Journal of Leukemia
Open Access
ISSN: 2329-6917
![]() +44 1300 500008
+44 1300 500008
ISSN: 2329-6917
![]() +44 1300 500008
+44 1300 500008
Research Article - (2018) Volume 6, Issue 1
Keywords: Chronic lymphocytic leukemia; Complete remission; Partial remission, Progression free survival; Global survival
Chronic Lymphocytic Leukemia (LCL) is a neoplasia characterized by small or slightly irregular type B lymph cells, found at the peripheral blood, bone marrow, lymph nodes and spleen [1,2]. As per the International Workshop on Chronic Lympocytic Leukemia (IWLCL), diagnosis criteria include type B lymphocytic leukocytosis (>5 × 109/L) with frequent incidence of CD5 and CD23, low-intensity CD20 and CD79b and incidence of surface immunoglobulin, for over three months [3]. This makes it different from monoclonal B-cell lymphocytosis where said number of lymph cells is not reached and there are no lymphomatoid characteristics and which immunophenotyping may be LCL, atypical LCL or unrelated to LCL.
LCL incidence is different across the world population. In white people with Caucasian heritage, it is accepted from 2 to 6 cases in 100,000, per year. It is more frequent in men. On the contrary, it is less common in Asians; in Korea, it is estimated at 0.11 in 100,000 [4]. In African-ascendants is 2.8 in 100,000. Moreover, in Asians who migrate to the US, this does not change [4-7]. In Mexico, it is six times lower than in Caucasian populations [8]. These facts suggest the genetic impact on the disease incidence. There are reports concerning the frequency variability of genes involved in LCL in Caucasian and Asian populations [9]. This variability impacts on the behavior differences of the disease across race populations.
After the diagnosis, data is found to show differences in terms of forecasting impact. For this purpose, Rai and Binet scales are wellknown Both are clinical, simple [10,11]. Inexpensive and easily applicable classifications that remain widely used. However, due to the clinical heterogenicity of the disease, this has led to finding other more accurate and specific forecasting factors. Moreover, with these new predictors, not only early disease results are sough, but also to select amongst the available treatments out there. With the FISH analysis, at least five forecasting alterations have been identified: in 13q14, trisomy 12, in 11q22-23, in 13p13 and in 17p; these chromosome anomalies range from a good to a bad forecast With immunogenetics techniques, it is possible to identify mutated or unmutated LCL cells, with worse results in the latter kind [12,13]. Through sequencing, many mutations have been identified; there are four forecasting implications at least: NOTCH1, SF3B1, BIRC3 and TP5 (fludarabin refractories); these are all related to a bad forecast [14,15]. The CD38 and CD49 level increase and the ZAP70 incidence are equally related to a bad forecast [12,16]. More recently, the minimum residual disease quantification has been incorporated to the forecasting studies [12,17-19].
From 1960, Chlorambucil and cyclophosphamide were the first drugs to show a consistent therapeutic impact on LCL; administered with or without prednisone and 50% responses were achieved [14]. Later, purine by-products were introduced (pentostatin, cladribine y fludarabin) that were soon related to alkylants, more particularly, to cyclophosphamide 90% [19-21]. As of this century, rituximab has been incorporated, generally related to cyclophosphamide and fludarabin (chemoimmunotherapy); with a response rate of 95% [22]. For this therapeutic line, other agents have been used: alemtuzumab, ofatumumab, and obinutuzumab; there is no absolute difference favoring a particular combination if toxicity, cost and efficacy are considered [12,14].
Over the last years, many new drugs have been found with different efficacies and dosage advantages. Obinutuzumab is a third-generation anti-CD20 that selectively links malignant B-cell lymphomas and leads to its death Ibrutinib is a Bruton tyrosinase inhibitor, required to keep the B-cell receptors way active (BCR; in oral form [23]. Idelalisib, an inhibitor promoting the programmed neoplastic cell death inhibiting its interactions with the environment [24]. There are other compounds, some of which are being used and others remain in development stage [25]. All of them, although effective on their own, become even more effective when combined, generally, with chemotherapy. New agents are first-line or second-line anti-LCL agents; its main functionality focuses on wrongly forecast varieties.
Autologous transplantation of stem cells does not offer substantial advantages when compared against new pharmacological treatment On the contrary, allogeneic transplantation is still to be considered for refractory diseases de novo, given the long-term efficacy of new drugs remains unknown [26,27].
