Medicinal & Aromatic Plants
Open Access
ISSN: 2167-0412
ISSN: 2167-0412
Review Article - (2014) Volume 3, Issue 1
Objective: Diabetes mellitus is a clinical syndrome characterized by a deficiency in insulin production or resistance to insulin action. Consequently, it leads to inappropriate hyperglycemia. Prolonged hyperglycemia can cause severe complications that probably affect every system of the body and every drug taken by the patient. This study highlights the most popular medicinal plants with potential antidiabetic significance, their modes of action together with the method used for their assessment.
Key findings: Through antidiabetic evaluation conducted on different medicinal herbs since centuries revealed the presence of potent antidiabetic activity. Moreover, the candidates from natural source with diverse structures of secondary metabolites. This indicates various sites of action within the human body. Conclusions: Further investigations are required, and more attention should be drawn to explore the biological activity of hundreds of traditionally used medicinal plants both in vitro and in vivo to assess the claimed activity with the aim of finding potent antidiabetic candidates from the natural resources.
Keywords: Medicinal plants; Antidiabetic agents; Herbs; Diabetes; Oral hypoglycemics
ALT: Alanine Transaminase; APDS: Allyl Propyl Disulfide; AST: Aspartate Transaminase; DM: Diabetes Mellitus; FBG: Fasting Blood Glucose; FPG: Fasting Plasma Glucose; FVO: Fructosyl Valine Oxidase Enzyme; GD: Gestational Diabetes; GHb: Glycated Hemoglobin; GIT: Gastro-Intestinal Tract; GLUT4: Glucose Transporter Type 4; HDL: High Density Lipoprotein; IDDM: Insulin Dependent Diabetes Mellitus; LD50: Lethal Dose 50; LDL: Low Density Lipoprotein; NIDDM: Non- Insulin Dependent Diabetes Mellitus; POD: Horse Radish Peroxidase; PPARα: Peroxisome Proliferator- Activated Receptor- Alpha; PPARδ: Peroxisome Proliferator-Activated Receptor- Delta; PPARγ: Peroxisome Proliferator-Activated Receptor- Gamma; RIA: Radioimmunoassay; STZ: Streptozotocin; THb: Total Hemoglobin; 3T3-L1: Cell Line Derived From Mouse; TZDs: Thiazolidinediones; UCP-1: Uncoupling Protein-1
Diabetes mellitus (DM) is a chronic disease characterized by a deficiency in insulin production and its action or both. That leads to prolonged hyperglycemia with disturbances in most metabolic processes inside the human body [1]. Untreated cases show severe tissue and vascular damage leading to serious complications such as retinopathy [2], neuropathy [3], nephropathy [4], cardiovascular complications [5] and ulceration [6]. Moreover, diabetes has an indirect relation with a many other diseases being the most common endocrine disorder. It was estimated that about 200 million people worldwide suffered from DM in 2010, and it is expected to reach 300 million by 2025 [7].
Both insulin and glucagon, pancreatic endocrine hormones, are responsible for controlling blood-glucose level within the body in an adequate level based on the body needs. Normally, insulin is secreted by the β-cells found at the islets of Langerhans in response to high levels of blood sugar. It potentiates the ability of muscle, red blood cells, and fat cells to absorb sugar out of the blood and consume it in other metabolic processes, which restore the sugar levels to the normal level [8].
On the contrary, glucagon is secreted by α- cells of the pancreas as a result of low blood-glucose level in between meals and during exercise. That stimulates the liver and other cells in muscles to release glucose out of the stored block in our bodies [8]. The harmonic relation between the two hormones, insulin and glucagon is shown in Figure 1.
