Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
![]() +44 1478 350008
+44 1478 350008
ISSN: 2165-7092
![]() +44 1478 350008
+44 1478 350008
Research Article - (2015) Volume 5, Issue 2
Aim: Aim of this study is to compare the results of laparoscopic suture vs stapler cystojejunostomy for pseudocyst of pancreas. Materials and Methods: In this retrospective study of 18 patients including both male and female of age ranging from 15 to 64 years were subjected to laparoscopic cystojejunostomy from April 2007 to july 2013, of which 13 patients underwent suture cystojejunostomy and 5 patients underwent stapler cystojejunostomy. These patients were followed for a period of 18 months assessing first bowel movement, duration of surgery, hospital stay, anastomosis leak, recurrence and morbidity. Result: Duration of surgery was 156.6 ± 10.4 minutes in laparoscopic suture cystojejunostomy and 122 ± 8.8 min in laparoscopic stapler cysto-jejunostomy. Postoperatively, the mean time for the first bowel movement was 36 hrs and 39 hrs, respectively, for suture and stapler cystojejunostomy. Mean hospital stay was six (range: 5-7) days. There was postoperative complication in the form of anastomosis leak that occurred in two patients in stapler cystojejunostomy group. There was no leak in suture group. There were no recurrences. Morbidity was greater in stapler group as leak occurred in two patients. Conclusion: We conclude that laparoscopic suture cystojejunostomy is a safe and feasible procedure and gives superior results in regards to safety of anastomosis and its resultant morbidity. Suture cystojejunostomy is also comparable to stapler in regards to operative time, bowel function and recurrence.
<Keywords: Cystojejunostomy, Suture, Stapler, Pseudocyst
Management of pseudopancreatic cyst ranges from observation to endoscopic methods and open/laparoscopic surgery. Laparoscopic surgery can be successfully used to treat pancreatic pseudocyst [1]. Most commonly performed procedure is drainage procedure. Drainage procedures include cystogastrostomy, cystojejunostomy and cystoduodenostomy. In drainage procedures, anastomosing cyst wall with jejunum can be done with an endo-stapler or with intra-corporeal suturing. Stapler anastomosis saves time and is easier to create than intra-corporeal suturing. Intra-corporeal suturing is difficult to perform and takes time. Post-operative morbidity includes anastomosis leak, recurrences, hematemesis etc [2]. So here we present a comparative study between stapler and suture anastomosis for cystojejunostomy.
In this retrospective study of 18 patients including both male and female of age ranging from 15 to 64 years were subjected to laparoscopic cystojejunostomy from April 2007 to july 2013, of which 13(70%) patients underwent suture cystojejunostomy and 5(30%) patients underwent stapler cystojejunostomy. In this study, only one pediatric patient of age 15 years was included in the suture group, rests of the patients were adults. All the surgeries were performed by a single surgeon. Acute pancreatitis was found to be etiological factor in 16 (90%) patients and blunt trauma abdomen was the etiology in 2(10%) patients. Size of pseudocyst ranged from 8 cm to 15 cm in largest dimension and all pseudocysts were located in tail of pancreas. All patients were investigated thoroughly with Ultrasound, Computerized Tomography scan and Magnetic Resonance Cholangiopancreatography. All patients were put for surgery with minimum 2 months after incidence of their etiological factor, so as to give adequate time for maturation of cyst wall. Pre-anesthetic checkup was done and fit patients were put for surgery.
Under general anesthesia, patients were put in modified lithotomy position. Pneumoperitoneum created using veress needle. Port positions were as follows- one 12 mm supraumbilical port, one 10 mm telescopic port- 3 cm lateral to the first port in right side, two 5 mm ports on either side in mid clavicular line in hypogastric region and one 5 mm port was placed 3 cm below left 5 mm port. Pseudo-cyst was identified in lesser sac and it was found to be totally free from stomach in all patients, so cystojejunostomy was contemplated instead of cystogastrostomy. All the mesenteric attachments of cyst were divided with harmonic scalpel, making its antero-inferior part bare for anastomosis. Cyst cavity was perforated and cyst fluid was aspirated and sent for culture & sensitivity and amylase levels. Cyst wall biopsy was taken and sent for histopathological examination. Jejunal limb was divided 25 cm from duodenojejunal junction, using linear stapler. Cystojeunostomy was done with the efferent jejuna limb, using non-absorbable suture in single layer, using intra-corporeal suturing technique. Jejunojejunostomy was done using linear stapler. Adk tube drain given in morrisons pouch. All ports were closed (Figures 1 and 2).
