Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Case Report - (2015) Volume 3, Issue 2
Lateral epicondylitis or tennis elbow, is a common elbow malady the extensor carpi radialis brevis origin. It is commonly treated by local injections of steroids are often associated with severe side effects and limited long term efficacy. Recently, hyaluronate is being increasingly used for the treatment of different degenerative processes of joints and soft tissue. Hyaluronate significantly and dose-dependently inhibits cell proliferation and decreased the expression level of mRNA for adhesion-related pro-collagens and cytokines. It is possible that such hyaluronate injections might improve results of injection therapy in tennis elbow syndrome. We reviewed 157 patients with tennis elbow that were treated in general, orthopaedic and hand clinics between 2003 and 2011. All patients were followed for up to one year according to a standardized protocol. Patients with rheumatoid arthritis and other rheumatoid diseases, after fractures or avascular necrosis about elbow, radial tunnel syndrome, and moderate and severe osteoarthritis were excluded. Patients were divided into three groups: first group treated by corticosteroid injection, second group treated by combination corticosteroid and hyaluronate injection and third group treated by hyaluronate injections only. The Hyaluronate treated group was clearly superior to the steroid group in efficacy measures (VAS score and DASH score) as well as side effect frequency. The combination therapy group was similar efficacy-wise to hyaluronate but similar to the steroid group in the number of associated side effects. In conclusion it seems that hyaluronate injection therapy is superior to steroid therapy in lateral epicondylitis.
Keywords: Tennis elbow, Corticosteroids injection, Hyaluronate injection
Lateral epicondylitis (tennis elbow) affects up to 3% of the general population and is the most frequent type of myotendinosis [1,2]. It can be responsible for substantial pain and loss of function of the affected limb for over 1 year in up to 20% of people [3,4]. Tennis elbow is considered an overload injury of the ECRB at the point of attachment at the lateral epicondyle. Most researchers agree that "angiofibroblastic hyperplasia" or non-inflammatory degeneration of Extensor Carpi Radialis Brevis (ECRB) or common extensor tendon is the pathology combined with cellular apoptosis [5]. In most cases the pathology is described as self-limiting, but requires medical treatment because of long time functional disability of the patients. The wide spectrum of nonsurgical treatment modalities (rest, activity modification, stretching exercises, using of counterforce brace, NSAID, steroid injections, botulinum injections, and shock wave therapy) is an indication that not one of them is highly effective. NSAID's are most useful for short-term pain relief. Injection of corticosteroids is efficacious for short time pain relief but is problematic because of rare severe adverse effects including tendon rupture [1]. There is a growing body of evidence supporting the use of hyaluronate injections in patient with ankle sprain, adhesive capsulitis of the shoulder, patients after flexor tendon injury and hip pathology, although the mechanism of the effect have not yet been clarified [6-11]. There is some evidence that hyaluronate significantly increase proliferation of vascular Endothelial Growth Factor (VEGF) and collagen type 4 for up to six weeks after injection. In addition it seems to decrease the amount of adhesion tissue, and dose-dependently inhibited cell proliferation and decreased the expression level of mRNA for adhesion -related pro-collagens and cytokines [5,12-14].
Use of Hyaluronate in lateral epicondylitis for treatment of tennis elbow in clinical practice has only seldom been described [1,2]. In this study, patients who received hyaluronate injections for lateral epicondylosis (tennis elbow) had significantly greater improvement in VAS (Visual Analogue Scale) pain at rest and after grip testing than control that persisted to 1 year follow up [2]. The use of hyaluronate injections for this entity has been routine in our practice for the last 10 years. This study is a prospective evaluation of 3 groups of patients treated with hyaluronate and compared with corticosteroid injection and combination therapy.
Patients
The patient cohort consists of a consecutive series of 157 patients treated for Tennis Elbow (TE). All subjects received research groups from populations speaking Hebrew, Arabic and Russian according including and excluding criteria’s only. The average age was 54 ± 8.5 (range 18-65 years). M/W ratio was 76/81. Ten patients had bilateral TE. Fifty four patients were treated with a single corticosteroid injection (betamethasone dipropionate 5 mg. and betamethasone sodium phosphate 2 mg.). Forty nine patients were treated with a standard single sodium hyaluronate 2% (40 mg / 2.0 ml) injection (Ostenil Tendon, TRB Chemedica International S.A., 1211 Geneva, Switzerland). Fifty four of the patients were injected using a combination of hyaluronate and steroids as described above. The first step was the steroid injection. Hyaluronate injection was carried out in 7-10 days after the steroid injection. In ten patients a non-simultaneous bilateral injection therapy was performed. All injections were performed according to the standard technique of peritendinous TE injection.