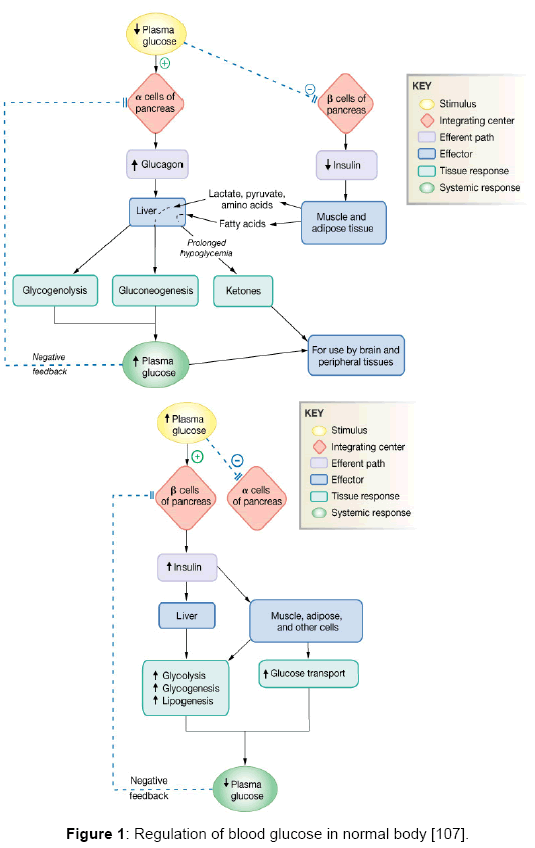
Figure 1: Regulation of blood glucose in normal body [107].
For better understanding DM, we write this piece of work about the disease, methods of diagnosis and treatment with special emphasis on naturally occuring secondary metabolites. Data were collected from different databases, including Pubmed, Google Scholar, Scifinder and Science Direct. Our aim is to present a scientifically relevant review for both researchers and readers, who are interested in the biologically active plants traditionally used in the treatment of diabetes. The possible mechanisms of action and common methods used for evaluation were also discussed.
Diabetes mellitus is classified into different categories, based on the etiology of the disease, but it is widely accepted that the two main types are; type 1 and type 2 [9].
Type 1 (IDDM) occurs in patients with little or no insulin secretory capacity. Consequently, they are in need for a replacement therapy of insulin for survival. The two major forms of type 1diabetes are type 1a (90% of type 1) and type 1b (10% of type 1). Type 1a results from immunological destruction of pancreatic ß cells associated with diseases such as Addison’s disease, Grave’s disease and Hashimoto’s thyroiditis [10,11]. However, type 1b is idiopathic where no etiological basis is identified. Some of these patients have predominant insulin deficiency and are susceptible to ketoacidosis, but no evidence of developing autoimmune diseases [12].
On the other hand, type 2 (NIDDM), is the most known form of diabetes, and it is characterized by abnormality in insulin secretion and its resistance [13]. Traditionally, it is predominant among elderly people (over 40 years). Commonly, it occurs in people with obesity, decreased body activity, and it may also be inherited [14]. The disease is often enhanced through dietary supplements, physical activity along with oral hypoglycemic agents [15].
Moreover, there is another temporary disease related to diabetes, which is known as gestational diabetes (GD) mellitus. It refers to the occurrence or initial recognition of glucose intolerance during the period of pregnancy [1]. Other types of diabetes include genetic abnormalities in the ß-cell of the pancreas or mutations in insulin receptor or post-receptor deformities [16]. Diseases of the exocrine pancreas such as pancreatitis, cystic fibrosis and excessive production of insulin counter regulatory hormones such as Cushing’s syndrome and acromegaly ultimately leads to DM [1]. Many drugs exemplified by glucocorticoids, niacin and interferon may induce DM [17].
Symptoms are nearly the same in the two major types of diabetes, but they differ in their intensity. The initial symptoms of untreated diabetic patients are attributed to elevated blood-glucose levels. Consequently, a loss of glucose in urine occurs, which increases urine output, leading to dehydration accompanied by thirst and raised water consumption. Insulin deficiency eventually results in weight loss in spite of an increase in appetite and food consumption. Untreated diabetic patients also suffer from fatigue, nausea and vomiting. They are susceptible to develop bladder, skin, and vaginal infections. Fluctuations in blood sugar levels can cause blurred vision. Moreover, very high sugar-levels can result in coma and even death [8].
The most popular methods for diagnosis of diabetes include the measuring of fasting plasma glucose level (FPG), which is done in the early morning. Patients with FPG below 100 mg/dl are considered normal; those between 100 and 125 mg/dl indicate pre-diabetic while those individuals with glucose levels above 125 mg/dl are considered diabetic [18].