The purpose of this study was to report the therapeutic results obtained from prospective protocols at the Hematology Service of our hospital, over the course of this century, before new drugs were used. All patients underwent chemotherapy (only one recent group also received rituximab).
All LCL patients taken care of at the Hematology Service of the National Medical Center (CMN) “20 de Noviembre”, ISSSTE [Institute for Social Security and Services for State Workers], from 2001 to 2016 were included. Inclusion criteria: with LCL with no prior treatment and no contraindications to receive the drugs used in our therapies. Each therapy was prescribed and followed prospectively. Those who died due to comorbilities unrelated to LCL, those who refused to continue undergoing chemotherapy or whenever the medical care was suspended due to administrative causes (loss of eligibility to the state health insurance) were removed from this study.
Patients included in this study were diagnosed with LCL and met the following criteria: persistent lymphocytosis above 5 × 109/L, for more than three months; typical lymphocytic morphology, with less than 10% of immature forms; immunophenotype of B strain with CD5, CD19, CD 79a, CD 20, CD22, CD23, CD24, CD25 + low-intensity SmIg; 30%+ lymph cells in the bone marrow.
The following variables were studied: age and gender; diagnosis date; general symptoms (lassitude, weight loss and fever, unrelated to infection); liver, spleen, and enlargement sizes; hemolytic state; initial infection; complete blood count and bone marrow; lactate dehydrogenase (DHL); glucose, urea, creatinine and uric acid; serum levels of immunoglobulins; bilirrubins; ranking as per Rai and Binet scales, comorbilities.
The initial treatment, curing degree and length of disease progression was recorded. Second-line treatment, magnitude and time to curing. The final results were recorded.
The final goals were progression-free survival (SLP) and global survival (SG).
First-line therapies were three (as for autoimmune hemolytic anemia, in any case, Prednisone 1 mg/Kg/day was added for a month):
CL (Every four weeks, until cured): Chlorambucil, 0.2 mg/kg/day, oral form, days 1 to 14 and two-week discontinuation.
CF (Every four weeks, six cycles): Cyclophosphamide, 250 mg/ m2SC, IV bolus, days 1 to 3. Fludarabine, 25 mg/m2 SC/day, IV bolus, days 1 to 3
CFR (Every four weeks, six cycles): Cyclophosphamide, 250 mg/ m2SC, IV bolus, days 1 to 3. Fludarabine, 30 mg/m2SC/day, oral form, days 1 to 4. Rituximab: 375 mg/m2SC, IV, day 1.
In second line, Cyclophosphamide, Vincristine and Prednisone (COP) or the same added anthracycline drugs (CHOP). If not used for first line, these were also prescribed for CFL and CFLR.
Complete remission Silent disease. No enlargements enlarged liver or enlarged spleen. Hemoglobin >11.0 g/dL, neutrophil granulocytes >1.5 × 109/L, neutrophilic granulocytes <4.0 × 109/L , with regular bone marrow.
Partially remission: Silent disease. 50% decrease in enlargements, enlarged liver or enlarged spleen. Hemoglobin >11.0 g/dL or with 50% initial value improvement; neutrophilic granulocytes >1.5 × 109/L or 50% initial value improvement; lymph cells with a >50% initial value decrease.
In progression: 50% increase in the neoplastic mass (lymphocytic leukocytosis, enlargement size, enlarged liver or enlarged spleen).
Statistical software SPSS version 22.0 for Windows was used. The descriptive analysis was conducted with central and scattering trend actions, absolute measures and percentages (nominal variables) or averages/means and limits (numeric variables). Comparative or association tests were conducted with chi2 and with non-parametric tests (Wilcoxon or Kruskall-Wallis). For global and progression-free survival, the Kaplan Meier method was used with log-rank for curve comparison. p <0.05 was taken into account for statistical significance. Confidence intervals (IC) were determined at 95%.
