Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2018) Volume 7, Issue 1
Background: In general, the prognosis in patients with well differentiated thyroid carcinoma (WDTC) is excellent. However, there are small cohorts of patients who experience a more aggressive form of disease which is often associated with certain poor prognostic factors. Identifying these patients at an early stage is imperative for guiding treatment decisions. The purpose of the work is to study the cumulative survival of patients with WDTC, depending on a number of clinical and biological characteristics of tumors.
Methods: A retrospective cohort study of patients operated on WDTC in the period from 1995 to 2015 (5526 people). Each patient was analyzed according to age, gender, tumor size and characteristics of the TNM (7 editions), clinical stage, volume of surgery, number of points on the MACIS scale, risk group, number of courses of radioiodine treatment, result treatment and the term of postoperative observation. The construction of cumulative survival curves was made according to the Kaplan-Meier approach. To compare the cumulative survival index value in groups, the non-parametric Log-rank test was used.
Results: The most unfavorable factors of the prognosis for patients with WDTC are such integrated indicators as the stage of disease IVb and IVc, as well as tumors of the T4b category. It is also unfavorable to recognize the age of patients over 60 years, the presence of distant metastases, the stage of disease IVa, the category of carcinomas T4a and the size of the tumor more than 40 mm. Other prognostic factors (invasion, multifocal tumor growth, metastasis of carcinoma to the lymph nodes, male sex, post-operative relapse), although they are probable predictive factors, but have somewhat less significance in analyzing the prognosis of survival of patients.
Conclusion: Understanding the importance of certain prognostic factors of survival is extremely necessary, since they are the only indicators of the effectiveness of the diagnostic, medical and organizational work will reduce the number of patients who require aggressive treatments and, consequently, increase the duration and quality of their postoperative life.
Keywords: Well differentiated thyroid carcinoma; Prognostic markers; Age; Size; Metastasis; Extra-thyroid extension; Invasion; Clinical stage; Risk group; Volume of surgery; Radioactive iodine avidity
WDTC: Well Differentiated Thyroid Cancer
Thyroid gland cancer is the most wide-spread endocrine system tumor. During these last 20 years significant increase is seen concerning morbidity due to well-differentiated (papillary and follicular) thyroid cancer (WDTC), the increase being 4 times higher in women and 3 times higher in men [1]. The prognosis for these carcinomas types is generally favorable, although in some small patient cohorts the disease may lead to lethal consequences. Early detection of tumor lesions, choice of optimal tactics of treatment and postoperative patient management improve significantly the results obtained as well as patients’ life quality.
Special attention is continuously paid to WDTC cases detected following the Chernobyl catastrophe because of this pathology significant expansion following irradiation of inhabitants due to the accident [2] as well as because of the existence of further risk of thyroid carcinomas development. The latent period becoming from the moment of irradiation influence and continuing to the disease manifestation may be as long as 50-60 years [3]. The superfluous relative risk developing already in 5 years following irradiation remains almost constant during the whose human life, the superfluous absolute risk becoming higher in the course of time [4]. The age of patients having been irradiated in their childhood and the number of such persons become greater in the course of time having passed from the moment of the accident; therefore, the problem of demographic prognosis for such patients becomes more and more actual [5]. These facts call forth both the continuous monitoring of population groups having become victims of the Chernobyl catastrophe and the study of long-term results of patient’s treatment and their lives quality in the post-operative period. The risk-adapted observation strategy is based on the current understanding of the disease biology and on the analysis of prognostic factors when current observation approaches are deliberately used. Prognostic factors help to detect patients with high relapse or death risk as well as to stipulate for adequate individual therapeutic approach.
In spite of a number of prognostic systems elaborated for the WDTK (AGES, MACIS, AMES, DAMES, SAG, GAMES) and being used with different frequency to forecast the life span and/or disease relapse risk [6], more and more investigators share the idea that such criteria should be from time to time corrected taking into consideration, first of all, individual risk [7-10]. The authors underline the importance of further investigations aiming to understand better the prognostic relevancy of these systems. The opinion is also suitable prognostic systems are to be adapted also to circumstances and situation of a concrete surgical institution [11].
The aim of this work is the cumulative survival study for WDTC patients having been operated and observed in the surgical clinic of the State Institution V.P. Komissarenko Institute of Endocrinology and Metabolism, Academy of Medical Sciences of Ukraine depending on a number of tumor clinical and biological peculiarities.
