Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Research Article - (2015) Volume 3, Issue 1
Background: Types of anesthesia and perioperative patient cares are the main determinants of maternal and neonatal outcomes in mothers undergo caesarean section. Body of evidence revealed that maternal and neonatal outcomes were better in mothers who gave birth under spinal anesthesia than general anesthesia. However evidences are lacking locally, hence, this study aimed to compare maternal and neonatal outcomes in mothers who undergo caesarean section under general anesthesia and spinal anesthesia.
Methods: A prospective Cohort study was conducted in Gandhi Memorial Hospital among mothers, who undergo cesarean section under spinal and general anesthesia from March to July, 2014. One hundred and twenty Mothers were followed for twenty four hours period. Statistical Package for Social Sciences version 16 was used to perform descriptive and logistic regression analyses. Statistical significance was set at P-value <0.05 to judge the association.
Results: The total response rate of the study was 120 (100 %). The study revealed that types of anesthesia were independent predictor of maternal and neonatal outcomes. Mothers who underwent caesarean section under spinal were more likely to have postoperative nausea and vomiting (COR=38.5, 95% CI=(12,123). Incidence of low Apgar score in first minute was two and half times more likely to occur in general anesthesia, (AOR=2.54, 95% CI=(1.26, 25.4). The first analgesic request in mothers underwent caesarean section under spinal anesthesia was three times more than mothers underwent caesarean section under general anesthesia (AOR=3.4, 95%CI=(1.4, 6.7)
Conclusion: Spinal anesthesia was associated with high incidence of postoperative nausea and vomiting and hypotension. But first minute Apgar score and first time analgesic request were better in spinal analgesia. General anesthesia was associated with high estimated blood loss, shorter time to first analgesic request and lower first minute Apgar score. Appropriate perioperative patient care by anesthetist and provision of drugs for treatment of hypotension were recommended.
Keywords: Maternal outcomes, PONV, Visual analog score, Addis Ababa, Ethiopia
Caesarean section is the procedure where a baby is delivered through an incision on the abdominal wall and uterus of the mother under general or spinal Anesthesia. It is often life-saving and aims to preserve the health of the mother and her baby [1]. Both general and spinal Anaesthesia are not ideal for cesarean section because each has advantages and risk to both mother and fetus. However, the plan of anesthetist is to choose the method which is safest and most comfortable for the mother, least depressant to the newborn and which provides optimal working conditions for the obstetrician [1-3].
General anesthesia is associated with aspiration of stomach contents, awareness of the surgical procedure, failed intubations, and respiratory problems for both mother and baby, but spinal anaesthesia causes a substantial drop in maternal blood pressure, which may affect both mother and fetus [1-3].
Research findings in Nigeria revealed that 6 of 84 maternal deaths, out of 12, 394 deliveries during10 years, were due to anaesthesia. The most common cause of death during general anaesthesia was failed intubation. There were four deaths due to pulmonary aspiration. Twenty-one patients died due to hemodynamic instability or high block levels during spinal anaesthesia [4].
From a prospective observational study in Malawi, maternal mortality under general anesthesia was higher than mothers underwent caesarean section under spinal anesthesia [5].
According to saving mother’s lives report, there were six deaths related with anesthesia. Obesity was a factor in four of the deaths and the other two were due to failure to manage the airway and inadequate ventilation by inexperienced anesthetist. One death was due to bupivacaine toxicity due to a drug administration error when a bag of dilute local anesthetics was thought to be intravenous fluid [6].
Access to care in Ethiopia did not meet the increments in the incidences and complications of anesthesia. In most of these patients had not been well addressed at large. As a consequence, there was increase the rate and economic burden over all. Proper management is crucial to keep the illness under control and taking the necessary action to protect their lives, health and well-being. Yet the dynamic nature of the problem exacerbate by lack of studies. Hence this study aimed to compare maternal and neonatal outcomes in mothers who undergo caesarean section under general anesthesia and spinal anesthesia.
