Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2013) Volume 2, Issue 4
Objective: To examine if sleep timing (combination of bedtime and wake up time) is associated with energy intake and physical activity/sedentary behaviour in obese adolescents.
Methods: Participants included in this cross-sectional examination were 26 (13 females) obese volunteers (BMI ≥ 95th percentile) with a mean age of 13.6 ± 0.5 years and valid data on self-reported sleep, food intake (dietary record), physical activity and sedentary time (accelerometer), screen time (self-reported), and anthropometry (BMI). We categorized participants as “late sleepers” (midpoint of sleep >3:30 a.m., n=13) and participants as “normal sleepers” (midpoint of sleep ≤ 2:30 a.m., n=13).
Results: As expected, wake-up time and bedtime were different between sleep timing groups (p<0.01); however, total sleep duration was the same (9.23 ± 1.14 vs. 9.16 ± 1.28 hours for normal and late sleepers, respectively, p=0.88). There was no significant BMI difference between late sleepers and normal sleepers. Total daily caloric intake was 27% higher in late sleepers (425 kcal) compared to normal sleepers (p=0.04). Using a linear regression model in the whole sample we observed that later sleep timing was associated with greater total caloric intake, independent of age, sex, BMI, moderate-to-vigorous physical activity (MVPA) and sleep duration (β=368.6, p=0.01). No association was found between sleep timing and MVPA or sedentary time. However, later sleep timing was related to greater screen time, independent of age, sex, BMI and sleep duration (β=105.7, p<0.01).
Conclusion: The present study is the first to report that later bedtime is associated with greater caloric intake and screen time in obese adolescents independent of total sleep duration.
Keywords: Children; Adolescents; Food intake; Obesity; Physical activity; Sleep timing
Childhood obesity has been widely identified as a complex condition, with a plethora of factors that are associated with its development. Accumulating evidence suggests that short sleep duration may be an additional determinant of obesity [1,2]. The mechanisms by which short sleep duration influence body weight are under investigation and might involve both sides of the energy balance equation. Experimental sleep restriction has been reported to increase appetite via an up-regulation of appetite-stimulating hormones [3]. Lack of sleep could also lead to weight gain and obesity by increasing the time available for eating and by making the maintenance of a healthy, physically active lifestyle more difficult [4]. In an environment where energy-dense foods are highly palatable and readily available, caloric intake may be directly proportional to the time spent awake, especially if most of wakefulness is spent in screen-based sedentary activities where snacking is common [5]. Furthermore, the increased fatigue and tiredness associated with not having enough sleep may impact overall physical activity participation [6].
In addition to the duration of sleep, sleep timing may also play an important role in energy metabolism and recent studies have set out to investigate the effects of misaligned sleep timing on health [7,8]. For example, an animal model experiment has shown that feeding mice at the “wrong time”, i.e. when they are supposed to sleep, can lead to weight gain [9]. Interestingly, a 2011 observational study involving 52 adults has shown that “late sleepers” (midpoint of sleep ≥ 5:30 a.m.) consumed on average 248 more calories per day than “normal sleepers” (midpoint of sleep <5:30 a.m.), with the majority of the excess calories occurring at dinner and after 8:00 p.m. [10]. This finding suggests that greater caloric consumption in the evening may be a behaviour that links later sleep timing to obesity risk. Likewise, two recent cross-sectional studies by Australian researchers have shown that late bedtimes and late wake up times are associated with a higher risk of obesity and poorer diet quality in children and adolescents, independent of sleep duration, physical activity level and sociodemographic characteristics [11,12]. More specifically, children with a later bedtime/later wake time engaged in less Moderate-to-Vigorous Physical Activity (MVPA) and in more screen time compared to a group of early bedtime/early wake time children, despite having similar sleep duration [12]. Similarly, the same authors found that children with a later bedtime/later wake time had a higher Body Mass Index (BMI) Z-score and consumed more nutrient poor foods than the early bedtime/early wake time group [11]. Although the literature is still sparse, these novel findings suggest that sleep timing, particularly time to sleep, is an important factor to consider for health outcomes and behaviours that is distinct and separate from total sleep duration.