Study design and subjects
The authors have carried out a retrospective cohort study of patients having been operated because of the WDTC in the State Institution V.P. Komissarenko Institute of Endocrinology and Metabolism, Academy of Medical Sciences of Ukraine in the period of 1995-2014. Total patients number is 5526 persons. For each patient, the following indices have been analyzed; patient’s age and sex, tumor histological type, its size and characterization according to the TNM (the 7th version has been used), clinical stage, volume of operation, quantity of points according to the MACIS scale, risk group, quantity of radioactive iodine courses, treatment results and duration of postoperative observation. Among patients there were 1,068 males (19.3%) and 4458 (80.7%) females. The mean patient age is 40.9 years (from 10 to 84 years). The papillary cancer was diagnosed in 4,957 patients (89.7%), the follicular one in 569 ones (10.3%). In most cases (5033 patients, 91.1%), thyroidectomy was carried out being supplemented in 1182 patients (21.4%) by the neck dissection; in 493 patients (8.9%) organ-sparing interventions were realized.
Calculating the survival, only the death cases due to underlying disease have been taken into account. This investigation includes 5,346 patients, i.e. 4,337 of females and 1,009 of males. The construction of cumulative survival curves was made according to the Kaplan-Meier approach.
The statistical evaluation of data obtained was made using Pearson’s criterion of distribution concordance (χ2). To compare the cumulative survival index value in groups, the non-parametric Log-rank test was used. All statistical analyses were performed using the computer programs packet Statistica 12 by Stat Soft, Inc. The critical significance level taken was 0.05.
The WDTK prognosis is known to be usually favorable, the general 5 years long and 20 years long survival exceeding 90% [9]. According to our data, the patients survival during 2, 5, 10, and 20 years makes 98.3%, 96,9%, 93% and 89.9%, respectively (for 5,526 patients); the patients survival calculated in cases when only lethal WDTC-due outcomes (5,346 patients) are taken into account reaches 99.2 %, 98.7%, 98.1% and 97.8%, respectively.
The index of diseased men survival from the cohort investigated is somewhat lower comparing to women (Table 1). In the literature available contradictory results are given leading to doubts concerning the prognostic importance of sex [8,12,13]. According to some data, the sex has been determined as a probable prognostic factor using onefactorial analysis; the multifactorial analysis approach, however, has not confirmed this assertion [14]. Nevertheless, our results support a conclusion stating the male sex to be generally a poor WDTK prognostic factor [5,15,16].
| Groups | Duration of survival, years | Р | |||
| 2 | 5 | 10 | 20 | ||
| Sex | |||||
| Females | 99.4 | 99 | 98.4 | 98.2 | 0.0034 |
| Males | 98.4 | 97.6 | 97 | 96.6 | |
| Age, Years | |||||
| <18 | 100 | 100 | 100 | 100 | 0 |
| 19-40 | 99.9 | 99.8 | 99.8 | 99.8 | |
| 41-60 | 99.5 | 98.8 | 98.1 | 98 | |
| >60 | 95.2 | 93.8 | 89.4 | 86.1 | |
Table 1: Cumulative survival indices of different sex and age patients with differentiated thyroid gland carcinomas (%).
The analysis of patients age-dependent cumulative survival was carried out for 4 patients groups; it is recently recommended taking into consideration actual discussion about the necessity of age border correction (before and after 45 years) being accounted during the disease stage determination according to the 7th version of the TNM Classification [5,9,10,15-17]. The worst results among the cohort patients are found for persons above 60 (Figure 1А), whilst the survival index for 19-60 years old patients fluctuates in limits 98.0-99.9 %, reaching 100 % for persons below 18 (Table 1). The data obtained support the opinion the worsening of WDTC patients survival takes place for the age group above 60 [9,13,16]. All the current clinical observations suggest the WDTC patient’s mortality to increase with age. The explanation of poorer prognosis causes is accompanied by the following facts: the patient group aged 60 years and above to contain a higher male part; these persons have tumors above 5 cm with more frequent metastases rate; their disease is usually attributed to the III-IV stages; it is less probable the patients to be treated by iodine isotope; most probably, these patients anamneses inform about external radiation therapy [5,16,18]. Unsatisfactory therapeutic results in elderly patients are also due to their worsened general condition (and accompanying disorders) as well as to decreased tolerance to the treatment.
