Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2018) Volume 8, Issue 3
Objectives: To remind the epidemiology, the diagnosis and the surgical aspects of laparoscopic management of giant ovarian cysts at the Gynecology and Obstetrics Department of Ouakam Military Hospital.
Materials and methods: This is a prospective and descriptive study carried out during 2 years, from February 1st 2015 to January 31st 2017 at the Gynecology and Obstetrics Department of Ouakam Military Hospital. It involved all patients who had undergone laparoscopic surgery for an ovarian cyst which measures 15 cm or more. The parameters studied were the patient's socio-demographic characteristics, the clinical symptomatology, ultrasound and/or CT scan results, surgical data, the histological nature of the cyst and the length of hospital stay. Data was captured and analyzed by Excel.
Results: Patients' age ranged from 13 to 41 years with an average of 27.1 years. Physical examination had shown an abdominal mass in all patients. Imaging examinations (ultrasound and/or CT scan) found an ovarian cystic mass that varied in size from 15 to 27 cm with an average of 20 cm. Only one patient (9.1%) had a rate of CA 125 above the threshold. Laparoscopy confirmed the diagnosis of all patients. We performed 9 cystectomies (81.8%) and 2 adnexectomies (18.2%). The procedure lasted in average 72 min with extremes of 50 and 90 min. The surgical follow-up was simple and the discharge was authorized 3 days after surgery. The histological examination of the surgical specimens performed in all patients revealed 3 serous cystadenomas (27.3%), 3 dermoid cysts (27.3%), 3 endometriomas (27.3%) and 2 mucinous cystadenomas (18.2%).
Conclusion: Laparoscopy should be indicated to treat giant ovarian cysts. Ultrasound and CT scan allow making good selection of cases for this approach.
Keywords: Giant ovarian cyst; Laparoscopic surgery; Cancer
Giant ovarian cysts are less and less common today because of the development of the sanitary system making early diagnosis and management easier [1]. However, this pathology, in decline in the developed countries, is still relevant in our developing countries where there is often a delay in consultation and diagnosis. Their laparoscopic management is very controversial because of the potential risk of malignancy but also technical difficulties. Through an analysis of the cases operated at the Service of Gynecology-Obstetrics of the Military Hospital of Ouakam and a review of the literature, we recall the epidemiological, diagnostic and operative aspects in the laparoscopic management of giant ovarian cysts.
This was a prospective and descriptive study conducted over a period of 2 years from February 1st, 2015 to January 31st, 2017 at the Department of Gynecology and Obstetrics of the Military Hospital of Ouakam. It concerned all patients who had had laparoscopic surgery for an ovarian cyst greater than or equal to 15 cm.
The parameters studied were the sociodemographic characteristics of the patients (age, parity), the clinical symptomatology, the results of the ultrasound and/or the CT scan (cyst size, wall thickness, uni or multilocular character, ascites and vegetations), operative data (exploration, performed gesture, possible complications, duration of the intervention), the histological nature of the cyst and the length of the hospital stay. The data was recorded and analyzed by the Excel software.
Surgical technique
The approach used was laparoscopy for all patients. They had a digestive preparation the day before the surgery. The intervention was done under general anesthesia. The patient was supine with her legs semi-flexed and her right arm down. The approach was open laparoscopic with a 12 mm trocar inserted through two fingers above the umbilicus. The insufflation pressure was limited to 15 mmHg. Then a 5 mm trocar was placed under visual control at the contralateral iliac fossa at the cyst site, two fingers across the anterior superior iliac spine.
The first stage of the surgery was an exploration of the abdominopelvic cavity for diagnostic purposes. In case of suspicious lesion of malignancy, a conversion to laparotomy was performed. In the opposite case, the monopolar tip and the suction cannula successively allowed the cyst to be punctured and the contents aspirated to reduce its size. Two more 5 mm trocars were then inserted into the ipsilateral iliac fossa at the cyst site and midway between the umbilicus and the pubic symphysis. Cystectomy was performed by divergent traction, step by step, until complete removal of the cyst envelope. The operative piece’s extraction was done in a condom through the trocar of 12 mm, a 5 mm optics being introduced through one of the trocars of 5 mm. The abdominal and pelvic cavity was lavishly washed with the patient in a proclive position before exsufflation and closure of the trocar orifices. All operative specimens were examined histologically.