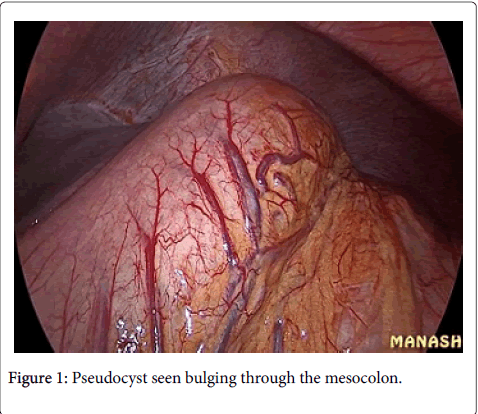
Figure 1: Pseudocyst seen bulging through the mesocolon.
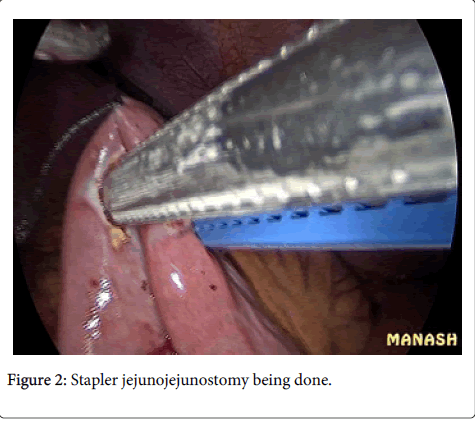
Figure 2: Stapler jejunojejunostomy being done.
Post op period- Patients were started oral liquids on the third day and gradually solid food was resumed. Drain was removed on 5th day. Sutures were removed on the third day. Patients were discharged on 6th to 8th day. Anastomotic leak occurred in two patients in stapler group on 5th and 6th day which was identified first by clinical examination in the form of increased abdominal tenderness and increase in drain output and confirmed by ultrasound. Both patients were successfully managed by laparoscopic toileting and intra-corporeal suturing of leaked part (angle) of cystojejunostomy with non-absorbable suture. Both patients recovered fully and their post op period was uneventful. In all patients, follow up ultrasound and Computerized Tomography Scan was done at 3 months, 6 months, 12 months and 18 months after surgery, revealing no recurrences (Figures 3 and 4).
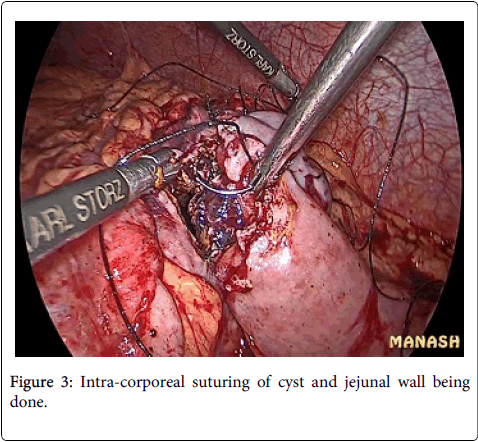
Figure 3: Intra-corporeal suturing of cyst and jejunal wall being done.
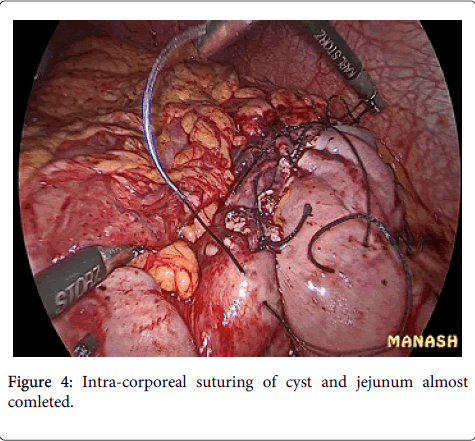
Figure 4: Intra-corporeal suturing of cyst and jejunum almost comleted.