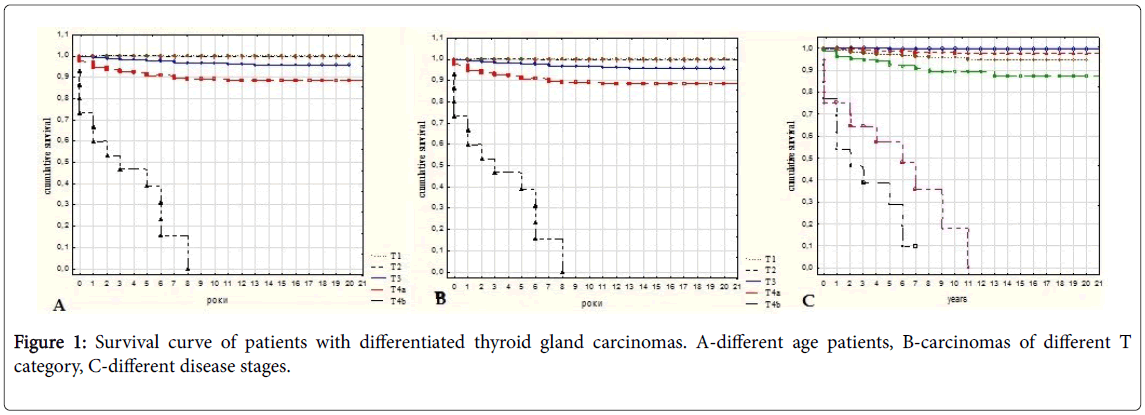
Figure 1: Survival curve of patients with differentiated thyroid gland carcinomas. А-different age patients, B-carcinomas of different T category, C-different disease stages.
Thus, we have confirmed male sex and age above 60 to be significant negative prognostic factors for WDTC patients [5]. Although it is shown the WDTC morbidity to become more frequent in women following menopause establishment due to decrease of estrogens protective action, the masculine sex, however, remains to be a significant negative prognosis factor in elderly persons (the women survival is better even in cases of their more severe disease course comparing to their men contemporaries [15]. This conclusion is illustrated by our data on the mortality level for cohort patients above 60: the morbidity level in men is twice higher comparing to the contemporary women’s one 7.2% (34/469) for women and 15.7% (16/102) for men (Р<0.05).
Primary tumors with sizes 1 cm and below are associated with good prognosis; it becomes, however, worse in the course of carcinoma size increase (Table 2). This fact is also found by other authors [5]. The relapse frequency in patients with tumor sizes above 1cm is 5 times higher comparing to patients with micro-carcinomas [19]. However, other tumor characters including even micro-carcinomas may also influence on the disease prognosis. One of these characters is multifocal tumor growth character; in this case the patient survival being worse comparing to ones whose carcinomas are without this character (Table 2). The multi-focal tumor growth character is associated with capsular invasion, metastases to lymph nodes, and tumors belonging to the category Т2-Т4 [20].
| Groups | Survival duration, years | Р | |||
| 2 | 5 | 10 | 20 | ||
| Tumor size, mm | |||||
| <10 | 100 | 100 | 100 | 100 | 0 |
| Nov-20 | 99.8 | 99.6 | 99.5 | 99.5 | |
| 21-40 | 99.2 | 98.5 | 97.6 | 97.2 | |
| >40 | 94.2 | 92 | 88.6 | 88.1 | |
| Multi-focal growth peculiarities | |||||
| – | 99.5 | 99.1 | 98.7 | 98.6 | 0 |
| + | 97.8 | 97.2 | 95.4 | 94.6 | |
| Intra-thyroid invasion | |||||
| – | 99.9 | 99.7 | 99.2 | 99.2 | 0 |
| + | 98.7 | 98.1 | 97.2 | 96.9 | |
| Extra-thyroid invasion | |||||
| – | 99.9 | 99.7 | 99.4 | 99.4 | 0 |
| + | 96.8 | 95.4 | 93.6 | 92.9 | |
| Metastases into lymphatic nodes | |||||
| N0 | 99.8 | 99.6 | 99.1 | 98.9 | 0 |
| N1а | 99.5 | 99.3 | 99.3 | 98.6 | |
| N1b | 98.7 | 98.3 | 96.8 | 95,6 | |
| Nаb | 96.6 | 95.1 | 93.6 | 93.6 | |
| Distant metastases | |||||
| М0 | 99.4 | 99.1 | 98.4 | 98.2 | 0 |
| М1 | 95.6 | 93.1 | 89 | 87.8 | |
| Т category | |||||
| Т1 | 100 | 100 | 100 | 100 | 0 |
| Т2 | 100 | 100 | 100 | 100 | |
| Т3 | 99 | 98 | 96 | 96 | |
| Т4а | 94 | 90 | 89 | 88 | |
| Т4b | 54 | 39 | 0 | 0 | |
Table 2: Indices of cumulative patient’s survival with differentiated thyroid gland carcinomas with different biological peculiarities (%).