The common strategy for treatment focused mainly on regulating and decreasing blood sugar to fall within the normal level. The main mechanisms in both traditional and Western medicines involve decrease blood sugar through stimulating pancreatic β-cells; inhibiting other hormones elevating blood sugar; increasing the affinity, and sensitivity of insulin receptor. On the other hand, lowering glycogen release; enhancing glucose utilization within many tissues and organs; clearing free radicals, resisting lipid peroxidation, correction of the lipid and protein metabolic disorders and improving human blood circulation are also involved [19].
The present oral antidiabetics (Figure 2) include sulfonyl ureas that decrease blood sugar, mainly by elevating insulin release from islets of Langerhans. They combine with sulfonylurea receptor on β-cells resulting in adenosine triphosphate–dependent potassium channels closure. Consequently, the cell membrane depolarizes and the subsequent calcium influx accompanied by secretion of stored insulin from secretory granules within the cells occurs. This mechanism works only in the presence of insulin [20,21].
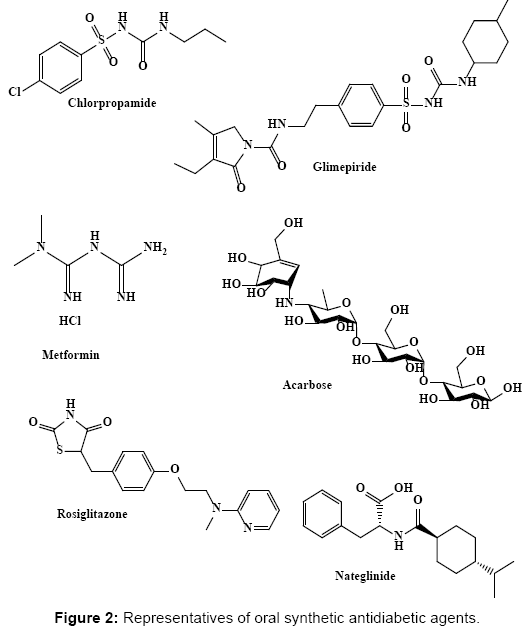
Figure 2: Representatives of oral synthetic antidiabetic agents.
Another known drug is the biguanides; they reduce hepatic gluconeogenesis and replenish peripheral tissues’ sensitivity to insulin through elevating insulin-stimulated uptake and utilization of sugar. However, biguanides are ineffective in insulin absence. The best example of this class is metformin [22].
The alpha-glucosidase inhibitors “starch blockers” inhibit certain enzymes responsible for the breakdown of carbohydrates in the small intestine. They act mainly by decreasing the rate of carbohydrate absorption in the body. Moreover, acarbose, an important example in this class, reversibly inhibits both pancreatic α-amylase and α-glucosidase enzymes by binding to the carbohydrate-binding region and interfering with their hydrolysis into mono-saccharides. This results in a slower absorption together with a reduction in postprandial blood-sugar levels [20,23].
Another important class of oral antidiabetic agents is the thiazolidinediones (TZDs). Their primary mechanism of action includes improving of muscle and adipose tissue sensitivity to insulin and to a smaller extent; reducing liver glucose production. TZDs are potent and selective agonists to the nuclear peroxisome proliferatoractivated receptor- gamma (PPARγ) present in liver, skeletal muscle and adipose tissue. Stimulation of such receptors controls the transcription of insulin-responsive genes involved in the regulation of transportation, production and glucose utilization. Moreover, it was shown that TZDs can enhance β- cell function by lowering free fatty acids levels that play an ultimate role in β-cell death [24].
The last class of commonly available oral hypoglycemics is the non- sulfonyl ureas secretagogues. This group increases the secretion of insulin from active β-cells by similar mechanism as sulfonyl ureas, but they bind to different β-cells receptors [25].