Tennis elbow diagnosis
The diagnosis of tennis elbow was made by detection of pain on the lateral side of the elbow and at the lateral epicondyle on palpation and during resisted dorsiflexion of the wrist of at least three months duration.
All patients were treated conservatively by NSAID's (oral celecoxib 100 mg per day or topical dicloren gel 1%) and physiotherapy for two to three months before being included in this study.
Inclusion criteria
a) Patients that diagnosed as TE as described above
b) Minimal 3-months symptom duration
c) Due to possible side-effects risk of injection therapy, only patients with a VAS score of 9 or higher upon localized pressure during palpation were included
d) Patients have completed and did not respond to a standardized physiotherapy protocol consisting of 6 sessions of deep friction massage, transcutaneous electrical stimulation and resistance training over 2 months as well as oral celecoxib 100 mg per day for 14 days and topical diclofenac 1% gel for two months
e) Patients gave consent to injection therapy
Exclusion criteria
Exclusion criteria included:
a) Treatment of TE within the last year that was not according to the specified protocol
b) Previous elbow surgery of any kind
c) Known systemic rheumatic disease
d) Patients exhibiting symptoms of radial tunnel syndrome
e) Elbow osteoarthritis on radiographs
f) Cervical radiculopathy
g) Elbow instability
h) Patients who were unable to understand the questionnaires were excluded from the study
Choice of therapy
Patients were offered a choice between injections of either medication or a combination of both types. Due to pricing considerations the patient's decision was based on financial ability and preferences. It should be appreciated that while the out-of-pocket patient expense is 15 times higher for the hyaluronate group, it was a quite frequent choice. This probably is due to patient's anxiety about steroid injections and their complications that is rather prevalent in the public.
Treatment effect assessment
Patients were assessed using a back -translated DASH (Disabilities of the Arm Shoulder and Hand) version for the three most common languages (Hebrew, Russian and Arabic). A higher score indicates greater disability. The questionnaire was self -filled by the patients, and a research assistant verified questionnaire filling.
In addition a standardized VAS score was filled out in answer to the question: "What number would you give your pain right now?" Higher scores indicate greater pain intensity.
Statistical analysis
Statistical analysis was performed using the Analyze-It for Microsoft Excel (version 3.60.1, 2014) statistical program. ANOVA or the Kruskal Wallis test for non-parametric variables was used to compare groups and time points. Student's t-score was used to compare two groups of continuous variables. Power analysis was performed using Russ Lenth Pitface program (version 1.76, 2011). For a sample size of 50 patients per group the study was powered to detect a 15 percent difference at 99% (S.D. assumed to be 0.2).
The treatment groups were similar in size and the steroid group patients were significantly older (58 ± 9 years old) than the hyaluronate group (50 ± 5 years old) or the combination therapy group (53 ± 7 years old) (ANOVA, F value>13, p<0.001). The patients that underwent steroid injection had higher DASH score (median 87, range 69-98) as compared with patients undergoing hyaluronate injection (median 82, range 67-95) or combination therapy (median 84, range 69-97). The average DASH score at baseline was 86.8 (range 92.8-80.8) for the steroid injected group, 81.9 (range 85.9-77.9) for the hyaluronate injected group and 83.7 for the combination therapy group (range 89.7- 77.7). The inter-group difference was statistically significant (H-statistic 11.8, p < 0.002) but the steroid group was similar to the combination group in a post hoc analysis.