The survival of WDTC patients become worse if tumors possess more aggressive invasive properties: it becomes decreased in cases of carcinoma invasion into the gland tissue and and it is a more significant fact in cases of carcinoma breaking through extra-thyroid tissues (Table 2). An aggravating circumstance worsening the prognosis for patients is increased frequency of tumor metastasis leading to invasion. Par example, in cases of tumor in gland limits metastases into regional lymph nodes were seen in 20% of patients, in cases of extra-thyroid growth the metastases frequency reaching 70%.
The invasion expansion is directly associated with prognostic characters, the prognosis becoming less favorable in the following order: patients with tumors without micro-invasions patients with tumors with micro-invasions patients with tumors with macroinvasion [21]; patients mortality increases up to 31% (this value being 17% in cases of non-invasive tumors) [13].
It should be underlined the information available to demonstrate a significant decrease of patients survival with metastasizing carcinomas (during 20 years of survival, its level was 60% in cases of metastases penetration into lymph nodes and 15% among patients with distant metastases) [13].
According to our data, the prognosis for patients with exactly shown metastasizing carcinomas is worse comparing to patients without metastases; however, 20 years long survival among patients with metastases into lymph nodes does not decrease below 90%, this level being something below than 90% in patients with distant metastases (Table 2). Perhaps such a low survival level given in the work mentioned above is due to about 20% patients with low-differentiated carcinomas in the cohort examined as well as to oxyphyl-cellular carcinomas which are known to be more aggressive than WDTC.
The T category in the TNM system is an integrated index distributing carcinomas not only according to their size, but also according to their characters and tumor expansion. Taking into account that both tumor size and its invasive properties are prognostic factors of WDTC patient’s survival (Table 2), it is clear the T category to be also associated with prognosis. The shortest survival term is seen among patients with tumors of the T4b category (Figure 1B). The mean survival term for patients cohort with such carcinomas penetrating to pre-vertebral fascia, carotid artery or mediastinum vessels is about 3 years following surgical intervention, mortality for this group reaching 87%.
Basing on carcinoma clinical peculiarities according to the TNM system, the disease stage may be determined really permitting the possibility of wide prediction making. Decreased patient survival beginning from the III stage is perhaps due to a fact that these groups include mostly elder persons, in particular, elderly ones (Table 3). The poorest for prognosis are stages IVb and IVc, especially IVb, which foresees (according to the 7th variant of the TNM classification) including to this group of patients with of T4b tumors (Figure 1C).
