Journal of Women's Health Care
Open Access
ISSN: 2167-0420
ISSN: 2167-0420
Research - (2021)
Background: Breast cancer is the leading cause for maternal mortality globally, especially in developing countries like Ethiopia. The incidence is increasing specially in developing regions. Regular breast self-examination is one of the most cost-effective methods for early detection of breast cancer in asymptomatic women.
Objective: The aim of the study is to assess the level of knowledge and breast self-examination practice, and its associated factors among students in private universities at west Arsi zone, south east Ethiopia.
Methods: A facility based cross-sectional study design was conducted from April 1 to 30, 2018. A total of 355 undergraduate female students were participated in the study. Simple random sampling technique was used to select the study participants. Binary and multivariate logistics regression analyses was applied using backward step wise method with p <0.05 and p>0.25 criteria to enter and exit from the model respectively. Odds ratios with 95% confidence intervals were computed and significance of all tests was determined at p ≤ 0.05.
Results: From all participants 84(23.7%) were knowledgeable about breast self-examination and 148(41.7%) and 65(18.3%) of them have knowledge about sign and risk of breast cancer respectively. Only 112(31.5%) ever practiced breast self-examination, from those 79(22.3) of them practice breast self-examination monthly and most them started breast self-examination between age of 20-30 years. After adjusting for possible confounders; Field of study, knowledge of breast cancer risk and sign were significantly associated with knowledge of breast self-examination. Knowledge about breast self-examination and from constructs of health belief model perceived susceptibility and perceived barriers were significantly associated with breast self-examination practice.
Conclusion: knowledge and practice of breast self-examination of undergraduate female students was low as a National guideline of Ethiopia FMOH that states all female age above 20 years should practice BSE. Therefore, the health sector should design strategies to improve female students’ knowledge and practice of breast self-examination.
Knowledge of breast cancer, Practice of breasts self-examination, Screening, Women students.
BC: Breast Cancer; BSE: Breast Self-Examination; CBE: Clinical Breast Examination; FMOH: Federal Ministries of Health; KAP: Knowledge, Attitude and Practice; SPSS: Statistical Package for Social Science; WHO: World Health Organization
Prevention is the best option to tackle the rising epidemic of breast cancer. Most successful approach to decrease mortality due to breast cancer is the application of secondary prevention. In this regard, screening, early detection and health awareness programs are cornerstones [1]. Early detection and diagnosis can greatly increase chances for successful treatment and thus increasing awareness of the possible warning signs of the disease among the general public is a necessity [2]. Breast self-examination (BSE), clinical breast examination (CBE) and mammography are the important methods traditionally used for detecting the breast cancer in the early stage. Mammography screening is costly, grab considerable economic and human resources and hence not practicable in developing countries. Women should be familiar with the known benefits, limitations, and potential harms associated with breast cancer screening and how their breasts normally look and feel and report any changes to a health care provider right away. Breast selfexamination (BSE) is one of screening methods, which involves the woman herself looking at and feeling each breast for possible lumps, distortions or swelling. It is a simple exercise which can potentially save the life of a woman. It is recommended for every woman above the age of 20 years to be done for 20 minutes every month. It is a cost-effective method of early detection of cancer of the breast especially in resource poor countries [3]. It could detect 40% of breast lesion, which vital for effective treatment. Therefore, education and adherence are a gateway to health promotion behaviors [4].
Breast Cancer is the top cancer in women worldwide and is increasing a particularly developing countries where the majority of the cases are diagnosed in late stage, Although breast cancer is thought to be a disease of developed world, almost 50% of breast cancer cases and 58% of death occur in less developed countries Incidence rates vary greatly worldwide from 19.3 per 100,000 women in Eastern Africa to 89.7 per 100,000 women in Western Europe [5].
More than 60% of the world’s total cases occur in Africa, Asia and Central and South America and these regions account for about 70% of the World’s cancer death, a situation that is made worse by the lack of early detection and access to treatment, the number of deaths was 21.2 per 100,000 women per year. These rates are ageadjusted and based on 2010-2014 cases and deaths. Breast cancer is common cancer in Ethiopia [6].
