Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Commentary - (2016) Volume 5, Issue 3
Although the surgical treatment of Obstructive Sleep Apnea (OSAS) expanded significantly over the last years with different techniques, uvulopalatopharyngoplasty (UPPP) remains the most common procedure used in the treatment of this complex syndrome.
It dates back to 50 years ago when Ikematsu [1] in Japan, developed a surgical procedure to relieve snoring shortening the soft palate and uvula with 80% of snoring improvement. Many techniques were developed after that.
Quesada et al. [2] introduced the Partial Palate Resection (PPR), more aggressive technique, that is considered the first method of UPPP. However, they were published in Latin language and because of that did not spread out.
Fujita et al. [3] published in English the UPPP technique, modifying the original procedure of Ikematsu [1], generating great enthusiasm among otolaryngologists.
Many surgical procedures emerged trying maximize results with great variations of success rates.
Sher et al. [4] in a meta-analysis of unselected cases treated with UPPP from 1966 to 1993, revealed that only 40.79% had successful surgery defined as 50% reduction of Apnea-Hypopnea Index (AHI).
Even Fujita [5] described different anatomic levels of obstruction in OSAS and that half of the patients were non-responders to the UPPP.
Riley et al. [6] described the surgical multilevel concept with 239 patients presenting 93.3% (223) having multilevel site of obstruction, type 2 (oro and hypopharyngeal) and only 16 patients (6.7%) had single level obstruction.
Senior et al. [7] considered that many patients worse after UPPP.
Comparing clinical findings to success or failure of UPPP, Friedman et al. [8] constructed a clinical staging system for patient selection those who will benefit from UPPP alone and those who need additional treatment, usually involving hypopharynx and tongue base. The system is based on three clinical findings: palate position, tonsil size and body mass index (BMI).
According to this selection, stage I patients would more likely benefit from UPPP alone where stage II and III need additional treatment to hypopharynx [8].
Multiple techniques were developed to evaluate the Upper Airway (UA) obstruction and currently sleep endoscopy (DISE: Drug-Induced Sleep Endoscopy) is considered the best way to identify the specific areas of collapse to plan an effective treatment [9,10].
With this new vision now it became rare that the surgeons treat OSAS with UPPP as a single treatment. Lin et al. [11] reviewed 49 multilevel surgery articles (1,978 patients) with success rate of 66.4%.
Currently, the UPPP remains a common surgery for OSAS treatment most combined with adjunctive multilevel procedures. Weaver et al. [12], in a multicenter study, provided that UPPP improves quality of life and sleep apnea symptoms in patients with sleep apnea.
Multiple UPPP techniques have been described, in the past few years, changing the concept of aggressive palate resection to palatal reconstructive surgery, improving function by altering form.
More than these traditional techniques, which simply remove tissue, these new procedures involve reconstruction of the upper pharyngeal airway tissues modifying structural abnormalities improving form and function.
Since Fairbanks [13] modifications, maximizing the lateralization of the posterior pharyngeal pillars, increasing the lateral dimensions of the oropharyngeal airway, a large number of UPPP techniques have been created with the same principles.
The latest procedures include: Uvulopalatal flaps [14], ZPalatopharyngoplasty [15], Palatal Advancement Pharyngoplasty [16], Lateral Pharyngoplasty [17], Expansion Sphincter Pharyngoplasty [18], Relocation Pharyngoplasty [19] and many others.
These new techniques may offer better outcomes over traditional methods of UPPP in selected patients Friedman II and III with lateral pharyngeal wall collapse (Figure 1).
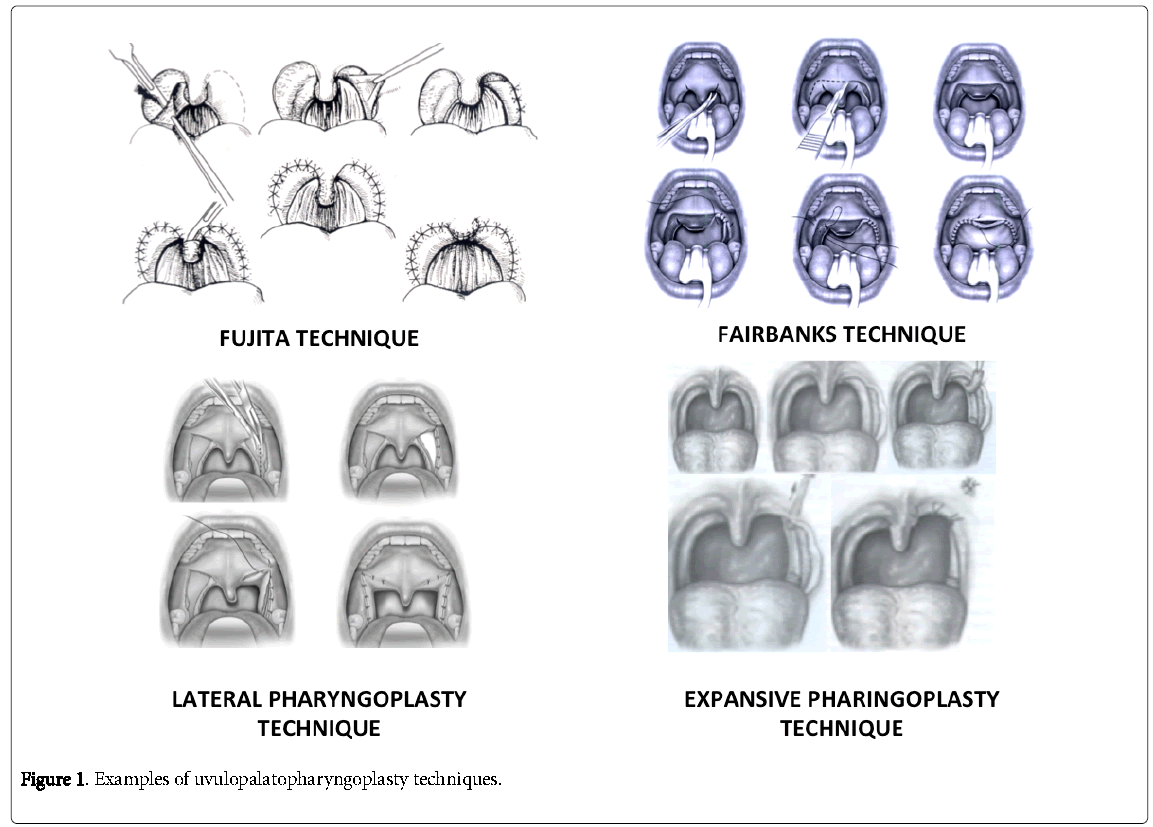
Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies.
The Friedman et al. [15] staging identifies tongue and tonsil size but not the velopharyngeal shape patterns that must be treated according its anatomical configuration. The lumen of OSA patients are more elliptical and flattened and more easily collapsible.
These innovative surgical techniques remodel the narrow pharynx advancing the soft palate and splint the lateral pharyngeal walls enlarging the lumen and lessen pharyngeal collapse.
Based on these new surgical concepts, the UPPP should be performed alone less frequently, in favour of being part of a multilevel approach according to the patient’s needs.