Study setting and participants
The study was conducted in Gandhi Memorial Hospital, which is one of the Governmental Hospitals in Addis Ababa under Addis Ababa Health bureau in kirkos sub city. This prospective cohort study includes mothers who were ASA I and II full term pregnant mothers and were followed consecutively under general and spinal anesthesia for 24 hrs peri-operatively. Sample size was calculated with two population proportion formulas by considering the following assumptions. It was determined by Level of significance (0.05), Power (0.80) andproportion of maternal satisfaction onVAS from previous study conducted inRawalpindi was 31% and 92% with general and spinal anesthesia respectively [7], which results in the sample size of110. Adding 10 % for allowance of non-response rate, the final sample size became 120 and assuming equal sample size for two groups.
Data collection method and measurement of variables
Data were collected using a pre-tested structured questionnaire. The trained data collectors manage the data in intraoperative and postoperative period and were not responsible for the anesthetic management for that particular subject.The Apgar score, need for support for neonates, maternal estimated blood loss, blood transfusion requirement, blood pressure, time from skin incision to uterine incision and time from uterine incision to baby out were observed intraoperatively and after having informed consent from the mothers, pain severity in 2, 6, and24hrs with visual analogue score and postoperative nausea and vomiting, levels of satisfaction were assessed postoperatively.
Maternal estimated blood losswas estimated by counting small gauze (10ml) and large soaked pack (100ml) blood and also the amount of blood in suction bottle. Maternal blood pressure was taken before conduction of anesthesia and intraoperatively every five minutes. Postoperative pain severity was assessed with Visual Analogue Score (VAS), and VAS values of 0 was taken as no pain and 10 mm-30 mm, 40-60 mm and 70-100 mm were taken as mild, moderate and severe pain respectively.
Satisfaction level was measured using a five point scale ranging from very satisfied to very unsatisfied and clients with satisfaction scale of very unsatisfied, unsatisfied and no opinion were considered as unsatisfied and the others were taken as satisfied.
Neonatal Apgar scores were the major neonatal outcome and which were assessed by standard Table format scored out of ten and interpreted as 0-3, 4-7 and 7-10 for sake of management, 0-3 is very sever which needs resuscitation, and 7-10 is normal as presented in the following Table 1.
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (skin color) | Blue and pale | Body pink, extremities blue | Completely pink |
| Pulse rate | Absent | Bellow 100 | Above 100 |
| Grimace(irritability ) | No response | Grimace | Cry |
| Activity (muscle tone) | No movement | Some flexion of extremities | Active movement |
| Respiration (effort) | Absent | Shallow and irregular | Deep and regular, strong cry |
Table 1: Neonatal Apgar scores.
Data processing and analysis
Data were entered, cleaned and analyzed by using Statistical Package for Social Sciences version 16. Descriptive statistics were run to see the overall distribution of the study subjects with regard to the variables under study. Chi square test and odds ratio were used to determine the association between hypothesized independent and dependent variables. Finally, multivariate analysis was used to control possible confounders and identify independent predictors of the postoperative nausea and vomiting, Apgar score, postoperative pain severity and maternal satisfaction. A Significance level was determined at ?< 0.05 to decide the significance of statistical tests.
Ethical consideration
Ethical clearance was obtained from Research and Ethics Committee (REC) of medical faculty, Addis Ababa University. Official letter was also written from Addis Ababa City Administration Health Bureau to Gandhi Memorial Hospital. More importantly informed consent was obtained from all participants and confidentiality of the data was ensured.
Socio-demographic characteristics
The total response rate of the study was 120 (100 %). The mean age of mothers were 28 (SD ± 5) and 27 (SD ± 5) for spinal and general groups respectively. The mean body max index of mothers were comparable among each groups, which accounts 24.3 (SD ± 4.2) and 24.2 (SD ± 4.3) for spinal and general groups respectively. The majority of cases were house wife (61.7%), Orthodox Christian followers (67.5%) and Amhara ethnic group (45.8%) by ethnicity. In terms of procedures all cases were performed by residents and majority of cases (90%) were managed by BSc Anesthetists (Table 2).