Study Design, Area and Period
An institutional based cross sectional study was conducted from April 1 to 30, 2018 among undergraduate female students in Private Universities in west Arsi Zone. There five private universities: Leadstar University college, Kiamed University college, US university college, Rift Valley and Paradise Valley Universities were private universities in West Arsi Zone and 250km away from capital city of Ethiopia, Addis Ababa. They were upgraded to university at 2006 E.C. and had three faculties such as business, health science and engineering in regular and extension programs. The selected two universities (Rift Valley and Paradise) have 4,620 undergraduate students in all programs from these 2,217 were female students.
Sample Size Determination
The sample size was calculated using single population proportion sample size determination formula. We used 30.5% proportion to determine knowledge and 9.2% proportion to practice Fituma, 2015, with 95% CI, and 5% marginal error.
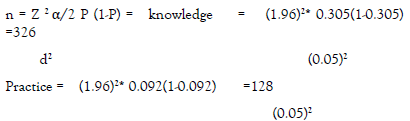
By adding 10 % contingency for non-respondent, the total sample size was 359.
Sampling Procedure
From five universities two universities (Rift valley and Paradise Universities) were selected randomly. The students were stratified into health and non-health student. The total sample size was allocated by using proportional allocation to size (PAS) to the total number of department from each strata. Then, the study subjects were selected by simple random sampling method by taking the list of female students in each department as a sampling frame.
Data Collection Tool
Data was collected by using pretested and structured questionnaire that were developed by reviewing related literatures and contain four parts socio-demographic, knowledge, perception or health belief constructs and practice through self-administered questionnaire. Afan Oromo and Amharic language versions of questionnaire were used for data collection purpose. Four diploma nurses who are confident in speaking Afan Oromo and Amharic were involved in the data collection. Also two BSc holder health professionals were recruited as supervisors.
Data Quality Control
The questionnaire was translated from English language to Afan Oromo and Amharic and back to English by other translator who was health professional to compare its consistency. For the instruments were developed after reviewing different literatures and modified in the area context, it was pretested on 5% of the total sample size and necessary adjustments was made on the questionnaire before it was used for actual data collection. The reliability of the questions was tested by Cronbach’s alpha and content validity was cross checked by another health professional.
Data collectors and supervisors were trained for two days on the study instrument and data collection procedure. The investigator and the supervisors were checked the collected data for completeness and corrective measures had been taken accordingly.
Data Analysis
The data was checked for completeness and consistencies, and then it was cleaned, coded and entered in to SPSS windows version 22. Descriptive statistics were computed to describe the study subject and determine the level of knowledge and practice of participants. Binary and multivariate analyses were constructed to examine the existence of relationship between the knowledge and practice of breast self-examination and selected covariates. Multivariate logistics regression analysis was applied using backward step wise method with p <0.05 and p > 0.25 criteria to enter and exit from the model respectively. Statistical significance was declared at P<0.05 and 95% CI. Odds ratios with 95% confidence intervals were computed and significance of all tests was determined at p ≤ 0.05.
Operational Definition
Breast self-examination: is a breast examination by women themselves to feel swelling, discoloration, discharge any change to their breast every months within 5-7 days of menstruation.
Knowledge of BSE: is knowledge of female about meaning of BSE, how to do and when to do BSE and measured by 6 multiple options question with right response 1 and wrong response zero.
Practice of breast self-examination: one who responds for question of breast self-examination practice yes and performing BSE every month.
Perceptions: it the way female beliefs about breast cancer and practice of breast self-examination and assessed by Likert scale containing the response from strongly disagree=1 to strongly agree=5 for each question.
Perceived severity: perception of the females as breast cancer is threatening and responds question to assess Perceived severity more than 50% after the responses were computed.
Perceived susceptibility: perception of females as they are more susceptible to breast cancer than other female and one who respond question prepared to assess Perceived susceptibility more than 50% after the responses were computed.