At the CMN “20 de Noviembre” Hematology Service, from 2001 to late 2016, 2’857patients were taken care of de novo. Out of these patients, 61 were diagnosed with LCL (2.1%). The main clinical and hematological data are found under Table 1.
| Fact | Result |
|---|---|
| Gender (F/M) | 27/34 |
| Age, in years (median/Limits) | 66/39-89 |
| Prior Evolution, weeks | 11/0-52 |
| Attack General Status (yes/no) | 36/25 |
| Hemolysis (Yes/No) | Apr-57 |
| Enlarged liver (Number/median in cm) | 34/3 |
| Enlarged spleen (Number/median in cm) | 56/6 |
| Enlargements, regions (<3 / >2) | 29/17 |
| Hematocrit % (median/Limits) | 38/6-51 |
| WBC x 109/L (median/Limits) | 120/16-448 |
| Neutrophilic granulocytes x 109/L (median/Limits) | 7/0.4.24 |
| Lymph cells x 109/L (median/Limits) | 104/10-430 |
| Platelets x 109/L (median/Limits) | 180/8-353 |
Table 1: Initial Clinical and Hematological Data Comparison against different protocols: p>0.08
The male gender was more prevalent. The minimum age of participation was 39 years old with a standard deviation of 11. In 26 patients, no initial sign was found and the most frequent alteration was an attack to the general status. Four patients suffered from initial hemolytic state (6.6%).
Two patients suffered from chronic airways infection initially. Mediastinal infiltration was found in one case and in another case, skin infiltration was found.
The mean lymph cell count, in the bone marrow, was 79% (40% to 96%).
The occurrence, intensity and magnitude of clinical and hematological data was equally distributed across the several first-line therapies (p>0.11).
The DHL mean was 239 UI/L with limits from 111 to 1’112 UI/L. The highest numbers were defined in patients suffering from hemolytic state (p=0.0001)
Classifications related to Rai and Binet forecasting scales are found under Table 2. Most are within the best forecasting levels. Level II (Rai) and A (Binet) were the most common ones, mainly in patients treated with CFR (p=0.02).
| Scale | No % | CL% | CF% | CFR% | N= |
|---|---|---|---|---|---|
| Rai 0 | 40 | 4 | 5.3 | 8.3 | 5 |
| I | 0 | 20.8 | 10.5 | 0 | 7 |
| II | 0 | 54.2 | 73.7 | 91.7 | 39 |
| III | 60 | 12.5 | 10.5 | 0 | 8 |
| IV | 0 | 8.3 | 0 | 0 | 2 |
| Binet A | 40 | 58.3 | 73.7 | 91.7 | 42 |
| B | 0 | 25 | 8.3 | 8.3 | 10 |
| C | 60 | 16.7 | 10.5 | 0 | 9 |
Table 2: Patient distribution as per the Rai (p=0.02) and Binet (p=0.087) scales
Twenty-four patients suffered from chronic diseases when LCL was diagnosed; Diabetes Mellitus type 2 in 14 patients; uremia in 4 patients, heart disease in 3 patients; the remaining ones were systemic high blood pressure (2) and rheumatoid arthritis (1).
Until 2004, the first-line therapeutic treatment was CL only. CF was applied for the next four years (until 2008). Lastly, CFR is used until 2016. Table 3 lists the use frequency for each.
| Treatment | N= | % |
|---|---|---|
| None | 5 | 8 |
| Chlorambucil | 23 | 38 |
| CF | 16 | 26 |
| CFR | 17 | 28 |
CFR: Cyclophosphamide/Fludarabine/Rituximab
CFR: Cyclophosphamide/Fludarabine/Rituximab Cyclophosphamide/FludarabineCyclophosphamide/Fludarabine
Table 3: Therapeutic Treatments Used
The curing magnitude of each therapy is found under Table 4. The lack of remission is only noticed when no treatment was administered or CL or CF treatment was administered. The best responses were achieved with CFR (p=0.0001).
| Remission | |||
|---|---|---|---|
| Treatment | None | Partial | Complete |
| None (Num/%) | 5/100 | 0 | 0 |
| CL (Num/%) | 8/34.8 | 7/30.4 | 8/34.8 |
| CF (Num/%) | 1/6.3 | 3/18.8 | 12/75.0 |
| CFR (Num/%) | 0 | 0 | 17/100 |
| Total (Num/%) | 14/23.0 | 10/16.4 | 37/60.7 |
Table 4: Cures resulting from several first-line treatments (p= 0.0001).
CL toxicity was found once only (neutropenia). There were two incidents with CF: neutropenia and pancytopenia. CFR was related to two cases of pancytopenia. (p=0.52).
Results, after first-line treatment, are found in Chart 5. Five patients did not receive any treatment due to early death (n=2) or due to the patient’s or his/her family members’ refusal (n=3). Progression occurred in 26 cases Table 5.
| Treatment | Remission | Progression | Death | Removed |
|---|---|---|---|---|
| None | 0 | 0 | 2 | 3 |
| Chlorambucil | 0 | 14 | 3 | 6 |
| CF | 3 | 8 | 3 | 2 |
| CFR | 10 | 4 | 1 | 2 |
| Total (Num/%) | 13/21.3 | 26/42.6 | 9/14.8 | 13/21.3 |
Table 5: Destination after the first-line treatment (p= 0.0001).