Natural products are the major mine for discovering promising lead candidates, which play an important role in future drug development programs. Ease of availability, least side effects and low cost make the herbal preparations are the main key player of all available therapies, especially in rural areas [26]. Since centuries, many plants are considered a fundamental source of potent anti-diabetic drugs. Although, synthetic oral hypoglycemics together with insulin are the main route for controlling diabetes. However, they exhibited prominent side effects and failed to reverse the course of its complications. This constitutes the major force for finding alternatives, mainly from plant kingdom that are of less severe or even no side effects [27]. In the following section, a compilation of the most famous plants widely used in folk medicine will be discussed. The aim of this review is not to mention all the antidiabetic plants previously discussed in details in the textbook of “Traditional Medicines for Modern Times Antidiabetic Plants” [28], but we will shed light on the most relevant data related to these popular plants. The most widely used antidiabetic herbs are highlighted below and summarized in Table 1.
| Therapeutic action | Botanical name |
|---|---|
| Acting like insulin [39] | Momordicacharantia Panax ginseng |
| Increasing insulin secretion from beta cells of pancreas [39] | Panax ginseng Allium cepa Azadirachtaindica Eugenia jambolana Pterocarpusmarsupium Medicago sativa |
| Regeneration of γ-cells of the islets of Langerhans [39] | Morusbomoysis Pterocarpusmarsupium Tinosporacordifolia Gymnemasylvestre |
| Reduction absorption of glucose from gastrointestinal tract [39] | Cyamposistertragonoloba Ocimum sanctum |
| Inhibition of aldose reductase activity[39] | Aralia elata |
| Increasing glucose utilization [39] | Zingiberofficinale Cyamospsistetragonolobus Grewiaasiatica |
| Reduction of lactic dehydrogenase and γ-glutamyl transpeptidase[39] | Lythrumsalicaria |
| Inhibition glycogen-metabolizing enzymes [39] | Allium sativum |
| Increasing glyoxalase 1 activity in liver [39] Increasing the creatine kinase levels in tissues [39] |
Trigonellafoenumgraecum |
| Inhibition of glucose-6-phosphate system [39] | Bauhinia megalandra |
| Oxygen radical scavengers [39] | Momordicacharantia |
| Protection of pancreatic beta cells from degeneration and diminish lipid peroxidation[63] | Morus alba |
Table 1: Classification of herbal antidiabetics according to their therapeutic action.
Aegle marmelos
It is commonly known as the Holy Fruit tree (Rutaceae). The oral administration of aqueous leaf extract to STZ diabetic rats was proven to be equally potent as insulin in normalizing blood glucose and insulin levels [29]. Its mode of action may be either due to stimulating glucose uptake or enhancing insulin secretion or both. In addition, it improved the functional state of the beta cells, regenerating the damaged pancreatic parts [30]. Moreover, the oral administration of its seeds aqueous extract showed a significant reduction in FBG level. Besides, it decreased total cholesterol level, LDL and triglyceride with concomitant elevation in HDL [31]. However, oral and intraperitoneal administration of the fruit aqueous extract showed antidiabetic activity in STZ induced diabetic rats. It significantly reduced the blood-glucose level as well as glycosylated hemoglobin, while elevating both serum insulin and liver glycogen. The fruit extract at a dose of 250 mg/kg was found to be more potent than glibenclamide [30].
On the other hand, A. marmelos methanol extract decreased blood sugar in alloxan diabetic rats, lowering its oxidative stress evidenced by reducing serum and liver lipid peroxidation, conjugated diene and hydroperoxide levels, elevating catalase, glutathione peroxidase, superoxide dismutase and reduced glutathione levels [32]. This relevant hypoglycemic effect is probably attributed to its coumarins. That stimulates insulin secretion from the pancreatic beta cells in the islets of Langerhans [30].
Allium cepa (Onion) and Allium sativum (Garlic)
They are important dietary supplements belonging to family Liliaceae that involved in the eastern kitchen. Studies showed that oral administration of the ethanol extract of garlic regulated the blood-sugar level, normalizing the activity of both liver hexokinase and glucose-6- phosphatase. In addition, it elevated liver glycogen, serum insulin as well as free amino acids, causing significant reduction in FBG, serum triglycerides, total cholesterol, urea, creatinine, AST and ALT levels [33]. The antidiabetic activity of the extract was more potent than glibenclamide, the commonly known antidiabetic drug [34].