Perceived benefits: perception of females as they got benefit when they perform breast self-examination and one who respond question prepared to assess Perceived benefits more than 50% after the responses were computed.
Perceived barriers: perception of females towards the barriers of performing breast self-examination and one who respond question prepared to assess Perceived barriers more than 50% after the responses were computed.
Perceived confidence: perception of females being confident of performing breast self-examination and one who respond question prepared to assess Perceived confidence more than 50% after the responses were computed.
Perceived health motivation: perception of females about motivating factors about performing breast self-examination and one who respond question prepared to assess Perceived health motivation more than 50% after the responses were computed.
Ethical Consideration
An ethical clearance was obtained from ethical clearance committee of Madda Walabu University. Furthermore, letter of permission was found from Rift Valley and Paradise Valley universities, Shashemene campus. Written consent was obtained from each study subjects after explaining the objectives of study and procedures.
Socio-Demographic Characteristics
A total of 355 (146 health and 209 non health) study participants were participated in this study making response rate of 98.9 %. More than half of the participants 200(56.3) were at age category of 20-24 years and the mean age of the study population was 24 (SD±3.2) years. Regarding marital status 293 (82.5%) of the participants were single. Majority 228(64.2%) of the participants were Oromo by ethnicity and 169 (47.6 %) were Muslims. Majority of study participants 179 (47.9%), 170(41.4) heard about breast cancer from TV and health professionals respectively (Table 1).
| Variables | Frequency | Percentage |
|---|---|---|
| Age | ||
| 20-24 | 200 | 56.3 |
| 25-29 | 142 | 40.0 |
| ≥30 | 13 | 3.66 |
| Field of study | ||
| Healthy | 146 | 41.1 |
| Non health | 209 | 58.9 |
| Academic year of study | ||
| First year | 148 | 41.7 |
| Second year | 112 | 31.5 |
| Third year | 63 | 17.7 |
| Forth year and above | 32 | 9.0 |
| Marital status | ||
| Single | 293 | 82.5 |
| Married | 50 | 14.1 |
| Widowed | 12 | 3.4 |
| Participant having child | ||
| Yes | 37 | 59.7 |
| No | 25 | 40.3 |
| Religion | ||
| Muslim | 169 | 47.6 |
| Protestant | 82 | 23.1 |
| Orthodox | 74 | 20.8 |
| Catholic | 23 | 6.5 |
| Others | 7 | 2.0 |
| Ethnic group | ||
| Oromo | 228 | 64.2 |
| Amahara | 43 | 12.1 |
| Tigre | 30 | 8.5 |
| Gurage | 25 | 7.0 |
| Other* | 29 | 8.2 |
| Source of information | Frequency | Percentage |
| TV | 170 | 47.9 |
| Radio | 147 | 41.4 |
| Friends | 109 | 30.7 |
| Health professional | 170 | 41.4 |
| Reading book | 122 | 34.4 |
| Class lecture | 109 | 30.7 |
| Family | 88 | 24.8 |
Table 1: Socio-demographic characteristics of undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
Knowledge and Practices of Breast Self-examination
Knowledge of the participants about breast self-examination was assessed by six (6) multiple question with possible values ranging from 6 to 20 with the mean score of 14.18 (SD ± 5). From all participants 84(23.7%) were knowledgeable about breast selfexamination. Knowledge of participants about sign of breast cancer was assessed by seven yes/no questions and 148(41.7%) of them have knowledge about sign of breast cancer and Knowledge of participants about risk of breast cancer was assessed by nine yes/no questions 65(18.3%) of them have knowledge about risk of breast cancer. When we see the family history of breast cancer, 16(4.5%) of the respondents reported that they have previous family history of breast cancer. From all participants participated in study only 112(31.5%) ever practiced breast self-examination, from those 79(22.3%) of them practice breast self-examination monthly and most them started breast self-examination between age of 20-30 years. From those who practiced breast self-examination 46(41.1%) of participants performed breast self-examination for last time one week ago (Table 2 and Figure 1).