Its occurrence was more frequent in CL (p=0.001). The time to occurrence was variable Figure 1. The highest efficacy in SLP was reached with CFR (p=0.0001). Nine patients passed away (14.8%), due to these causes: infection (6), bleeding (2) and activity (3), 13 patients were removed: 11 were dropouts and two due to ancillary death caused by comorbilities.
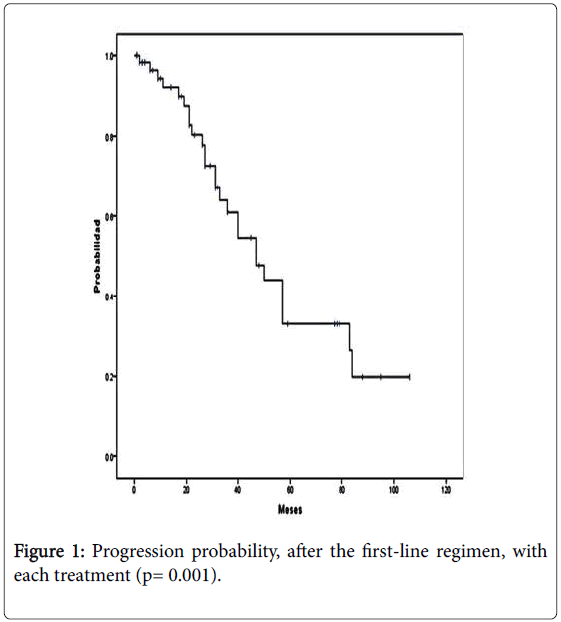
Figure 1: Progression probability, after the first-line regimen, with each treatment (p= 0.001).
Twenty-five patients agreed to receive second-line treatment: CHOP/COP 9, CF 7 and CFR 9. The selection between and CHOP and COP (N=9) was reliant on the first-line treatment (CL). In CF (N= 7), whether CL (5) was used or not was stated; in two cases, CF was repeated. CFR was stated in 9 cases, 5 received CF initially and the 4 remaining ones, CFR. The results of progressive patients were: fully cured 1 (3.8%), partially cured 2 (7.7%), death 4 (15.4) and removed 19 (73.1%).
With second-line treatment, patients had an additional average survival of 38 months (IC from 23 to 55)
The final results at the end of the study were: fully cured 12 (19.7%); partially cured 2 (3.3%); death 12 (19.7%); and removed 35 (57.4%). Death causes: 10 related to infection, 1 related to bleeding, and 1 to activity.
Causes of removal: death caused by comorbility 4 (11.4%) and dropouts 31 (88.5%). Dropouts that were fully cured 16, partially cured 8, and no remission whatsoever 6.
SLP (Figure 2) has an average of 47 months (IC 33.2 to 60.8). SG (Figure 3) does not reached the median and an average of 135 months (IC 33.2 to 158). The highest SG (p=0.001) was reached with CFR: 80% after 106 months.
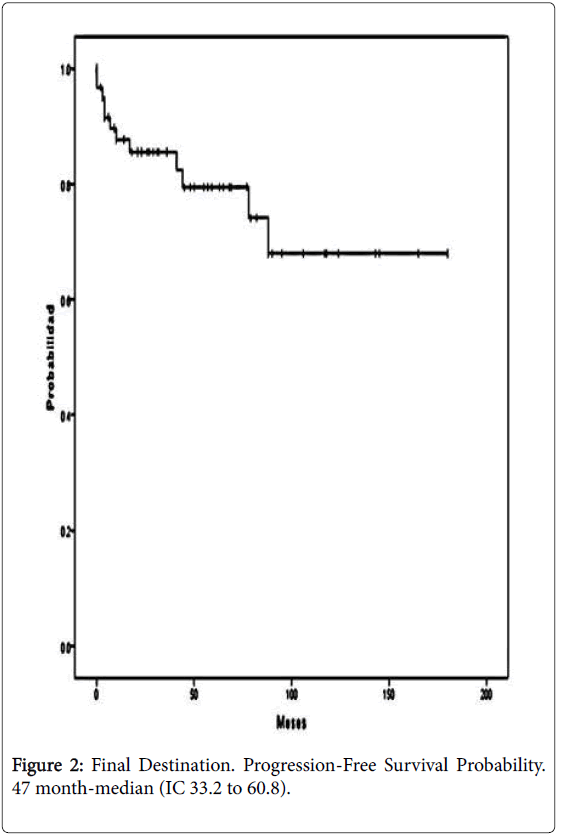
Figure 2: Final Destination. Progression-Free Survival Probability. 47 month-median (IC 33.2 to 60.8).