Frequency
During the study period, 43 patients underwent laparoscopic surgery for benign ovarian cyst. Of these, 11 (25.6%) had a giant ovarian cyst.
Characteristics of the patients
The average age of the patients was 27.1 years with extremes of 13 and 41 years. Ten of them (90%) were nulliparous. The interrogation found pelvic heaviness in 8 patients (72.7%) and 2 of them (18.2%) had dyspnea. The physical examination had demonstrated an abdominopelvic mass in all patients. Imaging examinations (ultrasound and/or computed tomography) revealed 7 multilocular tumors (63.6%) (Figures 1A and 1B), one bilocular (9.1%) and 3 unilocular tumors (27.3%) Only one patient (9.1%) had an abovenormal CA 125 level (Table 1).
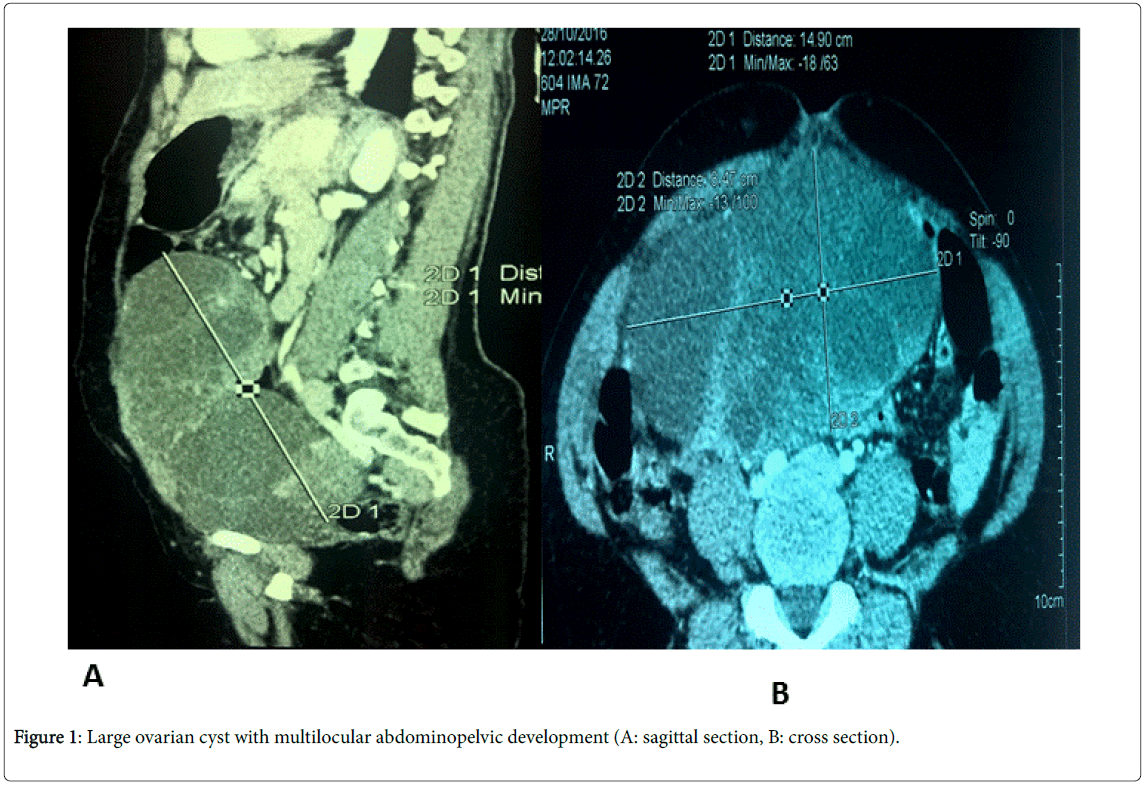
Figure 1: Large ovarian cyst with multilocular abdominopelvic development (A: sagittal section, B: cross section).