| Groups | Survival duration, years | Р | |||
| 2 | 5 | 10 | 20 | ||
| Disease stage | |||||
| I | 100 | 99.9 | 99.9 | 99.9 | 0 |
| II | 99.5 | 99 | 97.6 | 97.6 | |
| III | 98.4 | 97.4 | 95.8 | 95 | |
| IVa | 95.2 | 92.4 | 89.2 | 87.2 | |
| IVb | 46 | 29 | 0 | 0 | |
| IVc | 64 | 57 | 18 | 0 | |
| Operation volume | |||||
| ТЕ | 99.6 | 99.4 | 98.8 | 98.7 | 0 |
| HemiТЕ | 99.1 | 98.2 | 97.6 | 97.6 | |
| ТЕ+ dissection | 97.8 | 96.7 | 96.1 | 95.5 | |
| Labeled iodine therapy | |||||
| – | 98..3 | 97.3 | 97.1 | 97.1 | 0.0418 |
| + | 99.5 | 98.9 | 98.2 | 97.9 | |
| Labeled iodine therapy, quantity of courses | |||||
| 01-Mar | 99.3 | 98.9 | 98.2 | 97.8 | 0.8327 |
| 04-Jun | 100 | 98.8 | 98.8 | 98.8 | |
| >7 | 100 | 100 | 100 | 100 | |
| Risk groups | |||||
| 1 | 100 | 99.8 | 99.8 | 99.8 | 0 |
| 2 | 100 | 100 | 99.9 | 99.9 | |
| 3 | 98.2 | 97.3 | 96.1 | 95.7 | |
| Relapsis | |||||
| – | 99.6 | 99 | 98.5 | 98.2 | 0 |
| + | 98.2 | 94.1 | 88.4 | 88.4 | |
| MACIS system, scores | |||||
| <5,99 | 100 | 100 | 99.5 | 99.5 | 0 |
| 6-6,99 | 98 | 96 | 94 | 94 | |
| 7-7,99 | 96 | 94 | 90 | 86 | |
| >8 | 80 | 72 | 61.5 | 59.5 | |
Table 3: Indices of cumulative survival of patients with differentiated thyroid gland carcinomas demonstrating different clinical peculiarities (%).
The mortality of patients included by the cohort with the IVb stage of disease was 92%, the patient’s life span having been about 2 years post operation.
The mortality of patients from the IVc stage was lower (62%), their mean survival term being 3.5 years.
The prognostic WDTC factors mentioned above are independent from clinicians, so it is impossible to control them; however, they are to be taken into consideration when patient treatment and rehabilitation tactics are planning. Currently there are factors depending directly on the type of treatment, both therapeutic and surgical, as well as on adequate post-operative approaches. They include, first of all, the volume of surgical intervention as well as iodine isotope use permitting both to ensure and to foresee the treatment results.
Although the surgical approach is the most important for the WDTC treatment, the question concerning the surgical intervention volume and long-term treatment results, in particular the patients survival, remains poorly studied. There are even the data refusing the interactions between the surgical intervention volume and the level of WDTC patient’s survival: this interaction is underlined to be important only in cases of primary operations on great metastasizing tumors [22]. The majority of surgeons think the gland extirpation together with its tumor is a satisfactory volume of intervention in cases of small carcinomas which do not metastasize and do not invade to extrathyroid tissues (category Т1N0М0); it explains the excellent prognosis for the patient cohort having survived the same operation (Table 3).
Somewhat worse prognosis is shown in cases of extirpation of a single thyroid lobe with a tumor (hemi-thyroidectomy): in some of such patients the risk of post-operative disease relapse in a remained lobe is probably higher. Such operation volume is declared to be acceptable only if the gland contralateral lobe is not damaged by the tumor [23]. The prognosis is also poorer in cases of thyroidectomy and lymph node dissection which are inevitable if the nodes are penetrated by thyroid gland tumor metastases, i.e. in cases of more aggressive carcinomas (Table 3). Therefore, we cannot share the idea that the volume and type of surgical intervention do not exert on the level of patients survival [22].
As to the survival of patients with post-operative relapses, it is quite naturally lower comparing to ones without relapses; it is especially true for patients having survived during 10-20 years following the tumor extirpation (Table 3). In this sense it is important to determine prognosis for patients from different relapse risk groups (low, moderate or high). Our data witness the prognosis to be quite favorable for first two groups, being, however, significantly less favorable for high risk group (for WDTC patients, the high risk is determined in cases of “aggressive” histological carcinoma type, extrathyroid invasion, multi-focal growth character, tumor size above 4 cm, great metastasizing volume to regional lymph nodes, non-radical surgical intervention as well as patient age above 45; therefore, there are all the factors negative for patients survival) (Table 3). The total thyroidectomy with further radioactive iodine therapy decreases to a marked degree the relapsing frequency and improves the prognosis for WDTC patients [16]; we have also shown this fact; it is found there is no significant difference between patient’s survival levels depending on the quantity of radioactive iodine courses (Table 3).