A better understanding of children’s sleep timing behaviours is thus needed to determine whether children with late-to-bed behaviours engage in more sedentary time and/or consume excess energy, two behaviours that may impact body weight. To our knowledge, the present study is the first to investigate sleep timing and its relationship with caloric consumption and activity patterns in a population of obese children and adolescents. The primary objective of this study was to determine whether sleep timing is associated with energy intake and physical activity/sedentary behaviour of obese children and adolescents. We hypothesized that obese children and adolescents with later sleep timing would have greater daily energy intake, lower MVPA and greater sedentary time than those going to bed earlier, independent of total sleep duration and other potential confounding factors.
Participants
A sample of 62 obese children and adolescents aged between 8 and 18 years with a BMI greater than the 95th percentile [13] were recruited from the Children’s Hospital of Eastern Ontario (Ottawa, Canada) endocrinology clinic to participate in the Physiological and Psychological Predictors and Determinants of Metabolic Complications of Pediatric Obesity (POC) study between 2008-2010. All new patients visiting the pediatric endocrinology clinic for an obesity assessment were eligible to participate in the POC study and 26 of the original 62 met the eligibility criteria for the current cross-sectional analysis. These included having 5 or more days of self-reported sleep data (time to bed and time to wake), 3 days of complete dietary recording and at least 4 days of valid accelerometer data for assessment of their sleeping, eating and physical activity behaviours, respectively. Further details of the study subjects are displayed in Table 1. The POC protocol was approved by the Children’s Hospital of Eastern Ontario’s Research Ethics Board and written informed consent (>16 years) or parental consent and child assent (≤ 16 years) were obtained before study initiation as required by the institutional ethics board.
| Normal sleepers (n=13) | Late sleepers (n=13) | p value | |
|---|---|---|---|
| Age (years) | 13.3 ± 3.1 | 13.9 ± 2.0 | 0.53 |
| Sex Boys Girls |
5 (38) 8 (62) |
8 (62) 5 (38) |
0.24 |
| Height (cm) | 157.4 ± 12.0 | 164.4 ± 11.7 | 0.15 |
| Body weight (kg) | 91.6 ± 27.8 | 96.4 ± 19.6 | 0.61 |
| Body mass index (kg/m2) | 36.4 ± 8.1 | 35.6 ± 6.4 | 0.77 |
| Wake-up time (hour:min) | 7:08 ± 0:41 | 8:06 ± 0:47 | <0.01 |
| Bedtime (hour:min) | 21:54 ± 0:34 | 23:01 ± 0:55 | <0.01 |
| Sleep duration (hour) | 9.23 ± 1.14 | 9.16 ± 1.28 | 0.88 |
| Daily energy intake (kcal/day) | 1590 ± 468 | 2015 ± 543 | 0.04 |
| % Protein | 19.3 ± 5.9 | 19.2 ± 4.3 | 0.94 |
| % Carbohydrate | 49.6 ± 8.0 | 48.1 ± 7.1 | 0.61 |
| % Fat | 31.1 ± 7.4 | 32.7 ± 7.5 | 0.57 |
| MVPA (min/day) | 28.2 ± 10.0 | 42.9 ± 4.9 | 0.03 |
| Sedentary time (min/day) | 575.6 ± 17.1 | 560.3 ± 26.4 | 0.64 |
| Screen time (min/day) | 137.5 ± 17.2 | 225.3 ± 52.4 | 0.13 |
Table 1: Descriptive characteristics of participants (n = 26).
Anthropometric assessment
Weight was measured to the nearest 0.1 kg using a medical grade SECA 634 calibrated digital scale. Standing height was measured to the nearest 0.5 cm using a wall-mounted SECA 222 stadiometer. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared and BMI Z- scores were computed. These measurements were performed by trained research assistants according to standardized methods [14].
Sleep assessment
Participants were asked to self-report their respective time to sleep and time to wake for a 7-day period, and the average over 7 days was computed (bedtime, wake time, and sleep duration). Previous studies have found good agreement between self-reported sleep timing and objective measures such as actigraphy [11,15].