Many onion bulbs ether fractions showed significant hypoglycemic effects by decreasing the glucose peak in subcutaneous glucose tolerance tests [29]. Among them, A. cepa increases the fasting serum high-density lipoprotein values, exhibiting alleviation of hyperglycemia in streptozotocin (STZ) diabetic rats. The hypoglycemic and hypolipidemic effects of onion were usually associated with a relevant antioxidant activity, as indicated by the increase in superoxide dismutase activity. No effects were observed on both lipid hydroperoxide and lipoperoxide levels [35].
The main active components present are sulfur-containing compounds being diallyl disulfide (allicin) in garlic and allyl propyl disulfide (APDS) in onions [36]. These active secondary metabolites present in the form of cysteine derivatives, as. S-alkyl cysteine sulfoxides that decompose upon extraction into polysulfides and thio-sulfinates in the presence of allinase. The potent antidiabetic activity of both plants may be attributed to the presence of these volatile decomposed products that predominate in their oils in addition to other nonvolatile sulfur-containing peptides and proteins [37].
Aralia elata
It is a woody plant belonging to the family Araliaceae, known also by Japanese angelica tree. The antidiabetic activity of its root cortex may be attributed to the presence of elatosides E together with oleanolic acid and its derivatives. These secondary metabolites lower the serum glucose level as shown by oral sugar tolerance test in rats [38]. The hypoglycemic activity of A. elata is mainly mediated through inhibition of aldose reductase activity [39].
Azadirachta indica
It belongs to the family Meliaceae and has been used for a long time in traditional medicine in treating several ailments, including diabetes. Its leaves stem bark and seeds possess hypoglycemic activity via increasing insulin secretion from the beta cells of the pancreas [39]. Its leaves are characterized by the presence of high fiber content that is potent in diabetes management and controlling of post-prandial hyperglycemia through delaying gastric emptying, increasing viscosity of GIT content thus, suppressing digestion and absorption of carbohydrate with no risk of hypoglycemia, hyperinsulinemia and undesirable weight gain [40].
Bauhinia candicans and B. forficate
They are medicinal plants native to Peru, Brazil and Argentina sub-tropical regions, belonging to family Caesalpinaceae the methanol extract of B. candicans leaves, together with its butanol exerted a potent antidiabetic activity reducing the plasma glucose level as well as urinary glucose excretion through enhancing peripheral glucose metabolism [41]. Administration of B. forficata leaves various extracts to alloxan-diabetic rats resulted in an obvious suppression in serum glucose, triglycerides and total cholesterol. Moreover, chromatographic purification of B. forficata leaves n-butanol fraction, resulted in the isolation of kaempferilrin, a flavonoid, which showed a potent hypoglycemic activity upon oral administration in alloxan-induced diabetic rats [42].
Biophytum sensitivum
It is an herbaceous plant native to Nepal widely reputed in folk medicine belonging to family Oxalidaceae. Its leaf extract exhibited a potent antidiabetic activity affecting glucose homeostasis. It caused a significant rise in serum insulin together with reduction in bloodglucose levels suggesting an insulinotropic effect mediated through enhancing the synthesis and/ or release of insulin from the pancreatic beta cells [43].
Brassica nigra
It belongs to family Brassicaceae and endogenously grows in the Mediterranean regions. The aqueous B. nigra seeds extract exhibited a potent antidiabetic activity in STZ induced diabetic rats manifested by significant reduction in fasting serum glucose, glycosylated hemoglobin and serum lipids exceeding that of ethanol, acetone and chloroform extracts [44]. Its mode of action is mainly attributed to stimulating insulin release from pancreas and normalizing the effects of glucose metabolizing enzyme, therefore, improving glucose homeostasis in both liver and kidney [45].
Cinnamomum zeylanicum
It is commonly known as Cinnamon (Lauraceae) and widely used in East Asia and Europe. It is extensively used in folk medicine to treat diabetes. It contains volatile oils, mainly cinnamaldehyde. Cinnamon ingestion decreased total plasma sugar level with insulin sensitivity improvement. It also significantly reduced gastric emptying and profoundly decreasing postprandial glycemic response [33]. In addition, cinnamon aqueous extract revealed a potent antidiabetic effect through its up regulation of uncoupling protein-1 (UCP-1) and enhancing the translocation of GLUT4 in the muscle and adipose tissues [46].