| Variables | Frequency | Percentage |
|---|---|---|
| Knowledge on sign of breast cancer | ||
| Knowledgeable | 148 | 41.7 |
| Not knowledgeable | 207 | 58.3 |
| Knowledge of risk of breast cancer | ||
| Knowledgeable | 65 | 18.3 |
| Not knowledgeable | 290 | 81.7 |
| Knowledge of participant about BSE | ||
| Knowledgeable | 84 | 23.7 |
| Not knowledgeable | 271 | 76.3 |
| Ever practice of breast self-examination | ||
| Yes | 112 | 31.5 |
| No | 243 | 68.5 |
| Time you practice breast self-examination | ||
| Monthly | 79 | 22.3 |
| Quarterly | 16 | 4.5 |
| Half a year | 4 | 1.1 |
| Yearly | 7 | 2.0 |
| Rarely | 6 | 1.7 |
| Age at participants started practice of breast Self-examination | ||
| At 20 years | 39 | 11.0 |
| At 20-30 years | 59 | 16.6 |
| At 30-40 years | 9 | 2.5 |
| Above 40 years | 5 | 1.4 |
| Participants practiced of breast self-examination in last 12 month | ||
| Yes | 106 | 94.6 |
| No | 6 | 5.4 |
| For last time when participants practiced breast self-examination | ||
| One week ago | 46 | 41.1 |
| One month ago | 41 | 36.6 |
| Three months ago | 16 | 14.3 |
| One year ago | 9 | 8.0 |
Table 2: Knowledge and practice of breast self-examination among undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
Regarding factors encourage the students to do breast self-examination practice; one thirds 37(33%) of the participants practiced breast self-examination due to media (Figure 1).

Figure 1. Factors motivate to perform breast self-examination among undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
Reasons not Performing Breast Self-examination
Majority of the students didn’t carry out breast self-examination since they haven’t known how they perform breast self-examination (Figure 2).

Figure 2. Reason of not performing breast self-examination among undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
Perception on Breast Self-examination
Perception of participants measured using health belief model constructs and treated as continuous variables. The six constructs (susceptibility, severity, barriers, benefits, self-efficacy and health motivation) were analyzed as a continuous variable with possible values ranging from 9 to 45 for severity with the mean score of 25.53(SD±8.47), from 5 to 25 for susceptibility with the mean score of 12.34 (SD±5.23), from 6 to 30 for barriers with the mean score of 16.18 (SD±6.34), from 7 to 35 for benefits with the mean score of 21.35 (SD±6.95), from 7 to 35 for selfconfidence with the mean score of 21.76(SD±7.81) and from 6 to 30 for health motivation with the mean score of 20.57 (SD±7.03) (Table 3).
| Variables | Frequency | Percentage | Mean(SD) |
|---|---|---|---|
| Perceived severity | 25.53(±8.47) | ||
| Yes | 168 | 47.3 | |
| No | 187 | 52.7 | |
| Perceived susceptibility | 12.34(±5.23) | ||
| Yes | 179 | 50.4 | |
| No | 176 | 49.6 | |
| Perceived benefit | 21.35(±6.95) | ||
| Yes | 282 | 79.4 | |
| No | 73 | 20.6 | |
| Perceived barriers | 16.18(±6.34) | ||
| Yes | 179 | 50.4 | |
| No | 176 | 49.6 | |
| Perceived confidence | 21.76(±7.81) | ||
| Yes | 186 | 52.4 | |
| No | 169 | 47.6 | |
| Perceived health motivation | 20.57(±7.03) | ||
| Yes | 183 | 51.5 | |
| No | 172 | 48.5 |
Table 3: Health belief construct to measure perception breast self-examination among undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
Factors Associated To Knowledge of Breast of Self- Examination
Multivariate analysis was done between socio-demographic variables, other independent variable and knowledge of breast self-examination by entering those all variables together such as, marital status, field of study, knowledge of participants about breast cancer risk factors, knowledge of participants about breast cancer sign and knowledge of participants about incidence then the results show that field of study, knowledge of participants about breast cancer risk factors, knowledge of participants about breast cancer sign and knowledge of participants about incidence were significantly associated with knowledge of breast selfexamination.