| # | Age (year) | Parity | Symptoms | Ultrasound - CT scan (characteristics and size of the cyst) | CA 125 (UI/L) |
|---|---|---|---|---|---|
| 1 | 17 | 0 | Pelvic heaviness | Unilocular, pure liquid, thin wall, 15 cm | 29,3 |
| 2 | 35 | 0 | Pelvic heaviness | Unilocular, pure liquid, thin wall, 17 cm | 24,72 |
| 3 | 25 | 0 | Metrorrhagia, chronic pelvic pain | *Bilocular, thick wall, 19 cm | 10,61 |
| 4 | 13 | 0 | abdominal distension, pelvic heaviness, dyspnea | *Multilocular, mixed predominantly solid, thick wall, ascites blade, 25 cm | 6,46 |
| 5 | 27 | 0 | abdominal distension, pelvic heaviness | Multilocular, mixed predominantly solid, thick wall, 23 cm | 20,3 |
| 6 | 34 | 0 | Chronic pelvic pain | Multilocular, thick wall, 18 cm | 32,64 |
| 7 | 30 | 0 | Pelvic heaviness | Multilocular, mixed predominantly solid, thick wall, 21 cm | 18,5 |
| 8 | 15 | 0 | Pelvic heaviness, polymenorrhoea, dyspnea | *Multilocular, pure liquid, thin wall, 27 cm Urétéro-hydronéphrose |
63,5 |
| 9 | 26 | 0 | Pelvic heaviness | Multilocular, pure liquid, thick wall, 16 cm | 27,5 |
| 10 | 41 | 0 | Acute pelvic pain | Multilocular, pure liquid, thick wall, 17 cm | 23 |
| 11 | 36 | 2 | Pelvic heaviness | Unilocular, pure liquid, thin wall, 22 cm | 21,52 |
*CT scan
Table 1: Characteristics of the patients.
Per and post-operative data
Laparoscopy confirmed the diagnosis in all patients, two of whom (18.2%) had pelvic adhesions on exploration. We performed 9 cystectomies (81.8%) and 2 adnexectomies (18.2%). The intervention lasted on average 72 min with extremes of 50 and 90 min. The operative follow-up was simple and the exit was allowed 3 days after the surgery. Histological examination of operative specimens performed in all patients revealed 3 serous cystadenomas (27.3%), 3 dermoid cysts (27.3%), 3 endometriomas (27.3%) and 2 mucinous cystadenomas (18.2%) (Table 2).
| # | Laparoscopic exploration | Surgical gesture | Length of the intervention (min) | Histology | Length of hospital stay (days) |
|---|---|---|---|---|---|
| 1 | Left ovarian cyst Right ovarian dystrophy |
Cystectomy Ovarian drilling |
50 | Serous cystadenoma | 3 |
| 2 | Right ovarian cyst, utero-sigmoid adhesions | Cystectomy, adhesiolysis | 68 | Endometrioma | 3 |
| 3 | Left ovarian cyst Utero-ovarian adhesions |
Cystectomy, adhesiolysis |
75 | Endometrioma | 3 |
| 4 | Right ovarian cyst | Cystectomy | 80 | Dermoid cyst | 3 |
| 5 | Left ovarian cyst | Cystectomy | 85 | Dermoid cyst | 3 |
| 6 | Right ovarian cyst | Cystectomy | 55 | Endometrioma | 3 |
| 7 | Left ovarian cyst | Cystectomy | 90 | Dermoid cyst | 3 |
| 8 | Right ovarian cyst | Adnexectomy | 87 | Mucinous cystadenoma | 3 |
| 9 | Left ovarian cyst | Cystectomy | 60 | Serous cystadenoma | 3 |
| 10 | Right ovarian cyst | Adnexectomy | 60 | Mucinous cystadenoma | 3 |
| 11 | Left ovarian cyst | Cystectomy | 80 | Serous cystadenoma | 3 |
Table 2: Per and post-operative data and histological types.
