Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 2
Objective: To report a case of large remnant ablation in a patient with metastatic papillary thyroid carcinoma.
Methods: We present the initial presentation, radiologic findings and subsequent surgical and medical management. The pertinent literature and management options are also reviewed.
Results: A previously healthy 80 year old woman presented to clinic with a large right-sided neck mass of several years duration. Fine needle aspiration biopsy was consistent with papillary thyroid carcinoma. Pre-operative CT imaging noted a 6cm by 6cm mass, extending into the mediastinum with mediastinal lymphadenopathy and numerous bilateral pulmonary nodules. She underwent tumor resection, however the left thyroid was left in place because the tumor extended retrosternally, and no plane could be established between the tumor and the larynx. She received 31.9 mCi of I-131 for ablation of the remaining left thyroid lobe four months later. Repeat CT imaging four months after the initial dose of I-131 showed regression of the mediastinal lymphadenopathy and pulmonary nodules, with the exception of one nodule in the right lower lobe. Approximately nine months after receiving the initial dose of I-131, she received 158.5 mCi I-131 for remnant ablation. CT imaging six months following I-131 remnant ablation noted interval increase in size of the nodule in the right lower lobe of her lung, but was otherwise unchanged from her previous CT.
Conclusion: This case illustrates the use of radioactive iodine for ablation of a large thyroid remnant when total thyroidectomy is not an option in the management of metastatic papillary thyroid carcinoma.
<Keywords: Metastatic papillary thyroid carcinoma; Radioactive iodine; Large remnant ablation
CT: Computed Tomography; I-131: Radioiodine
Surgery remains the mainstay for treatment of differentiated thyroid carcinoma. Total or near-total thyroidectomy followed by radioiodine (I-131) ablation of residual thyroid tissue is the recommended treatment for high-risk disease, including those patients with macroscopic tumor invasion and distant metastases [1]. However, total or near-total thyroidectomy is not always possible, especially in patients with extensive or locally invasive tumor. As an alternative, large remnant ablation may be considered. There is little evidence regarding the use of I-131 to ablate the remaining thyroid lobe in locally invasive disease.
A previously healthy 80 year old woman presented to the outpatient Otorhinolaryngology clinic with a large, right-sided neck mass of several years’ duration. Fine needle aspiration biopsy was consistent with papillary thyroid carcinoma. On Computed Tomography (CT) imaging, the mass measured at least 6 cm by 6 cm, extending inferiorly into the paratracheal mediastinum, and displacing the common carotid posteriorly, with possible invasion of the right internal jugular vein (Figure 1A). Imaging also noted extensive mediastinal lymphadenopathy (Figure 1B), as well as numerous bilateral pulmonary nodules, all suggestive of metastatic disease. She underwent tumor resection with modified radical neck dissection. Intraoperatively, the tumor was found to be adherent to the larynx, trachea and carotid artery. Because the tumor extended retrosternally, and no plane could be established between the tumor and the larynx, the tumor was transected in the main portion of the right thyroid lobe and the left thyroid lobe was left in place. After surgery, she completed a two-week course of external beam radiation and was referred to Endocrinology for further management. Post-operative imaging revealed the presence of the left thyroid lobe which was left in place, in addition to extensive remnant tissue around the trachea and esophagus. The decision was made to give her a low radioactive iodine dose to ablate those remnants without causing significant morbidity. This would be followed, if tolerated, by a larger dose a few months down the road.
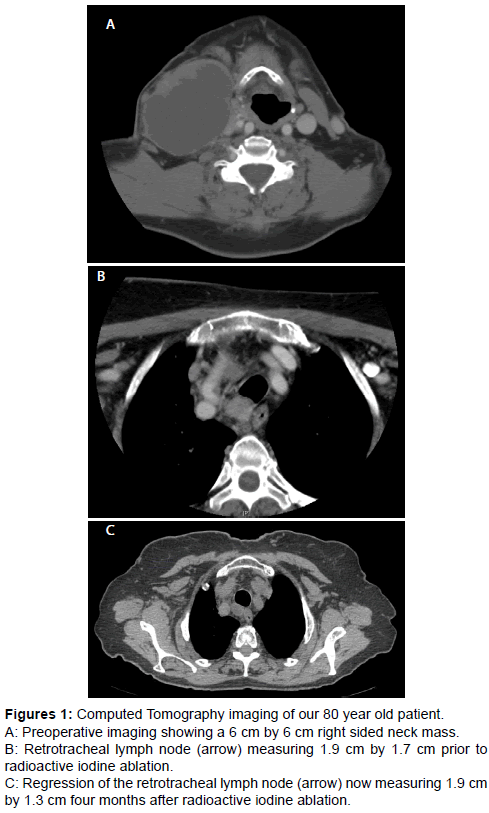
Figure 1: Computed Tomography imaging of our 80 year old patient.