Oral administration of cinnamaldehyde, its chief active constituent, resulted in significant reduction in serum glucose, glycosylated hemoglobin, total cholesterol and triglyceride levels accompanied by a marked increase in serum insulin, hepatic glycogen and high-density lipoprotein in a dose-dependent manner [47].
Coptis chinensis (Huanglian)
It belongs to family Ranunculaceae and popularly used to alleviate diabetes in traditional Chinese medicine. Its antidiabetic activity is likely due to the presence of berberine, an isoquinoline alkaloid that predominates in plant roots, rhizomes, stems and barks. Studies showed that berberine produced significant reduction in blood-glucose level, plasma total cholesterol, triglycerides, and markedly decrease disaccharidases and β-glucuronidase activities in STZ-induced diabetic rats.
It successfully reduced body weight, increasing insulin response, enhancing glucose’s uptake by adipocytes via GLUT1, acetylcoenzyme a carboxylase phosphorylation, adenosine monophosphate-activated protein kinase. Moreover, it increased the PPARα/δ/γ protein expression in liver thus it potentiates insulin receptor expression in liver and skeletal muscle cells with concomitant improvement in glucose consumption, relieving some diabetic complications through marked regeneration in the damaged pancreas [48].
Cyamopsis tetragonoloba
C. tetragonoloba (Fabaceae) beans ethanol extract administered to alloxan-induced diabetic rats caused significant reduction in bloodglucose levels [49] which can be mediated through reduction of glucose absorption from gastrointestinal tract together with enhancing glucose utilization [39].
Eugenia jambolana
It is familiar by Jamun or black plum, belonging to family Myrtaceae. It is also known as Syzygium cumini and is widely being used over many centuries for the treatment of diabetes by the traditional practitioners. Oral administration of the pulp extract of the fruit resulted in the enhancement of insulinemia through insulin secretion stimulation and insulinase activity suppression from liver and kidney [29]. While, administration of the seeds dried alcohol extract resulted in hypoglycemia and decreased glycosuria, partially restoring the altered hepatic and skeletal muscle glycogen content as well as hexokinase, glucose-6-phosphatase, phosphofructokinase and glucokinase [50].
Moreover, the flavonoid rich extract of its seeds showed a potent antidiabetic activity manifested by a reduction in fasting and peak bloodglucose levels, in addition to an improvement in glycogen biosynthesis, glucose homeostatic enzymes’ activities as well as the in vitro insulin release from pancreatic islets. Its mechanism of action is probably due to up regulation of both PPARα and PPARγ in addition to its ability to differentiate 3T3-L1 preadipocytes [51]. Besides, seed kernel extracts were found effective in inhibiting α-glucosidase accounting for the mode by which this herb exerts its anti-diabetic effect [52].
Ficus bengalenesis
Oral administration of its bark aqueous extract exerted significant hypolipidemic, hypoglycemic and serum insulin increasing effects with intimate similarities to that exerted by a minimal dose of glibenclamide in STZ induced diabetic rats. It effectively reduced serum glucose level, normalizing serum electrolytes levels, glycolytic enzymes and hepatic cytochrome P-450 dependent enzyme systems accompanied by reduction in liver and kidney lipid peroxides. This was further confirmed by histological studies of the dissected pancreatic sections [53]. This is mainly attributed to its leucopelargonidin glycoside content. In addition, pelargonidin was more effective than leucocyanidin in enhancing the in vitro release of insulin by the pancreatic beta cells [33].
Grewia asiatica
It is known as Phalsa or Falsa belonging to family Malvaceae, native to southern Asia, and commonly cultivated in tropical countries. Ethanol extracts of its fruit, stem bark and leaves orally administered elicited an observable reduction in serum glucose level of alloxan induced diabetic rabbits. This anti-hyperglycemic may be mediated by its antioxidant and radical scavenging activity rather than by stimulating the release of insulin [54].
Gymnema sylvestre
A member of family Asclepiadaceae, which is widely known as gurmar. It is a woody, climbing plant; its main constituents are gymnemic acid, gurmarin, a polypeptide of 35 amino acids and saponins [34]. G. sylvestre leaves extract exhibited a potent antidiabetic activity in type 2 diabetes, as evidenced by causing a prominent suppression in bloodglucose, glycosylated hemoglobin and glycosylated plasma proteins together with restoring blood glucose homeostasis in type 2 diabetic patients. These results postulated that the beta pancreatic cells may be regenerated by G. sylvestre leaves extract supplementation and further confirmed by insulin levels elevation in patients serum [55].