Duration of surgery was 156.6 ± 10.4 minutes in laparoscopic suture cystojejunostomy and 122 ± 8.8 min in laparoscopic stapler cystojejunostomy. Postoperatively, the mean time for the first bowel movement was 36 hrs and 39 hrs, respectively, for suture and stapler cystojejunostomy. Mean hospital stay was six (range: 5-7) days, except for 2 cases which leaked (hospital stay was 13 and 14 days). There was no leak in suture group. There were no recurrences in any group. Morbidity was greater in stapler group as leak occurred in two patients. The cost of treatment was significantly higher in stapler group as patients had to buy stapler endo-cartridges. This cost further got increased in two patients in which leak occurred. Therefore suture proved to be a more cost-effective option than stapler. The confidence interval for this study is 95%. P-value of leak in stapler group has been calculated as 0.0067 and found to be significant. Also operative time, hospital stays and first bowel movement was also found to be significant (Table 1 and Table 2).
| Suture group(n-13) | Stapler group(n-5) | p-value | |
| Age | 41.2 (MEAN) | 43.6 (MEAN) | 0.3616 |
| Gender | |||
| Male | 10 | 4 | |
| Females | 3 | 1 | |
| Co-morbidities | |||
| Cardiovascuolar | 1 | ||
| Diabetes | 1 | ||
| Others | |||
| Size of the pseudocyst | 10.84 (MEAN) | 12.4 (MEAN) | 0.092 |
Table 1: Clinico-pathological features.
| Suture group(n-13) | Stapler group(n-5) | p-value | |
| Operative time | 156.6 (Mean) | 122 (Mean) | 0.00001 |
| Hospital stay | 6 (Mean) | 9 (Mean) | 0.0107 |
| First bowel movement | 36 (Mean) | 39 (Mean) | 0.0277 |
| Complications-Anastomosis leakage | 0 | 2 | 0.0067 |
Table 2: Post-operative outcome.
Pseudocyst of pancreas is a fluid collection contained within a well-defined capsule of fibrous or granulation tissue or a combination of both. They do not possess an epithelial lining. Pseudocyst of pancreas most commonly occurs as a complication of acute or chronic pancreatitis. They are present in 10-20% of cases in acute pancreatitis and in 30% cases in chronic pancreatitis [3]. Most common etiology includes gallstone and alcohol in adults and abdominal trauma in pediatric age group [4]. Most common presentation includes no symptoms, vague upper abdominal pain, nausea and vomiting, flatulent dyspepsia, lump in abdomen, pleural effusion. Diagnosis is usually suggested by ultrasound and confirmed by Computerised Tomography Scan and Magnetic Resonance Cholangiopancreatography. Management includes observation which is advised in most pseudocysts for initial 6 weeks in hope of spontaneous resolution. Spontaneous regression of asymptomatic pseudocyst following attack of acute pancreatitis occurs in 30-60% cases [5]. It takes usually 4-6 weeks for cyst wall to mature by replacement of granulation tissue with fibrous tissue. But complication rate increase by 50% after 6 weeks, which includes infection, pseudoaneurysm, bleeding and obstruction6. Ultrasound guided or Computerised Tomography guided percutaneous drainage can also be done, but has significant complications including bleeding, infection and high recurrence rate [6]. Endoscopic drainage includes creating a tract between stomach and cyst wall and putting a stent in between, its main drawback is lack of clearance of necrotic material leading to recurrences. Laparoscopic method is gaining popularity as it is minimally invasive and has ability to clear all necrotic material. Laparoscopic surgery for the pancreatic pseudocyst was introduced by Way et al. [7]. Laparoscopic cystogastrostomy and cystojejunostomy are most commonly performed procedures. Cystojejunostomy can be performed with staplers or sutures. For stapler one 12mm port is needed but is easier to perform and saves time. Intracorporeal suturing is difficult to perform and takes time. But thick walled pseudocyst may not be amenable to stapler anastomoses. In suture cystojejunostomy, angle can be reinforced with an extra 2-3 sutures, which was the site of leakage in our study. In our series, two cases of stapler anastomoses group leaked while there was no leakage in suture anastomosis group. Most probable explanation of leak in stapler group is unevenness of thickness of cyst wall which was anastomosed with jejunum. All patients in our study had well-formed cyst wall as minimum 8 weeks had passed before patients were put for surgery and cyst wall thickness was also confirmed by Computerized Tomography Scan preoperatively.
This trial found that laparoscopic suture cystojejunostomy is a safe and feasible procedure and gives superior results in regards to safety of anastomosis and its resultant morbidity. Suture cystojejunostomy is also comparable and in some parameters better than stapler cystojejunostomy.