| Variable | Number [%] | Number [%] | Total |
|---|---|---|---|
| General | spinal | ||
| Age (Mean ± SD) | 27±5 | 28±5 | |
| 15-19 | 2[3.3] | 1[1.7] | 3[2.5] |
| 20-24 | 18[30] | 15[25] | 33[27.5] |
| 25-29 | 20[33.3] | 26 [43.3] | 46[38.3] |
| 30-34 | 14[23.3] | 11[18.3] | 25[20.8] |
| 35-39 | 6[10] | 6[10] | 12[10] |
| 40-45 | 0[0] | 1[1.7] | 1[0.8] |
| BMI (Mean ± SD) | |||
| <18.5 | 1[1.6] | 1[1.6] | 2[1.6] |
| 18.5-24.9 | 23[38.3] | 40[66.7] | 63[52.5] |
| 25-29 | 20[33.3] | 11[18.3] | 31[51.7] |
| 30-35 | 6[10] | 6[10] | 12[10] |
| >35 | 0[0] | 2[3.3] | 2[1.67] |
Table 2: Socio-demographic characteristics of patients who underwent C/S under
general and spinal anesthesia in Gandhi Memorial Hospital, Addis Ababa, July
2014
Types of anesthesia administered and qualification of anesthetists
The majority of cases were managed by BSc anesthetists and no cases were operated under spinal anesthesia by master anesthesia professionals as shown in (Figure 1)
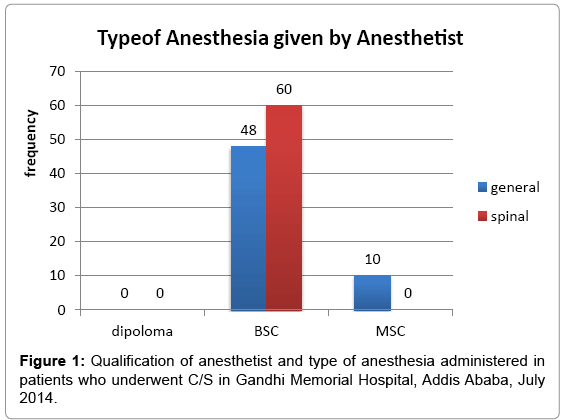
Figure 1: Qualification of anesthetist and type of anesthesia administered in patients who underwent C/S in Gandhi Memorial Hospital, Addis Ababa, July 2014.
Preoperative related history of study participants
Among the total cases, majority of cases (65%) were emergencies patients that underwent caesarean section for general and spinal anesthesia. About 57.5% of cases had no history of previous caesarean section. The mean preoperative systolic blood pressure was 129 (SD ± 12.5) and 128 (SD ± 12.6) for spinal and general groups respectively. The preoperative hematocret (Hct) was 38.6 (SD ± 3.4) and 39.6 (SD ± 4.8) for spinal and general respectively (Table 3).
| Variables | Number [%] | Number [%] | Total |
|---|---|---|---|
| ASA | General | Spinal | |
| ASAI | 51[85] | 104[86.7] | 53[88.3] |
| ASAII | 9[15] | 7[11.7] | 16[13.3] |
| Urgency of caesarean section | |||
| Elective | 21[35] | 21[35] | 42[35] |
| Emergency | 39[65] | 39[65] | 78[65] |
| Previous caesarean section | |||
| Yes | 23[38.3] | 28[46.7] | 51[42.5] |
| No | 37[61.7] | 32[53.3] | 69[57.5] |
| Preoperative Hct | |||
| Mean ±SD | 38.6 ±3.4 | 39.6 ±4.8 | |
| Mean preoperative systolic BP | |||
| Mean ±SD | 129 ±12.5 | 128 ±12.6 |
Table 3: Preoperative characteristics of patients who underwent C/S under general and spinal anesthesia in Gandhi Memorial Hospital, Addis Ababa, July 2014
Intraoperative outcomes of study participants
Among the study cases, there were no incidence of maternal death and cardiac arrest in both groups. The mean of intraoperative systolic and diastolic blood pressure under spinal was 103 (SD±14.3 and 58.9 (SD ± 10) and it was significantly lower than under general type of anesthesia 124 (SD±10.50) and 73.6 (SD ± 10) (Table 3).