All groups improved after injection both as measured with the DASH score and the VAS score (Table 1, ANOVA, F>30, p<0.0001, Table 2, ANOVA, F>45, p<0.0001). The treatment modality appears to be important in determining the response especially at the one year follow-up time point (Figure 1). Hyaluronate containing injections appear to possess clear superiority over steroid only therapy. Once again the results with hyaluronate and combination therapy appear to be similar.
| Average DASH score at baseline | Average DASH score at 6 months | Average DASH score at 12 months | |
| Steroid | 86.8 ± 6 | 45.9 ± 5 | 61.3 ± 4 |
| Hyaluronate | 81.9 ± 4 | 35.9 ±2 | 7.7 ±3 |
| Combination Therapy | 83.7 ± 6 | 35.9 ± 4 | 12.9 ± 4 |
Table 1: Average DASH Score.
| Average VAS score at baseline | Average VAS score at 6 months | Average VAS score at 12 months | |
| Steroid | 10.0 ± 0 | 4.4 ± 1.5 | 5.5 ± 1 |
| Hyaluronate | 10.0 ± 0 | 3.3 ± 1 | 0.6 ± 0.5 |
| Combination Therapy | 10.0± 0 | 3.2 ± 1 | 1.1 ± 1 |
Table 2: Average VAS Score.
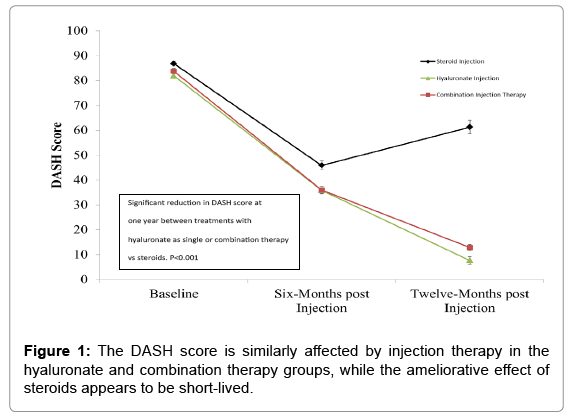
Figure 1: The DASH score is similarly affected by injection therapy in the hyaluronate and combination therapy groups, while the ameliorative effect of steroids appears to be short-lived.
VAS score improved in the hyaluronate and combination groups better than in the steroid group. The decrease averaged 4.5 units in the Steroid and Combination treatment groups and 9.4 units in the hyaluronate group at one year follow-up time point (ANOVA, p<0.001, F>225).
Average VAS score at 1 year after treatment was significantly higher (average 5.5 ± 4) in the steroid group as compared with 0.5 ± 2 for the hyaluronate group and 1.1 ± 1 for the combination group (ANOVA, F value>218, p<0.001). The latter two groups appear to have similar scores at one year after injection.
The degree of improvement in DASH score at one year is not gender specific (Student's t-test, t-statistic<0.3, p>0.7). Similarly the VAS score improvement does not appear to be gender specific (Figure 2).
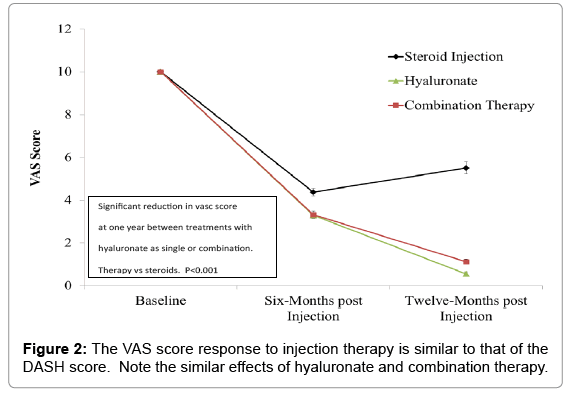
Figure 2: The VAS score response to injection therapy is similar to that of the DASH score. Note the similar effects of hyaluronate and combination therapy.
There were 22 repeat injections within one year in this group. All repeat injections were in the steroid injected group consisting of over 40 percent of the group. The sub-group requiring repeat injections was analyzed for any unique predicting factors. There was no significant difference in gender (3:1 male predominance in the hyaluronate and combination injected groups versus 3.1:1 male predominance in the steroid group) or age (53 in the hyaluronate group versus 57 in the steroid injected group) between the groups. The change in VAS score averaged 5 units in the patients that required repeated injections in contrast with 9 units in the patients that did not require repeat injections.