A: Preoperative imaging showing a 6 cm by 6 cm right sided neck mass. B: Retrotracheal lymph node (arrow) measuring 1.9 cm by 1.7 cm prior to radioactive iodine ablation.
C: Regression of the retrotracheal lymph node (arrow) now measuring 1.9 cm by 1.3 cm four months after radioactive iodine ablation.
Subsequently, approximately four months after her surgery, she received 31.9 mCi of I-131 for ablation of the remaining functioning left thyroid lobe. At that time, her thyroglobulin level was 3.5 ng/mL. She subsequently became hypothyroid, and was started on levothyroxine. Repeat CT imaging four months after the initial dose of I-131 showed regression of the mediastinal lymphadenopathy and pulmonary nodules (Figure 1C), with the exception of one nodule in the right lower lobe which increased in size from 0.8 cm by 0.6 cm to 0.9 cm by 0.8 cm. Her unstimulated thyroglobulin level became undetectable. Approximately nine months after receiving the initial dose of I-131, she received 158.5 mCi I-131 for remnant ablation after thyrotropin alfa administration. CT imaging six months following I-131 remnant ablation noted interval increase in size of the nodule in the right lower lobe of her lung, but was otherwise unchanged from her previous CT. Her unstimulated thyroglobulin level was 0.8 ng/mL. Further follow-up revealed stability of the lung nodules and given her age and good overall functional status, and after consultation with a medical oncologist, the patient decided to continue surveillance (as opposed to starting a tyrosine kinase inhibitor), with the possibility to revisit that option in the future should her clinical condition deteriorate. She remains stable to that day, two years after surgery.
The incidence of thyroid carcinoma continues to increase [1]. It is estimated that 60,220 new cases of thyroid carcinoma will be diagnosed in 2013 [2]. Papillary thyroid carcinoma accounts for approximately 85% of well-differentiated thyroid carcinoma [1]. While papillary thyroid carcinoma is generally indolent, metastatic thyroid carcinoma presents a difficult situation, especially when total or near-total thyroidectomy is not possible. Typically, I-131 ablation is employed as adjunct therapy, following surgery because normal thyroid tissue has higher iodine avidity when compared to tumor.
In our patient, total thyroidectomy was not possible due to the extent of tumor invasion into the neck structures and mediastinum. There have only been a few studies using I-131 ablation as an alternative to total thyroidectomy, and even less regarding its use in metastatic carcinoma. In one study, 19 patients had a hemithyroidectomy for differentiated thyroid cancer without metastasis, and were given I-131 for large remnant ablation. The success rate for ablation was only 28% after a mean dose of 141.3 mCi of I-131, compared to 80% success in patients with smaller remnants after near-total thyroidectomy [3]. In a larger study of 46 patients, 33-47% with malignancy in remnant tissues, 82% underwent successful large remnant ablation [4]. As evidenced by Bal et al. radiosensitivity is unpredictable and highly variable between individual patients. Their study found overall cumulative success rates of ablation were 56% after the first I-131 dose, 92% after the second, and 100% after the third [5]. Our patient’s large remnant ablation was presumed successful after receiving 31.9 mCi I-131, based on a subsequent undetectable thyroglobulin level.
Lobar ablation appears to be a two-step procedure, with the first dose of I-131 being akin to a surgical thyroidectomy and the second dose acting as a remnant ablation [5]. Our patient received a second dose of 158.5 mCi I-131. Remarkably, the metastatic mediastinal lymphadenopathy and most of the pulmonary nodules largely regressed after the initial I-131 treatment. There is a lack of long-term data regarding recurrence in patients treated with I-131 for large remnant ablation. Leblanc found no difference in recurrence rates between those treated with partial thyroidectomy plus I-131 versus those treated with total thyroidectomy after a median follow up of 6.2 years [6]. A larger follow up study by Santra found similar results [7]. There is little to no data regarding prognosis of patients treated with I-131 for large remnant ablation with distant metastasis at the time of treatment. A large study with long-term follow up would be necessary to provide adequate comparison.
The recommended treatment for high-risk differentiated thyroid carcinoma is total or near-total thyroidectomy followed by radioiodine ablation. However, if total or near-total thyroidectomy is not possible, large remnant ablation is a feasible option, as this case illustrates.