The mean differences of intraoperative systolic and diastolic Blood pressure in cases under spinal and general were significantly associated in independent T test. T (118)=9.19, and t (118)=8.1 at p<0.0005, for systolic and diastolic blood pressure respectively. However, there was no significant difference on intraoperative vasopressor requirement between general and spinal anesthesia groups, (P>0.1095). Estimated blood loss was significantly lower under spinal anesthesia than general anesthesia, χ2 (2)=14.942, p<0.005.
The mean time from skin to uterine incision under spinal anesthesia was 3.5 (SD ± 1.6) and was not significantly different from the meantime from skin to uterine incision under general anesthesia, which accounted 3.4 (SD ± 1.9), p>0.609. In the two tailed statistical analysis, the difference in mean duration of anesthesia under spinal and general anesthesia were not showed significant under spinal anesthesia 43 (SD±10.4) and general anesthesia 44.4 (SD ± 18), t (118) = 0.324, P>0.747 (Table 4).
| Variables | Number [%] | Number [%] | Total |
|---|---|---|---|
| General | spinal | ||
| Mean intraoperative BP | |||
| Systolic (Mean ±SD) | 124 ±10.5 | 103 ±14.3 | |
| Diastolic (Mean ±SD) | 73.6 ±10.3 | 58.9 ±9.6 | |
| Vasopressor used | |||
| Yes | 2[3.3] | 5[8.3] | 7[5.8] |
| No | 58[96.7] | 55[91.7] | 113[94.2] |
| EBL | |||
| <500 | 14[23.3] | 33[55] | 47[39.2] |
| 500-1000 | 42[70] | 27[45] | 69[57.5] |
| >1000 | 4[6.7] | 0[0] | 4[3.3] |
| Time from skin to uterine incision | |||
| Mean ±SD | 3.4 ±1.9 | 3.5 ±1.6 | |
| Time from uterine incision to baby out | |||
| Mean ±SD | 1.9 ±2 | 1.5 ±0.8 |
Table 4: Intraoperative characteristics of patients who underwent C/S under General and spinal anesthesia in Gandhi Memorial Hospital, Addis Ababa, Ethiopia, 2014
Intraoperative neonatal outcomes among the study cases
There was no neonatal incidence of death under both general and spinal anesthesia. However, there was one neonatal incidence of cardiac arrest under general anesthesia (Table 5).
| Variables | Number [%] | Number [%] | Total |
|---|---|---|---|
| General | spinal | ||
| Apgar score 01 min | |||
| 0-3 | 3[5] | 1[1.7] | 4[3.3] |
| 7-Apr | 5[8.3] | 15[25] | 20[16.7] |
| 10-Jul | 52[86.7] | 44[73.3] | 96[80] |
| Apgar 05min | |||
| 7-Apr | 3[5] | 1[1.7] | 4[3.3] |
| 10-Jul | 57[95] | 59[98] | 116[96.7] |
| Oxygen requirement | |||
| Yes | 7[11.7] | 5[8.3] | 12[10] |
| No | 53[88.3] | 55[91.7] | 108[90] |
| Incidence of cardiac arrest | |||
| Yes | 1[1.7] | 1[0.8] | 0[0] |
| No | 59[98] | 60[100] | 119[99.2] |
Table 5: Intraoperative neonatal outcomes who delivered under spinal and general anesthesia in Gandhi Memorial Hospital, Addis Ababa, July 2014
There was a significant association between type of anesthesia and first minute Apgar score (p<0.026). Moreover,there were no significant association between groups in fifth minute Apgar score (p>0.381) and neonatal oxygen requirement (p > 0.301) and incidence of neonatal cardiac arrest (P>0.5)
Postoperative maternal outcomes among the study cases
The median time of first analgesic request was higher in spinal anesthesia group cases (93±4.2) minutes than general anesthesia groups (80±3.9) minutes. The man Whitney test was used to test the mean time difference of the first time analgesic request and it was found to be significant level (p< 0.0005).
Incidence of postoperative nausea and vomiting was higher in women under spinal anesthesia (73.3%) when compared to general anesthesia (6.7%). There was a significant relationship between types of anesthesia and postoperative nausea and vomiting on chi- squared independent test (p<0.00025).
