Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 1
Metastatic cancer to the thyroid gland is rare, and indications for subtotal thyroidectomy versus total thyroidectomy are poorly defined. Here we present the first reported case of a patient with a thyroid metastasis from a primary lacrimal sac squamous cell carcinoma. This patient was originally managed with a thyroid lobectomy, but later underwent a completion thyroidectomy. This case is unique in scope and illustrates some of the considerations in determining the best surgical management for thyroid metastases.
<Cancer that is metastatic to the thyroid gland is a rare occurrence, but should always be considered in a patient with a history of cancer who presents with a neck mass [1]. In an autopsy series, the frequency of thyroid metastases among cancer patients were reported to be anywhere from 1.25%-24% of patients [2]. The most common primary sites were renal, colon, breast, lung and sarcoma [1]. Metastases might present synchronously with the primary tumor or with delays of up to 20 years. Surgical management provides a survival benefit to patients with metastatic cancer to the thyroid gland [2]. However, there is no clear consensus as to whether to remove the entire thyroid or to perform a lobectomy or subtotal thyroidectomy to remove just the tumor tissue [3].
Furthermore, primary tumors of the lacrimal drainage system are extremely rare, with less than 900 known cases reported in the literatura [4,5]. Adenoid cystic sarcoma and squamous cell carcinoma (SCC) are the most common subtypes [6]. Here, we describe a case of a thyroid metastasis from a primary SCC of the left lacrimal sac. The case study described helps to illustrate the considerations when determining the optimal strategy for surgical management of secondary thyroid malignancy.
A 48-year-old Asian woman presented to the otolaryngology clinic with a three week history of a left submandibular neck mass. She was managed conservatively with antibiotics and steroids with no improvement. Ultimately, fine needle aspiration (FNA) was positive for metastatic non-keratinizing poorly differentiated SCC. Initial PET scan demonstrated increased uptake near the left tonsil, and CT scans demonstrated fullness in base of the tongue. However, evaluation of the upper aerodigestive tract focusing on the tongue base and tonsil via direct laryngoscopy with biopsy failed to localize a primary tumor. The patient was managed for an unknown primary tumor of the head and neck with radiation therapy, with full regression of the neck lesion. One dose of Cisplatin-based chemotherapy was given, but was discontinued due to the development of tinnitus in the setting of a good response to radiotherapy alone.
A follow-up PET scan 2 months after completion of therapy demonstrated increased uptake in the left lacrimal duct. At this time, the patient admitted to a three year history of left epiphora as well as a palpable periorbital mass that she had noticed while she was undergoing radiation therapy. She underwent left lacrimal sac and duct excision, left perilacrimal fossa bony-soft tissue excision, left anterior ethmoidectomy and left subtotal maxillectomy, as well as a left upper/lower eyelid full-thickness excision and repair with ipsilateral medial canthoplasty and ipsilateral orbitotomy. She also underwent ipsilateral modified radical neck dissection one month later to remove metastatic lymph nodes. Two level 1B lymph nodes were positive for malignancy. She was next treated with 14 fractions of radiotherapy to the primary site for a total of 3500 cGy, in addition to Cetuximab in view of her previous adverse reaction to Cisplatin.
23 months later, the patient presented with intermittent odynophagia and referred otalgia which did not respond to antibiotics. Serial imaging identified a progressively enlarging left thyroid nodule (Figure 1), and the patient underwent an uncomplicated left thyroid lobectomy. Pathology revealed that the left thyroid lobe, surrounding cartilage, soft tissue, and perithyroid lymph nodes were positive for metastatic SCC. Lymphatic spread was felt to be the most likely pathway for this involvement, so completion thyroidectomy with CCRT was proposed, with curative intent. Thyroidectomy and level VI nodal dissection were therefore accomplished, with bilateral para-thyroid cartilage and soft tissue resection as well as neurolysis of the left recurrent laryngeal nerve. Pathology was positive for metastatic lymphadenopathy in level 4, with no disease identified in the right thyroid lobe. The postoperative course was complicated by hypocalcemia that responded to oral repletion, as well as weakness in left vocal cord mobility that improved over several months. She also received concurrent chemoradiation therapy (CCRT) with 5-FU and Cisplatin, which was tolerated well. 5000 cGy of radiation was given in 25 fractions to the anterior neck.