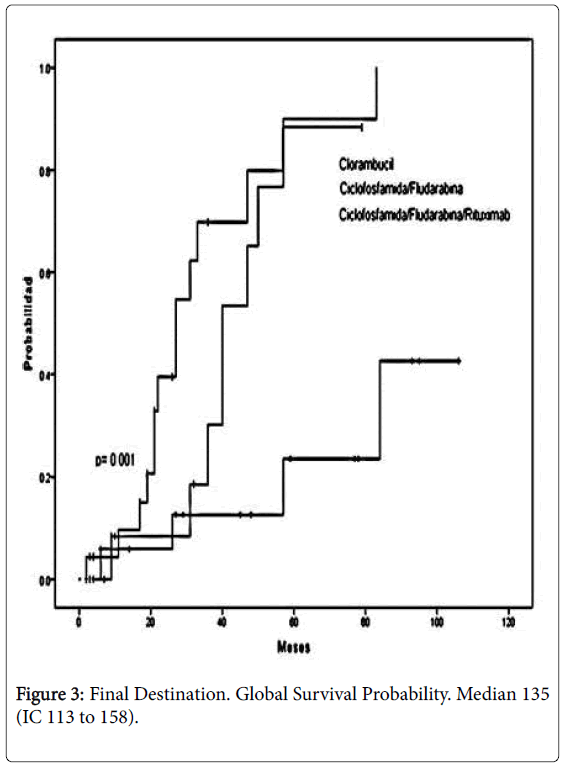
Figure 3: Final Destination. Global Survival Probability. Median 135 (IC 113 to 158).
Forecasting factors were searched with all initial variables. In the univaried analysis, to get a full initial remission, initial hemolysis (p=0.02), Rai levels III and IV de Rai (p=0.03), number of hematocrit <36% (p=0.0001), lymphocytic leukemia >83 × 109/L (p=0.003) and DHL >211 UI/L (p=0.001) had a negative impact. No variable with a forecasting value was found for SLP. A negative forecast was found in SG related to an attack to the initial general status (p=0.01) and lymphocytic leukocytosis >81 × 109/L.
With multivaried analysis, in the case of initial remission, no forecasting factor was found. In SLP, the lymphocytic leukocytosis >81 ×109/L (p=0.04) has a negative impact (p=0.04). SG was negatively impacted on in the case of lymphocytic leukocytosis >62 × 109/L (p=0.02) and due to lymph cells in the bone marrow > 69% (p=0.01).
The relative incidence of new LCL cases taken care of in our hospital show the low LCL incidence in our country. As causes thereof, as per the international literature, several genome modifications have been found after having compared Asian and Caucasian populations [9]. More recently, a study was published showing a decrease in the B cell lymphoma 2 (BCL2)-modifying factor incidence, an antiapoptotic modulator [27]. Genetic differences have been defined, including its clinical consequences amongst said populations, although there is no final explanation [28]. Environmental influencing factors impacting on these dramatic differences are proposed. However, there are no final data. Nonetheless, this impact related to LCL incidence is a fact, regardless of the patient’s race, by using military-use toxics (Orange Agent: 2,3,7,8-tetrachlorodibenzo-p-dioxin)[29].
Age and gender distribution in our patients is similar to that of other domains. Although found in young patients, LCL is not rare in 30 to 40-year-old patients [30]. The clinical incidence is not very different from our descriptions above, with less than sick individuals who have suffered from attacks, scarce incidence of hemolytic state and initial infection. Several clinical and hematological data were not statistically different across all three therapeutic treatments (p>0.08). Amongst Rai and Binet classifications, most were found in the low-risk scales, lower than III or B. In other reviews incorporating various cases, risk distribution in both classifications is found across all stages: in Rai (19% to 13%) and in Binet (21% to 25%) [31]. These data show that, in our population, a disease starts with a better initial forecast, as per all two classifications.