There was no significant mean difference between spinal and general groups for postoperative pain severity assessment on Visual Analogue Score (VAS) of 2hrs, t (118) =1.621, P>0.054, one tailed. However, there were mean differences between spinal and general groups for postoperative pain severity assessment on VAS of 6 and 24hrs, (t (118) =-3.154, p<0.0001 and t (118) =-3.413, P<0.005, one tailed) respectively.
There was no significant association on regular pain measurement after two hours postoperatively (P>0.08, two tailed). However; there were a significant association on regular pain measurement at 6 and 24 hrs postoperatively (p<0.01 and 0.020, two tailed) respectively.
Chi square analysis was assumed and was not satisfied the criteria and the fisher’s exact test was used and it was found that there was no significant relationship (P>0.532, 2-tailed) (Figures 2 and 3).
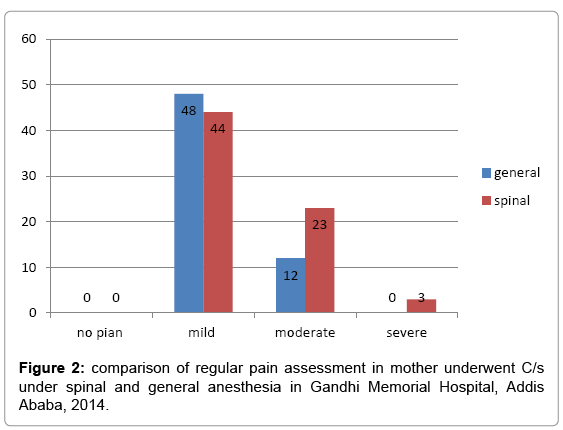
Figure 2: comparison of regular pain assessment in mother underwent C/s under spinal and general anesthesia in Gandhi Memorial Hospital, Addis Ababa, 2014.
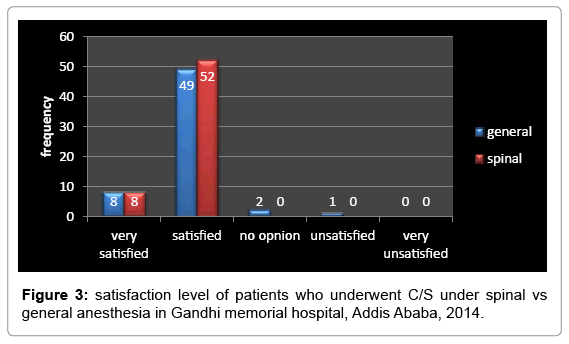
Figure 3: satisfaction level of patients who underwent C/S under spinal vs general anesthesia in Gandhi memorial hospital, Addis Ababa, 2014.
Factors affecting maternal and neonatal outcomes
Among the preoperative variables, only types of anesthesia was significantly associated with postoperative nausea and vomiting at P<0.05. Incidence of postoperative nausea and vomiting was nearly thirty nine times more common in spinal anesthesia than general anesthesia; OR= 38.5, 95% CI= (12, 123). However, the risk of developing postoperative nausea and vomiting was 15 times more common in spinal anesthesia than general anesthesia; RR= 15.0
Among the intraoperative variables, the mean intraoperative systolic and diastolic blood pressure, total Intravenous fluid requirement and vasopressor requirement were significantly associated with postoperative nausea and vomiting in spinal anesthesia (P< 0.05), but in general type of anesthesia, these variables did not show significant association.
Post operative nausea and vomiting was more likely in women with low mean intraoperative systolic blood pressure and low mean intraoperative diastolic blood pressure in spinal anesthesia than general anesthesia, (COR=1.06, 95% CI= [1.03, 1.09]) and (COR=1.08, 95% CI= [1.04, 1.11]) respectively. Pain severity assessment on Visual Analogue Score (VAS) after six and twenty four hours interval showed a significant association with PONV in spinal type anesthesia (P<0.05).
In multivariate analysis, types of anesthesia was the independent predictor of maternal outcomes (AOR=0.026, 95% CI= [0.01, 0.08]). Incidence of low Apgar score in first minute was three and half times more likely to occur in general anesthesia, (AOR=3.54, 95% CI= [1.26, 25.4].
This prospective observational study tried to compare maternal and neonatal outcomes in mothers who underwent caesarean section under General and spinal Anesthesia in Gandhi Memorial Hospital.