Out of 157 treated patients there were 16 side-effects reported including 10 patients with fever (defined as per-os measured temperature of 37.5ºC or higher) and 7 patients with localized erythema (one patient had both). Other side effects were not observed.
The improvement in DASH score was 64 ± 21 in the group without side effects, versus 58 ± 20 in the group with side effects (the difference was not significant, Student's t-test, p>0.23). The improvement in VAS score was 8.3 ± 2 in the group without side effects, versus 8.1 ± 1.7 in the group with side effects (the difference was not significant, Student's t-test, p>0.7). The groups with and without side effects were similar in age and gender distribution. There were 6 patients with side effects in the steroid group, no patients with side effects in the hyaluronate group and 10 patients with side effects in the combination therapy group.
Tennis elbow is a common clinical disorder of unknown etiology. The condition is widely believed to originate from repetitive overuse with resultant micro-tearing and progressive degeneration due to an immature reparative response [15]. Histological evaluation supports a non-inflammatory degenerative process. There is evidence that the tendon degeneration involves both apoptotic and autophagy mechanisms [5]. A proposed mechanism involves tendon pathology, changes in neuromuscular function as well as changes in pain threshold [3]. Neurochemicals including glutamate, substance P, and calcitonin gene-related peptide have been identified in patients with chronic tennis elbow and in animal models of tendinopathy [16].
It is known that hyaluronate plays a significant role during development, wound healing and regeneration, has anti-inflammatory effects as well as the possibility that its presence will restore normal tissue function [17,18]. It enhances muscle progenitor cell recruitment as well as tendons and inhibits premature myotube fusion, implicating a role for this glycosaminoglycan in functional repair [19].
The current study examined the use of three types of injection therapy. The groups were similar in size, but the patients undergoing steroid therapy were a little older and had better DASH score, though due to study design had similar pre-injection VAS score. The slight demographic difference is between the groups is due to the study design. This study did not have a randomized design due to ethical considerations and statistical processing was not performed for the data related to origin ethnicity and race. However, the authors noted that no difference was seen in the study regarding the criteria.
The use of steroid has become associated in the public opinion with severe side effects and an immediate pain relief with dubious long-term results, and thus most patients either agree to this therapy or not but would not agree to randomization. On the other hand, hyaluronate is a much more expensive therapeutic modality. It appears to be more efficacious than steroids in the rather selective group chosen for this study, patients with severe pain who failed two months of conservative treatment [20].
The current study supports the use of a single hyaluronate injection as therapy for lateral epicondylitis in preference to steroid injections. The steroid effect appears to diminish with time in contrast to the hyaluronate effect. A meta-analysis has shown that steroid therapy is not more useful than placebo [21]. A combination injection treatment is also possible, but its results are not better than those achieved using hyaluronate alone. On the other hand, the side effects appear to be more frequent when steroid injection is used, whether alone or in combination. Corticosteroid injections appear less efficacious than other treatments in the intermediate and long term. According to the literature, steroids used in the elbow region, might incur a risk of tendon damage and are probably less efficacious than placebo therapy [22]. Local tissue damage caused by injection of steroid can explain the pain and functional deterioration at point of 12 months follow up (increased DASH score and VAS) in this study. It’s not observed in the combination therapy group. The authors assume that hyaluronate injection ameliorate and restore normal tissue function and prevents local tissue damage of the steroids
The results of the combination therapy group appear to be similar to those of the hyaluronate group; however there was a tendency toward more side effects in the combination therapy group. It is possible that addition of steroids might provide faster pain relief, but causes systemic and local side effects typical of the use of steroid injections. However this was not assessed in the current study that focused on intermediate and long term results.
The current study appears to indicate that hyaluronate injection is a preferable alternative to steroid injections for the treatment of tennis elbow. The effect size is larger with hyaluronate injections, and lasts longer.
Limitations of the current study include lack of group randomization. However, due to the significantly greater risk of side effects and need for repeat injections in the steroid group, it seems that a clear recommendation of hyaluronate injection could be made in preference to steroid injections. Further research should be performed comparing the results of phototherapy and hyaluronate injections, as both appear to be efficacious [21].
Data collection was performed by LG, AS and AG, manuscript drafting was performed by LG, ER and DR.