Comorbilities were typical for the age and, naturally, chronic and degenerative ones. The most popular one was Diabetes Mellitus, type 2. This is also typical in Mexico, across several age ranges, with a similar incidence (22%), for 60+ years [32]. However, these did not impact on the patients’ results related to efficacy and toxicity. Factors with a negative forecast, to get to a full initial remission, in the univaried analysis, were initial hemolysis, anemia, DHL increase, lymphocytic leukocytosis and those who reached Rai levels III and IV, although it was not designed for this purpose [10,11]. No variable with forecasting value was found for SLP. A negative forecast was found in SG related to an attack to the initial general status and lymphocytic leukocytosis.
In the multivaried analysis, lymphocytic leukocytosis was a negative predictor for SLP and SG and lymph cell count for the bone marrow. Therefore, lymphocytic leukocytosis is the most frequent variable related to the forecast. It seems reasonable that being a benchmark of the neoplastic level it may be used as a reliable indicator. However, this finding has not been consistent, although other authors have reported it. Compared against the new forecasting data and new drugs, the variables herein are applicable only if used as per the treatments used herein [33]. With new drugs, new forecast data are to be used.
All three first-line treatments were used in several stages. It relied on drug affordability. In fact, CL had been used in our hospital a long time before, with dosage differences, but not always protocolized [13]. At the beginning of this century, it was administered regularly, scheduled and with consistent dosage. Initial cures through CL, in our studies, are comparable to those reported by other authors (69%). CF efficiency is also comparable to other reports (80%)[34,35]. The best responses, with first-line treatment, were obtained with CFR, a known observation [36] SLP, after the initial treatment, was also better with CFR and matches other studies [36,37] . In one of the pioneer works with CFR and six-year follow-up, SG is 77% [38]. Our reported SG is lower but includes CL and CF-treated patients. If CFR-treated patients are included only, the length was higher and comparable to the one above [38]. It is to be considered that our results come from a low-risk population, as per Rai and Binet scales.
First-line treatment is initiated for progressive diseases. Moreover, there are new data impacting on the therapeutic choices: TP53 (or dysfunction); IGHV mutational status, serum B2 microglobulin, age and clinical stage (Rai/Binet); with these data, five risk groups have been calculated with SG, at five years, from 93.2% to 23.3%. Even with this information, CFR treatment, as used in this treatment, remains the first-line treatment [13,39-41]. It is acceptable to use other combined anti CD20 with chemotherapy, instead of rituximab, with apparent advantages (obinotuzumab/chlorambucil)[40-42]. In the case of highrisk sufferers (from 17p and TP53 mutations), with active and progressive disease, options including ibrutinib, venetoclax, idelalisib or stem cell transplantation. In any case, it would be recommendable to control the patient’s response by defining the minimum disease level.
With the drugs administered to the patients under examination and with no access to drugs, the acceptable second-line treatment is the treatment used herein. With these drugs, over three years of survival were achieved. Our behavior was to prescribe treatments other than first-line treatments, except for those where the CF or CFR treatment was repeated. The progression time was not measured, as recommended [40,42]. Recent criteria for new medication, recommend to repeat first-line handling if progression happens after three years; if progression were to occur before that time period, ibrutinib, idelalisib, venetoclax, lenalidomide and other drugs may be used. If these have not been used, cyclophosphamide, fludarabine and rituximab combinations are equally recommended [42]. Several guides recommend to provide care to LCL patients at hospitals with expert personnel who follow in-house protocols [13,40]. First- or second-line toxicity was limited to neutropenia or pancytopenia. 12 deaths resulted from the end study; most of them occurred due to infections and only one case of death caused by neoplastic activity.
At the end of the study, over half of the patients had been removed or most dropped out of it. The number of dropouts is very high and the exact cause of this remains unknown, although most of them were fully or partially cured. This suggests that the dropout cause was related to out-of-hospital deaths, unrelated to the LCL activity or administrative reasons.
LCL incidence, in our hospital, is very low and does not entail a main issue, given its magnitude. As per the Rai and Binet forecasting scales, most of the patients are in a good forecast, below levels II and B; yet our results did not influence on the final result forecast. The initial lymphocytic leukocytosis showed a negative forecasting value for SLP and SG.
The CFR protocol proved to have the highest efficiency in SLP and SG. This makes it a convenient first-line treatment as adverse factors (in 17p and TP53 mutations) are absent. Other chemo immunotherapy combinations seem to have comparable results.