In this study there was no incidence of maternal and neonatal mortality between groups. This finding was inconsistent with other studies [4,5,8]. The reason might be due to appropriate perioperative patient care, short duration of follow up and /or relatively small sample size in our study.
Incidence of blood loss was more likely in general anesthesia than spinal anesthesia (AOR=8.2, 95% CI= [3.7, 18]. This finding was strongly supported the studies conducted in Ethiopia [9] and abroad [1,10]. The reason for such increase in blood loss under general anesthesia might be due to drugs that decrease uterine contraction (halogenated inhalational agents) and/or relative incensement in blood pressure in case of general anesthesia
In this study, there were a significant mean difference between the two groups regarding intraoperative mean systolic and diastolic blood pressure t (118) = 9.19, vs t (118) =8.1 at p < 0.0005, two tailed for systolic and diastolic blood pressure respectively. And the reason for this significant difference in blood pressure between the groups might be due to inadequate preloading of mothers who underwent spinal anesthesia; large doses of local anesthetic and extensive sympathetic blockade and or rapid infusion of large doses of oxytocine for uterine contraction.
Incidence of postoperative nausea and vomiting was higher in women under spinal anesthesia (73.3%) when it was compared to general anesthesia (6.7%). Incidence of postoperative nausea and vomiting was thirty eight and half times more common in spinal anesthesia than general anesthesia, (COR= 38.5, 95% CI= [12, 123]) which was comparable in a study conducted abroad [1] (COR = 23.22, 95% CI =[8.69, 62.03]). This might be due to associated with hypotension that stimulates the more vascular area, chemoreceptor trigger zone, on the floor of the fourth ventricle and rich in dopaminergic, histamine and other receptors that have many nerve fibers to Gastrointestinal tract via vagus nerve that causes nausea and vomiting; Uterogenic drugs used for uterine contraction also might contribute. But it needs further researching with clinical trial and large sample size.
The median time of first analgesic request in mothers underwent C/S under spinal anesthesia (93±4.2) minutes were longer compared to general (80 ± 3.9) group. A study conducted in Croatia (21) was in line with this study finding regarding first analgesic request (159 ± 39 vs 119 ± 44). However, the median times in this study were shorter compared to Croatian study findings and this might be due to patient variation, intraoperative drugs durations of action (analgesics, local anesthetics).
In this study pain severity assessment on VAS after two hours postoperatively was not significant on types of anesthesia administered. However, pain severity assessment on VAS after six hours (41 ± 15vs 32 ± 14 mm) and twenty four hours (20 ± 12 vs 13.81 mm) were significant in general and spinal at P<0.01 and P<0.02 respectively. In other study conducted abroad (21), the VAS scores in general and spinal after twenty four hours (59 vs 38mm) respectively were comparable to this study.
Unlike other studies7 this study did not show any significant difference in maternal satisfaction level on Anesthetic technique. The reason for this discrepancy might be due to maternal knowledge and attitude towards anesthesia before induction that they thought they could feel pain and even die under anesthesia and they were satisfied when things were not as they expected preoperatively
There was a significant association between types of anesthesia and better Apgar score of 01 minute in babies born under spinal anesthesia than general anesthesia. This finding is consistent with other studies conducted in Ethiopia [9] and abroad [1,3,6,11-12]. However, there was no significant association between types of anesthesia and Apgar score of 05 minute unlike other studies [3,9,11-12].
Incidence of lower mean intraoperative systolic and diastolic pressure was associated with spinal anesthesia. Even though the intraoperative blood pressure of general anesthesia groups was normal, estimated blood loss was higher than spinal anesthesia. Incidence of postoperative nausea and vomiting was higher in spinal anesthesia. The Apgar score of neonates in the first minute was lower in general anesthesia. However, there was no difference on Apgar score of five minute in both groups
Severity of pain assessment on VAS after six and twenty four hours postoperatively was higher in general anesthesia. Moreover there was no significant difference in General and spinal anesthesia on maternal satisfaction level.
Generally, it is not possible to say spinal anesthesia is superior over general on maternal and neonatal outcomes. Therefore, further research with clinical trial should be conducted