Moreover, studies revealed that G. sylvestre enhanced the production of endogenous insulin without direct effect on the metabolism of carbohydrate. It was found that gymnemic acid prevents taste buds activation by sugar molecules, curbing the sugar craving by filling the receptor locations on the taste buds. Similarly, it occupies the receptor location in the intestine absorptive external layers thus inhibiting the sugar molecules uptake by the intestine, resulting in obvious reduction in plasma sugar level [29].
Lawsonia inermis
It is a popular member of family Lythraceae, which is commonly known as Henna, its leaves is found to constitute carbohydrates, flavonoids, proteins, phenolic compounds, tannins, terpenoids, alkaloids, quinones, xanthones, coumarins, as well as fatty acids [56]. Oral administration of 70% ethanol as well as 95% methanol extracts of the whole plant exhibited potent hypoglycemic and hypolipidaemic activities in alloxan induced diabetic mice causing significant reduction in serum glucose, cholesterol and triglycerides levels exceeding the effect of glibenclamide [57,58].
Lythrum salicaria
It is a member of family Lythraceae, commonly found in Europe, Asia, southeastern Australia and northwest Africa. It is also known as Purple loosestrife. L. salicaria stem and flower ether extracts caused a significant depression in serum glucose upon oral administration accompanied by an elevation in circulating insulin levels [59]. Its promising antidiabetic activity, mostly due to its richness in phenolic compounds, mainly tannins [60].
Medicago sutivu
It is a perennial flowering plant belonging to family Fabaceae, known by Alfalfa and also called Lucerne. It is commonly used in traditional medicine to treat diabetes. Administration of its aqueous extract alleviated hyperglycemia in STZ-diabetic mice via stimulating 2-deoxy-glucose transport in addition to glucose oxidation, and conversion of glucose to glycogen in mouse abdominal muscle. It also potentiated insulin secretion from the pancreatic β-cells. This insulinreleasing effect was also observed in both methanol and water fractions suggesting the synergistic effect of various extract constituents [61].
Momordica charantia
A well-known plant (bitter melon) belonging to family Cucurbitaceae that widely used in folk therapy for the treatment of diabetes. Oral administration of the fruit juice or seed powder resulted in a significant decline in FBG and pronounced amelioration of glucose tolerance exerting both insulin secretagogue and insulinomimetic activities [62]. This potent antidiabetic activity mainly attributed to the presence of an insulin-like polypeptide known by polypeptide- P, similar in structure to the bovine insulin, which reduces plasma sugar levels when injected subcutaneously into type I diabetic patients and appears to inhibit gluconeogenesis. In addition, it improves glucose tolerance in type II diabetes [29,33]. Other reported hypoglycemic agents isolated from M. charantia comprise the sterol glucoside mixture charantin isolated from fruit and the pyrimidine nucleoside vicine abundant in the seeds [62].
Morus alba
It is a member in family Moraceae, and is known as mulberry. The flavonoids rich fraction of the Egyptian Morus alba root bark 70% alcohol extract exhibited hypoglycemic activity in STZ diabetic rats upon oral administration. It significantly decreased the value of the blood-sugar level through protection of pancreatic beta cells from being degenerated and diminishing lipid peroxidation through reduction of lipid peroxides. Its detailed phytochemical investigation revealed the presence of four hydrophobic flavonoids namely morusin, cyclomorusin, neocyclomorusin, and kuwanon E, a 2-arylbenzofuran, moracin M, and two triterpenes, betulinic acid and methyl ursolate that may account for its antidiabetic potency [63].
Murraya koeingii
The curry leaf tree belonging to family Rutaceae is widely cultivated for its aromatic leaves, which are used as a flavoring agent. It was reported that an oral administration of M. koeingii leaves showed potent hypoglycemic effect associated with an increase in hepatic glycogen content due to stimulated glycogenesis and suppressed glycogenolysis as well as gluconeogenesis [29]. It also prevented the β cells from damage, exhibiting antioxidant and free radical scavenging activity showing more efficacy than glibenclamide [64]. It effectively reverted serum urea, uric acid and creatinine to the normal levels, reflecting its protective effects on kidney in STZ-induced diabetic rats [65].