Classification of sleep timing groups
Midpoint of sleep for each participant was calculated by subtracting half of the total sleep duration from time to wake (e.g., 8:00 a.m. wake time- ½ 10 h slept = 3:00 a.m. midpoint). Participants were categorized a priori into two age-specific groups; children (≤ 12 years) and adolescents (≥ 13 years). The rationale for this stratification is based on the different sleep needs in these two groups [16]. In both age groups, “late sleepers” were defined as having a midpoint of sleep greater than the median and participants with a midpoint of sleep less than or equal to the median were classified as “normal sleepers” for subsequent analyses. The two normal sleep groups, initially stratified by age, were amalgamated into one group (normal sleepers, midpoint of sleep ≤ 2:30 a.m., n=13), and the same procedure was replicated for the late sleepers (midpoint of sleep >3:30 a.m., n=13).
Food intake assessment
All participants were instructed to complete a 3-day dietary record, including 2 week days and 1 weekend day. Participants were shown how to complete the record by the research coordinator who provided instructions about measuring the quantities of ingested foods. Subjects were instructed to log when they ate and what they ate at each meal and snack, during the 3-day period. If time for snack and meals were reported simultaneously, the two meals were merged for consistency. Mean energy and macronutrient intake was calculated using the ESHA food processor SQL dietary analysis software (ESHA Research, USA), with the 2007 Canadian Nutrient File. This method of dietary assessment has been shown to provide a relatively reliable measure of diet in this population [17]. Of note, the 3 days of dietary record data were matched to sleep data for each participant.
Physical activity and sedentary behaviour assessment
Participants were asked to wear an Actical accelerometer over the right side of their hip on an elasticized belt during waking hours for 7 consecutive days. The Actical device measures and records timestamped movement in all directions and provides an assessment of physical activity level. A valid day was defined as at least 10 hours of wear time; respondents with 4 or more valid days were retained for analyses [18]. For each minute, the level of movement intensity (sedentary, light, and moderate-to-vigorous physical activity - MVPA) was based on published cut-points: sedentary equating to wear-time zeros plus observations less than 100 counts per minute (cpm) [19]; MVPA equating to 1,500 cpm or more [20]. For each child, minutes at each intensity level were summed for each day and averaged for all valid days. Further details on how the MVPA and sedentary time were derived from the accelerometers can be found elsewhere [18,21].
While accelerometers can accurately classify participant’s behaviours as sedentary, they do not provide information about the type of sedentary behaviour or context. For this reason, daily screen time values were derived as a mean score of reported time spent watching TV/movies, playing seated videogames and spending time on computers outside of school or homework over a 7 day period. Although self-report measures provide reliable estimates of screen time, their validity remains untested [22].
Statistical analysis
Since there was no statistically significant gender interaction between sleep timing and the outcome variables, data for both sexes were combined to improve clarity and maximize power. Independent t-tests were used to test for differences between groups (late sleepers vs. normal sleepers). A chi-squared test was also used to assess statistical significance with categorical variables. Furthermore, we conducted a linear regression analysis to examine the association between sleep timing and daily energy intake, MVPA and sedentary behaviour. In the adjusted analysis, age, sex, BMI, MVPA (when not the outcome) and sleep duration were entered into the model to determine whether the association is independent of these covariates. All statistical analyses were performed using the Statistical Package for Social Science for Windows software (SPSS 20, IBM, USA). A two-tailed p value of less than 0.05 was considered to indicate statistical significance.
Baseline characteristics of participants by sleep timing category are shown in Table 1. The midpoint of sleep for the children (≤ 12 years) was 2:48 a.m., whereas the midpoint of sleep for the adolescents (≥ 13 years) was 3:08 a.m. We observed no significant difference in the anthropometric measurements between sleep timing groups. As expected, time to wake and time to bed were significantly different between child and adolescent groups; however, total sleep duration was not different.
Total daily caloric intake was 27% higher in late sleepers (425 kcal) compared to normal sleepers, p=0.04, with no difference in macronutrient distribution. Figure 1 provides a visual representation of cumulative calorie intake across the day for a sub-sample, n=16, of participants for whom we had complete data on meal timing. Albeit not statistically significant due to the small sample size, this illustrates a tendency for greater food intake later in the evening (after dinner). MVPA was nevertheless significantly higher in late sleepers; however, late sleepers engaged in 88 min more daily screen time on average, p=0.13, than their counterparts categorized as normal sleepers.