Female students those from health fields are more likely know about breast self-examination (AOR 2.15, CI 95% (1.23-3.76), students who know about sign and risk of breast cancer has more knowledge about breast self-examination than those who don’t know about sign and risk of breast cancer (AOR 3.073 95% C.I (1.545-6.114)] and [AOR 2.368, 95% C.I (1.196,4.688)] respectively (Table 4).
| Variables | Knowledge of BSE | Cor & 95% CI | AOR & 95% CI | |
|---|---|---|---|---|
| Knowledgeable | Not Knowledgeable | |||
| Field of study | ||||
| Health | 93 | 53 | 2.78(1.47,3.81) | 2.15(1.23,3.76) |
| Non health | 178 | 31 | 1 | 1 |
| Knowledge of BC sign | ||||
| Knowledgeable | 135 | 13 | 2.88 (1.19,6.00) | 3.073(1.545,6.114) |
| Not knowledgeable | 136 | 71 | 1 | 1 |
| Knowledge of BC risk | ||||
| Knowledgeable | 32 | 33 | 2.33(1.09,4.25) | 2.368(1.196,4.688) |
| Not knowledgeable | 239 | 51 | 1 | 1 |
Table 4: Multivariate analysis of variables knowledge of BSE among undergraduate female students in west Arsi zone, south east Ethiopia,, 2018.
AOR: adjusted for age, field of study, academic year of study, marital status, ethnic group religion, participant having child, source of information.
Factors Associated to Practice of Breast Self-examination
The variables those candidates for multivariate analysis during bivariate analysis such as, field of study, marital status, knowledge of breast self-examination study, knowledge of sign of breast cancer, and from constructs of health belief model perceived susceptibility, perceived barriers and self-confidence were assessed for association to practice of breast self-examination, but only few variables such as knowledge of breast self-examination, field of study, perceived susceptible and perceived barriers were associated. Also, the results of multivariate analysis show that undergraduate female students who has knowledge about breast self-examination 3.16 times more practice breast self-examination than who don’t know about breast self-examination [AOR 3.163 95% C.I (1.794-5.577)]. From constructs of health belief model the participants who perceived they are susceptible for breast cancer are 2.15 times more likely to practice breast self-examination [AOR 2.154 95% C.I (1.220- 3.804)] and those who not perceive about the barriers of breast self-examination are less likely to practice breast self-examination [AOR 1.787 95% C.I PV 0.047(1.008-3.168)] (Table 5).
| Variables | Practice of BSE | COR, 95% CI | AOR, 95% CI | |
|---|---|---|---|---|
| Yes | No | |||
| Knowledge about BSE | ||||
| Knowledgeable | 45 | 39 | 3.513(2.110,3.706) | 3.163 (1.794,5.577) |
| Not knowledgeable | 67 | 204 | 1 | 1 |
| Perceived susceptibility | ||||
| Yes | 44 | 135 | 1.932(1.225,3.048) | 2.154 (1.220,3.804) |
| No | 68 | 108 | 1 | 1 |
| Perceived barriers | ||||
| Yes | 45 | 134 | 1.830(1.162,2.884) | 1.787 (1.008,3.168) |
| No | 67 | 109 | 1 | 1 |
Table 5: Multivariate analysis of variables of practice BSE among undergraduate female students in west Arsi zone, south east Ethiopia, 2018.