Giant ovarian cysts are rare and their frequency is variously appreciated according to the authors [2,3]. This variability of frequency is probably due to definitions that differ from one series to another. They range from ovarian cysts larger than 10 cm to those extending above the umbilicus [4]. For Dolan et al. [2], the size of the peritoneal cavity should also be taken into account, especially if it is a young patient during a period of growth. These cysts are most often found in women of childbearing age [5], rarely before puberty or after menopause. In our series, we made the same observation. The symptomatology is dominated by pelvic heaviness and abdominal distension. In the abdominopelvic forms, we can note mass effects such as diaphragmatic compression at the origin of dyspnea and compression of the inferior vena cava or the ureter responsible respectively for stasis edema lower limbs and uretero-hydronephrosis. In our series, two patients (18.2%) with cysts 25 and 27 cm long had dyspnea. Due to the associated abdominal distension, giant ovarian cysts can mislead an ascites of great abundance [3]. Ultrasound and computed tomography (CT scan) allow to make the diagnosis by specifying the size and the characters of the cyst which direct towards the type and the benign or malignant nature. Indeed, the thickness of the wall, the uni or multilocular character, the presence or absence of intra or extra-cystic vegetations and ascites are all criteria that guide the nature of the tumor. Tumors suspected of malignancy are those that are predominantly solid, multicleafed with a wall thickness greater than 2 mm, thick walled and hypervascularized with Doppler. The risk of malignancy is higher in the post-menopausal period and in cases of bilateral cysts. Computed tomography also makes it possible to better specify tumor ratios with neighboring organs and to perform an extension assessment in the event of a malignant tumor [3]. The determination of CA 125 does not make it possible to affirm or deny the malignant nature of the tumor. Indeed, some benign tumors such as endometriomas are often associated with a significant increase in CA 125 levels.
Giant ovarian cysts are benign in 70% of cases and can be purely fluid or mixed. It may be a serious, mucinous, dermoid or endometriotic cyst [6-8]. In the series of Diop [5] and Alobaid [4], there was a predominance of serous and mucinous types. The same observation was made in our series and in the literature in which we note that mucinous cystadenomas are benign in 75% of cases, borderline in 10% of cases and malignant in 15% of cases [9-11]. This malignant potential, although low, poses the problem of the surgical approach. While some authors chose laparotomy [5,12], others [4,13], as was our case, preferred laparoscopy. The latter allows a complete and reliable exploration of the abdominopelvic cavity to evaluate the risk of malignancy. Indeed, in a study by Canis [5,12], it was proved that in cystic adnexal masses, the negative predictive value of the laparoscopic diagnosis of malignancy was 100%. This reinforces our choice of laparoscopy as a first-line approach for the management of giant ovarian cysts. When a suspicious lesion is found in the diagnostic time of laparoscopy, laparotomy should be performed. This approach would treat the majority of giant ovarian cysts laparoscopically and therefore reduce the postoperative prescription of analgesics and the risk of deep vein thrombosis by early mobilization. It also offers other benefits in terms of reducing the length of hospital stay and early return to normal activity [4].
However, some technical difficulties are associated with the laparoscopic management of giant ovarian cysts. These include the extraction of the often voluminous surgical specimen and the risk of dissemination of tumor cells in borderline or malignant tumors. To overcome these obstacles some technical devices were proposed. Indeed, in the Quilian series [13], cysts were extracted through the opening of a 10 mm trocar after morcellation or by a posterior colpotomy. After 4 years, he had not objectified cases of recurrence or spread of the tumor. In our series, all the surgical pieces were extracted inside a condom through a 12 mm trocar. The average duration of follow-up of our patients was 2 years and we did not notice any recurrence. Other authors [14,15] who had used this fragmentation technique had made the same observation. However, all these studies were characterized by a relatively short duration of patient follow-up, whereas a larger retreat is necessary for an objective assessment of the risk of dissemination and recurrence of the tumor after morcellation. After cyst extraction, an abundant toilet of the abdominal-pelvic cavity with 1 to 4 liters of isotonic saline would also reduce the risk of tumor cell dissemination. This measure is particularly recommended for mucinous or dermoid cysts [16].
Giant ovarian cysts are a rare condition occurring in young women during periods of genital activity. Histological types are dominated by serous and mucinous cysts. Their laparoscopic management requires a good selection of patients by ultrasound and computed tomography to exclude cases of suspected malignancy that fall under laparotomy.