The prediction system being the most widely used one – MACIS – distributes the cohort patients among groups of low (the I disease stage, sum of scores being <6), moderate, and high risk (the III-IV stages, sum of scores being >8) has permitted to understand the patients survival becomes decreased due to the increased quantity of poor prognosis factors having been involved into calculation (Table 3). At the same time the survival term of cohort patients distributed among these groups is higher comparing to the level indicated by MACIS system authors: they report about 20-years long survival being 99%, 89%, 56%, and 24%, our data are 99.5 %, 94%, 86%, and 59.5%, respectively, the score sums being below 6, from 6 to 6.99, from 7 to 7.99, and above 8. The facts indicated suggest the improving of diagnostics, patient’s treatment and rehabilitation during the period having passed from the moment of the original paper publication [24] to our current time. This conclusion is confirmed by results of patient’s mortality comparison during periods of time 1936-1975 and 1976-2015: the predicted level of patient’s mortality with MACIS prognostic score value above 6 is lower for the last period mentioned, although the relapses quantity remains at the same level [25].
Therefore, the investigations realized permit to conclude the most unfavorable prognostic factors for WDTC patients are such integrated indicators as the disease stages IVb and IVc and also tumor Т4b categories. Even in cases of papillary micro-carcinomas, the III-IV disease stages are thought to be negative prognostic factors, although the survival level for this patients group is high (95.7% for 10 years survival [16]. Some changes of components taking into consideration for determination of the disease stage are given in the 8th edition of the TNM Classification [17]; for sure, they will not change the negative contribution of the IV stage in the survival of WDTC patients of 55 years old and above.
The patient’s age above 60, presence of distant metastases, IVa stage of disease, T4a carcinoma category and the tumor size above 40 mm are recognizes as negative prognostic factors. For papillary carcinoma, the presence of distant metastases in elderly patients as well as carcinomas with tumor size above 3 cm requiring aggressive intervention in younger ones are recognized to be important prognostic factors [9]. According to some other information, only distant metastases into bones belong to negative prognostic factors [26], the patient’s age is thought to be an important prediction factor only for drug response prognosis [27].
Other prognostic factors (invasion, multi-focal character of tumor growth, carcinoma metastases into lymph nodes, belonging to the male sex, post-operational relapses), although they are probable prognostic factors, are of lower relevance for the prognosis analysis concerning patients survival. For example, the recognition of metastasizing into lymph nodes and male sex as prognostic factors found in one-factorial analysis have not been confirmed by the multifactorial analysis [28]. At the same time multi-focal tumor growth as well as the presence of category N1b tumor are thought to be important factors of WDTC relapse risk [29,30]. According to some other data, tumor belonging to the N1b category as well as the level of post-operative thyreoglobulin is also relapse development predictors, while it is not true for clinical and biological properties of thyroid carcinomas [31].
Some changed criteria included into the algorithm of the disease stage determination according to the 8th variant of the TNM Classification [17], in particular the increase of the barrier age to 55, are directed to the decrease of patients number which will be included to groups with the III and IV disease studies and therefore to certain limitation of radical treatment approaches. As to post-Chernobyl carcinomas, the requirements to reconsider the necessity of use radical or organ-sparring surgical interventions are also due to decreased, in the course of time, tumors quantity with aggressive biological characters having been more frequently found during the first decade after the catastrophe. In dynamics analysis of such carcinomas frequency in our patients cohort taking into consideration only several parameters being negative factors of patients survival, namely according to Т4а, Т4b and Nаb tumor categories, suggests such a conclusion (Table 4).
| Period of observation | Quantity of patients | Quantity of tumors of categories, | ||
|---|---|---|---|---|
| n(%) | ||||
| Т4а | Т4b | Nаb | ||
| 1994-1999 | 580 | 77 (13.3) | 1 (0.17) | 146 (26.9) |
| 2000-2004 | 1087 | 76 (6.3)* | 6 (0.55) | 162 (14.9)* |
| 2005-2009 | 1650 | 95 (5.8) | 6 (0.36) | 210 (12.7) |
| 2010-2014 | 2209 | 65 (2.9)* | 4 (0.18) | 227 (10.3)* |
Table 4: Twenty years long dynamics of thyroid gland differentiated carcinoma with aggressive characters among a cohort patients.
Consequently, the understanding of different survival prognostic factors is extremely necessary, they being the single indices of diagnostics, treatment and management permitting to decrease the quantity of patients requiring aggressive treatment approaches; in such a way the duration and quality of patient’s post-operative life should become higher.
All authors declare they have no conflicts of interest.