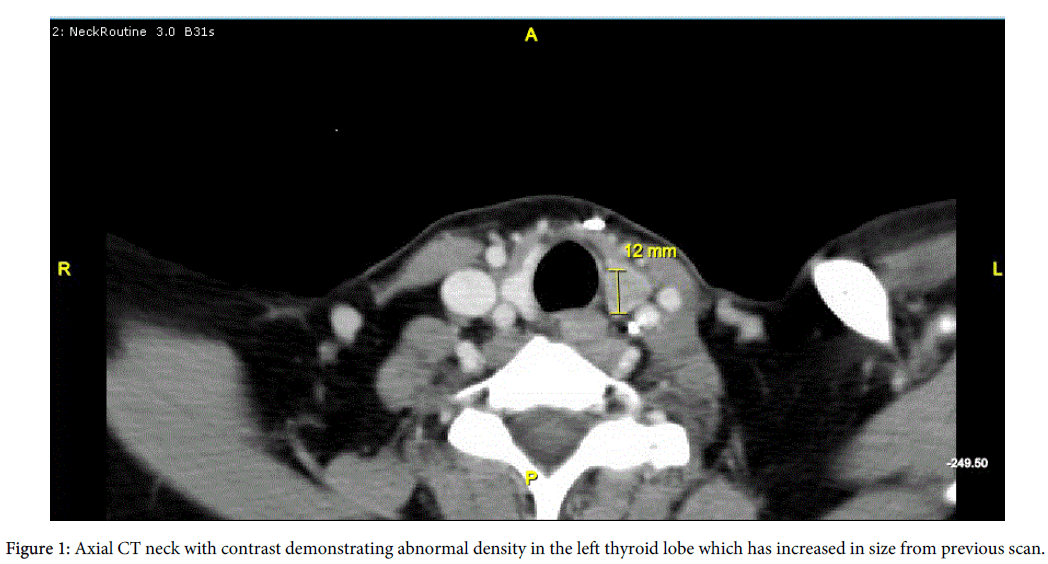
Figure 1: Axial CT neck with contrast demonstrating abnormal density in the left thyroid lobe which has increased in size from previous scan.
Nine months post-thyroidectomy and three months after completion of CCRT, the patient developed additional metastatic submandibular lymph nodes and a left sixth nerve palsy, with findings consistent with leptomeningeal metastases. CT scan of the chest also revealed positive mediastinal lymph nodes. She was then treated with single agent paclitaxel chemotherapy. She ultimately succumbed to metastatic disease a year later, approximately 4 years after undergoing completion thyroidectomy
Primary tumors of the lacrimal drainage system are rare, with less than 900 known cases reported in the literatura [4,5]. Most patients present with epiphora and few have a palpable mass at the medial canthus [4,5]. Among lacrimal tumors, there appears to be no gender predominance and the average age of diagnosis is in the patient’s 6th decade [7]. 50-70% of lacrimal tumors are malignant and 70% are epithelial in origin [4,5]. Most malignant lacrimal sac tumors are treated with surgery or radiotherapy, but there is no consensus for management due to its rarity [5]. A recent cohort analysis suggested that both surgery and radiotherapy improved survival in patients with SCC of the lacrimal duct [6]. However, while local invasion is common, metastases of lacrimal gland tumors are seldom reported [6]. One case series of 82 patients reported lymphatic metastases in 21 patients (26%), lung metastases in 4 patients and esophageal metastases in 2 patients [7]. Secondary malignancies of the thyroid gland are also uncommon, and are predominantly from renal, colon, breast, lung and sarcoma primary sites [1]. To our knowledge, this is the first and only report of a lacrimal tumor metastasis to the thyroid gland.
Secondary tumors of the thyroid gland can arise through either lymphatic or hematogenous spread. The rich vascular supply of the gland does increase susceptibility to hematogenous as opposed to lymphatic spread. It has been shown in these cases that surgical removal of secondary thyroid malignancies is warranted, prolonging survival by an average of ten months [2]. Lymphatic and direct involvement of the thyroid is not uncommon in laryngeal malignancies, where indications for therapeutic and prophylactic management have been described. Recent reports suggest concurrent thyroidectomy if paratracheal lymph nodes are involved, or if there is >10 mm subglottic extension of the tumor [8,9]. More distant lymphatic spread, as from the lacrimal duct, and the management of the contralateral lobe is less clearly defined.
Indications for subtotal thyroidectomy versus total thyroidectomy are not clearly available. The rich vascular supply of the gland raises questions regarding appropriate margins when there is involvement of the contralateral lobe. In cases of hematogenous thyroidal involvement some argue that lobectomy and total thyroidectomy result in similar patient survival [10], while some studies suggest that total thyroidectomy may improve locoregional control rates [2,3,11]. Total thyroidectomy is associated with increased patient morbidity, including dysphagia, speech problems, transient or permanent hypocalcemia, and airway problems, especially in patients with tumor invasion into adjacent neck structures [3]. In this patient who was initially managed with lobectomy, a completion thyroidectomy was performed after extensive discussion because of suspected lymphatic spread of the tumor and her history of recurrent tumor metastases in the head and neck region. The decision to proceed with completion thyroidectomy was therefore undertaken with curative intent. Following thyroidectomy, locoregional disease did not recur in the surgical bed, although regional submandibular metastases were noted. While there were mild sequellae following surgery, these were treated successfully with medical management.
This report highlights the rare occurrence of a lacrimal gland malignancy that eventually metastasized to the thyroid gland. This secondary thyroid malignancy was ultimately resected via a staged procedure with mild sequellae. The decision to intervene surgically in situations such as this should be weighed against anticipated and possible morbidity, and multi-disciplinary discussions may be advantageous.