The American cancer society guidelines for the early detection of cancer and Ethiopian federal ministry of health cancer prevention guideline state that women should know how their breasts normally look and feel and report any breast change promptly to their health care provider. Breast self-examination is an option for women starting in their 20s. This study show that from all participants 84(23.7%) were knowledgeable about breast selfexamination, this results almost consistent with a study done at Debra Berhan university [7]. Ambo University Natae, 2015 and Mekele town [8], but higher than a study done at Adama science and technology university students [9]. The difference may be due to study participants composition and their level of knowledge about breast self-examination. The study reveal that from all participants participated in the study only 112(31.5) ever practiced breast self-examination, from those 79(22.3) of them practiced breast self-examination monthly and most of them started breast self-examination between age of 20-30 years. This result almost agrees with the study done in Ambo University that reported, only 63 (20.7%) participants practiced BSE. Of the participants who practiced BSE, 28 (44.4%) practiced BSE monthly 23 (36.5%) were practiced once every three month, 6(9.5%) and 6(9.5%) were practiced once quarterly and never once yearly respectively. A study done at Rift Valley University Adama campus revealed that 25.8% of participants had practiced breast examination [10,11,18].
The results of multivariate analysis showed that under graduate female students who has knowledge about breast self-examination 3.16 times more practice breast self-examination than who didn’t know about breast self-examination [AOR 3.163 95% C.I (1.794- 5.577)]. From constructs of health belief model the participants who perceived they are susceptible for breast cancer were 2.15 times more likely to practice breast self-examination [AOR 2.154 95% C.I (1.220-3.804)]. A study done in Debra Berhan University show that the predictor factors of practicing BSE were knowing how to perform BSE, knowing when to perform BSE, knowing the three positions to perform BSE, and believing that BSE is important and useful to detect breast cancer [12,14], but a study done in Kafa zone explained that all constructs of health belief model were significantly associated with BSE. However, after controlling for possible confounding factors, the result showed that per a unit increases in total score of perceived susceptibility and severity towards breast cancer the odds of performing BSE increased. As an study done in Ambo University showed that majority of the respondents did not know that BSE can early detect the problem of breast, only one fifths of participants practiced BSE [13]. Study done at Debra Birhan University on undergraduate female students show that 64% of the participants had heard of BSE and 35.8% of the participants knew how to perform BSE. Furthermore, one thirds of participants were aware when to perform BSE. The main sources of information were mass media 39.8% and health professions 22.3%. Overall, 37.3%, 32.5%, and 30.25% of the study participants had poor <50%, medium 50–75%, and good knowledge >75 on BSE, respectively [11,16,17].
Generally, under graduate female student’s knowledge about breast self-examination was 23.7% and practice of regular monthly breast self-examination was 22.3%. Therefore, both knowledge and practice of breast self-examination of undergraduate female students were low as a National guideline of Ethiopia FMOH that states all female age above 20 years should practice BSE. The most reason of not practicing breast self-examination was don’t know how to do breast self-examination (53.09%).
Ethics Approval and Consent to Participate
The study was done by interviewing female college students after an ethical consent was obtained from Madda Walabu University ethical clearance committee and individual verbal consent was obtained from the study participants. Regarding the minors, consent to participate was found from their parents on their behalf. This manuscript has never been submitted and deliberated for publication to any other journal.
Consent for publication
Not applicable.
Availability of supporting data
Data will be available upon request.
Competing interests
The authors have no any competing interest and all have agreed the manuscript for publication.
Funding
This study has no specific funding.
Authors’ contributions
All authors have equal contribution to the manuscript. All authors critically reviewed the manuscript, read and approved the final manuscript.
Authors' information
HA is MCH coordinator at Shashemene hospital, KH and AL are assistant professors at Madawalabu University, AA and TE are lecturers at Madawalabu University.
Authors are grateful to Madawalabu University for supporting this study. We are also very grateful to study participants and data collectors for their cooperation to undertake this study.
Citation: Kedir H, Ahmed K, Abdulkadir A, Ermeko Wanamo T, Lette A (2021) Knowledge and Practice Of Breast Self-examination and Associated Factors Among Women Students in West Arsi Zone, Southeast Ethiopia. J Women's Health Care 10:542. doi:10.35248/2167-0420.21.10.542.
Received: 01-Jul-2021 Accepted: 14-Jul-2021 Published: 21-Jul-2021
Copyright: © 2021 Kedir H, et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original work is properly cited.