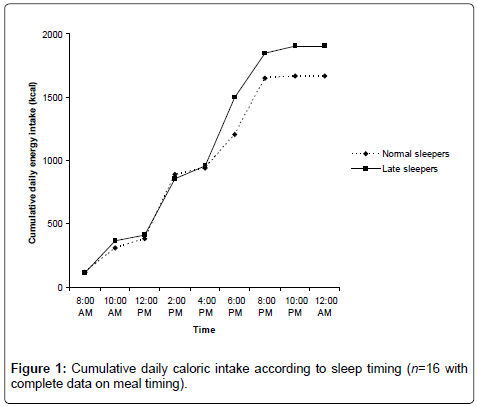
Figure 1: Cumulative daily caloric intake according to sleep timing (n=16 with complete data on meal timing).
The relationship between sleep timing in the whole sample and daily energy intake is shown in Table 2. We observed that later sleep timing behaviour was associated with greater total caloric intake in this cohort of obese adolescents, independent of sleep duration and other covariates. In the adjusted model (model b), 25% of the variance in daily caloric intake was explained by sleep timing and a 1-hour change in sleep timing was associated with a 369 kcal/day change in energy intake. However, when screen time was entered into the model the association became non- significant. We did not find any association between sleep timing and BMI Z-score (data not shown).
| Beta | 95% CI | r | p | |
|---|---|---|---|---|
| Unadjusted model | 359.8 | 59.7; 660.0 | 0.45 | 0.02 |
| Adjusted modela | 368.6 | 101.2; 636.0 | 0.50 | 0.01 |
| Adjusted modelb | 141.9 | -143.1; 426.8 | 0.21 | 0.31 |
Table 2: Association between sleep timing and daily energy intake in obese
adolescents.
As shown in Table 3, the linear regression analysis did not identify a significant association between sleep timing and daily MVPA or sedentary time in this cohort. Later sleep timing was however related to greater screen time, independent of sleep duration and other covariates, p<0.01. In the adjusted model, 31% of the variance in screen time was explained by sleep timing and a 1-hour change in sleep timing was associated with a 106 min/day change in screen time.
| Beta | 95% CI | r | p | |
|---|---|---|---|---|
| MVPA (min/day) Unadjusted model | 7.43 | -1.88; 16.74 | 0.40 | 0.10 |
| 6.36 | -1.71; 14.4 | 0.39 | 0.11 | |
| Sedentary time (min/day) Unadjusted model | 11.1 | -34.5; 56.8 | 0.13 | 0.61 |
| Adjusted modela | 4.7 | -20.9; 30.4 | 0.10 | 0.70 |
| Screen time (min/day) Unadjusted model | 125.7 | 42.1; 209.2 | 0.55 | <0.01 |
| Adjusted modela | 105.7 | 36.4; 175.1 | 0.56 | <0.01 |
Table 3: Association of sleep timing with moderate-to-vigorous physical activity and sedentary behaviour in obese adolescents.
Collectively, this study showed that daily caloric intake was 425 kcal higher in late sleepers (midpoint of sleep >3:30 a.m.) compared to normal sleepers (midpoint of sleep ≤ 2:30 a.m.). Furthermore, later sleep timing was associated with greater daily energy intake, independent of sleep duration, BMI, and MVPA; however, the association became non significant after further adjustment for screen time, suggesting that screen time may be a possible mediator of the relationship between sleep timing and increased food consumption. Although sleep timing was not associated with MVPA, we observed that later sleep timing was associated with more screen time regardless of total sleep duration. These findings imply that sleep timing is an important aspect to consider with regards to eating and screen time behaviours in obese children and adolescents and that a narrow focus on sleep duration alone may not be enough.
