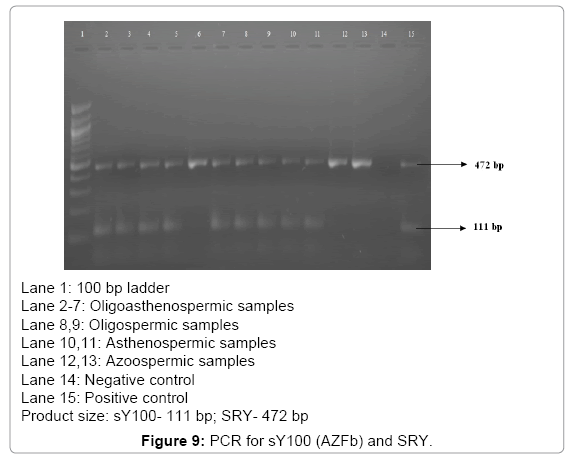
Figure 9: PCR for sY100 (AZFb) and SRY.
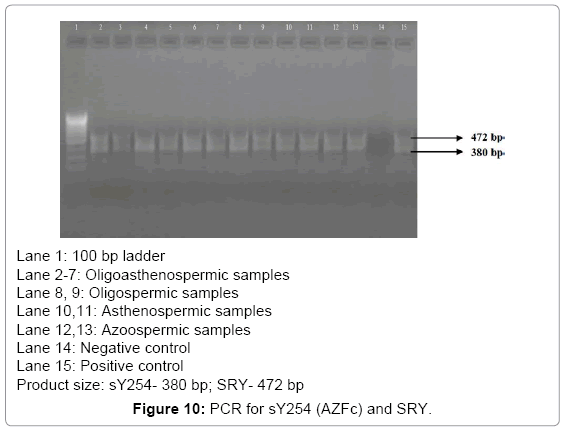
Figure 10: PCR for sY254 (AZFc) and SRY.
| STS markers | Diabetic infertile men (N=12) | Control men N=10 | |||||||||||
| Oligoasthenozoospermia | Oligozoospermia | Asthenozoospermia | Azoospermia | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| AZFa-sY86 | ✔ | No deletion of STS markers | |||||||||||
| AZFb | |||||||||||||
| sY100 | ✔ | ✔ | ✔ | ||||||||||
| sY134 | ✔ | ||||||||||||
| AZFc-sY254 | |||||||||||||
| Triplex PCR | |||||||||||||
| AZFa-sY84 | |||||||||||||
| AZFb-sY99 | |||||||||||||
| AZFc-sY156 | ✔ | ✔ | ✔ | ✔ | ✔ | ||||||||
✔- Deletion
Table 1: d Y chromosome STS markers in diabetic infertile men.
The recommendations of the European Academy of Andrology (EAA), suggest that over 90 per cent microdeletions can be detected by the use of 2 STS markers for each AZF loci. Therefore we used sY156 and sY254 for detecting microdeletions in AZFc locus. To our astonishment 41.6% of diabetic infertile men showed deletion of sY156 marker. Since sY156 STS marker was invariably deleted in 5 diabetic infertile men, we tried to find the expression profile of this STS marker. No functional gene has been assigned for this 923bp DNA fragment. Rather it belongs to processed pseudogeneTRIM60P8Y (tripartite motif containing 60 pseudogene 8, Y-linked) extending from 23,025,594 - 23,026,663 forward strand on Y chromosome. It also codes for long non coding RNA (lncRNA) ENST00000436338 spanning around 762 bp. TRIM60P8Y has been alternatively named as HAVANA gene OTTHUMG0000043859 coding ring finger protein 129 (RNF129) pseudogene. Frequent deletion of sY156 marker in AZFc region in diabetic infertile men is unclear. In near future, the advanced approaches of genomics and proteomics would help to interpret the causative mechanisms for diabetic male infertility. There is no much previous literature that depicts a clear association between infertility and diabetes. This study addresses connection between Y chromosome microdeletion and diabetic male infertility. The result showed can be further substantiated with more number of samples.
STS walking of Y-chromosome can be done to find the gene that is deleted either upstream or downstream of sY156 STS marker and relation between diabetes and male infertility can be elucidated. Despite the lack of conclusive studies, it is evident that there are enough compelling reasons to believe that the future of male fertility may be impaired by diabetes mellitus.