Our results are concordant with those recently published by other researchers [10-12] showing that later sleep timing is associated with increased food intake and greater screen time engagement. Studies have also repeatedly reported that screen time promotes overconsumption of food [5], suggesting that it may not be surprising to observe a higher food intake later in the day if a large proportion of this time is spent in screen-time sedentary behaviour. However, previous studies in the field have mainly reported that short sleep duration (or experimental sleep restriction) is associated with increased food intake, possibly due to an up-regulation of appetite-stimulating hormones and a longer period of time spent awake [1-3]. The finding that later bedtimes and later wake up times are associated with greater food intake independent of total sleep duration is a novel observation and suggests that sleep timing is also an important additional aspect to consider in the control of energy balance. For instance, a later bedtime likely allows for more unprotected time (i.e. time not spent in school or engaged in a specific activity) for a child or adolescent to access and subsequently consume food or drink.
In contrast to recent findings published by Olds and coworkers [12], we did not find an association of sleep timing with adiposity indices and MVPA in the present study. The most plausible explanation for the lack of association between sleep timing and anthropometric measurements is the fact that the present study was conducted only in an obese sample of children and adolescents, thereby significantly reducing the inter-individual variability in body size. Additionally, the fact that short sleep duration was the same for both sleep timing groups suggests that sleep duration may be more important in predicting adiposity, as previously reported [1], but that sleep timing may still negatively influence eating and screen time behaviours without necessarily impacting body weight. This observation is reinforced by the fact that late sleepers engaged in more MVPA than normal sleepers, thus suggesting that certain unhealthy behaviours (i.e. greater food intake and screen time) can be compensated for by a greater participation in physical activity so that the net impact on body weight is not different between both sleep timing groups.
Although counterintuitive, the observation showing that late sleepers engaged in more MVPA than normal sleepers is in line with recent studies showing large inter-individual variations in physical activity levels across different sleep patterns [23]. It is possible that physical activity participation is more related to individual motivation than to sleep timing per se. For example, restricted sleep has been shown to increase [24,25], decrease [6,26], or have no effect [27,28] on physical activity level in previous studies. Thus, the higher MVPA in late sleepers compared to normal sleepers can be seen as a balancing force for them; however, adjusting for MVPA did not reduce the association between sleep timing and daily energy intake (i.e. no change in the beta coefficient), suggesting that MVPA is not a major explanatory variable. In contrast, further adjusting for screen time substantially reduced the beta coefficient, suggesting that an important portion of the extra 425 kcal ingested by late sleepers may be attributed to snacking while engaging in screen time. In addition, a projected weekly accumulation of 2,975 extra kilocalories for late sleepers would not be fully compensated for by their approximately 98 extra minutes of weekly MVPA approximating less than 1,000 kcal. The residual positive caloric balance is not inconsequential.
The present study has limitations that warrant discussion. First, the cross-sectional nature of this investigation limits causal inferences. Second, the small sample size and preliminary nature of this study preclude any definitive conclusion and generalization of our findings. This is the first study to explore sleep timing and its relationship with caloric consumption and activity patterns in a population of wellphenotyped obese children and adolescents and the fact that many of our associations were significant despite the small sample suggests that the reported relationships are meaningful and relevant. Third, there are the commonly acknowledged limitations associated with self-reported measures (e.g. recall and social desirability bias). Finally, residual confounding is always a limitation in observational studies and the possibility that some unmeasured variables could influence the reported associations (e.g. maturation, socio-economic status, and family characteristics) is always a possibility.
In summary, the present study shows that later bedtime is associated with greater caloric intake and screen time in obese children and adolescents independent of total sleep duration. These substantial differences suggest that that bedtime is an important factor to consider that is separate and distinct from total sleep duration. Given that the higher energy intake associated with later bedtime appears to be partly explained by screen time, future studies should examine whether reducing screen time can positively influence feeding behaviour of late sleepers.
This study was funded by a Canadian Diabetes Association Innovation Grant (#IG-1-07-2307-KA) and equipment was supplied through a CFI/ORF Leaders Opportunity. The funding source had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication. Kristi Adamo holds a CIHR New Investigator Award and an MRI Early Researcher Award. Jean-Philippe Chaput holds a Junior Research Chair in Healthy Active Living and Obesity Research. The authors declare no conflict of interest.