Another studies showed that single oral administration of variable doses of M. koeingii leaves aqueous extract exerted a pronounced antidiabetic activity in alloxan induced diabetic rabbits as evidenced by marked lowering in blood-glucose level and improvement in glucose tolerance suggesting the tendency of its usage as an adjunct to dietary supplement and drug therapy for adequate control of diabetes mellitus [66]. Moreover, intraperitoneal administration of mahanimbine, carbazole alkaloid isolated from its leaves, at doses of 50 and 100 mg/kg showed a marked hypoglycemic activity reducing fasting blood sugar, triglycerides, low-density lipoprotein, VLDL levels increasing HDL level [67].
Ocimum sanctum
It is commonly known as Holy basil (Labiateae). Administration of O. sanctum leaves alcohol extract, orally, significantly reduced glycemia and enhanced exogenous insulin action. Administration of leaf powder to healthy and diabetic rats resulted in reduction of FBG after one month [39]. Its pronounced therapeutic potential as antidiabetic agent can be attributed to the presence of eugenol, its chief active constituent, reducing elevated serum sugar, cholesterol triglyceride levels as well as lactate dehydrogenase, alanine transaminase, aspartate transaminase and alkaline phosphatase [68].
Panax ginseng
Ginseng root (Araliaceae) has been used for over 2,000 years in the Far East for its health-promoting activities. It contained triterpene glycosides (saponins), commonly referred to as ginsenosides, peptides, polysaccharides, fatty acids and polyacetylene alcohol [69]. The hypoglycemic effect of ginseng root may be attributed to blocking intestinal glucose absorption and inhibiting hepatic glucose- 6-phosphatase activity resulting in delaying of food digestion and carbohydrate absorption rate [70]. Ginseng polypeptide, isolated from the root was effective in decreasing liver glycogen and blood-sugar levels while, its aqueous extract showed a remarkable hypoglycemic activity, increasing insulin production, reducing pancreatic β-cells death and resistance to insulin, thus improving postprandial glycemia in diabetic patients [33].
However, intraperitoneal injection of P. ginseng berry extract significantly improved glucose tolerance associated with a marked decrease in serum insulin levels together with rise in energy expenditure and body temperature. Although, ginsenoside showed a potent antihyperglycemic action, it was not accompanied by body weight changes, postulating that other extract ingredients may distinctly energy metabolism by various pharmacological mechanisms. Additional site of action for ginseng berry is the gastrointestinal tract, it exerts postprandial hypoglycemia via gastric vagal afferents, inhibited brain stem neuronal activity [70].
Picrorrhiza kurroa
It belongs to family Scrophulariaceae, and is commonly known as Kutki. Its alcohol extract reduced the sugar level in alloxan-induced diabetic rats through acting as a free radical scavenger. It can also decrease elevated blood urea nitrogen, serum lipid peroxides levels as well as ameliorating white blood cells destruction, protecting vital tissues including the pancreas and inhibiting undesirable body weight loss thus reducing the causation of diabetes [50,64]. Picrosides from Katuki constituted the major active ingredient responsible for its potent hypoglycemic activity presenting a natural and safe remedy for prevention or delaying of diabetic complications [71].
Polygonati Odorati
It belongs to family Liliaceae, its aqueous extract showed potent antidiabetic activity influencing glucose or carbohydrate metabolism through inhibiting α-glucosidase activity in the digestive canal and thus improving glucose and triglyceride metabolism [72].
Psidium guajava
It is known as Guava belonging to family Myrtaceae. It contains a high percentage of vitamins B1, B2, B6, vitamin C, free sugars (glucose, fructose and sucrose) and carotene. Oral administration as well as intraperitoneal injection of aqueous leaves extract to alloxan-induced hyperglycemic rats has shown beneficial effect not only on bloodglucose but also on body weight, glucose and ketone level of urine and tissue of pancreas showing a marked inhibitory activity on protein tyrosine phosphatase1B [73].
While, the methanol extract showed hypoglycemic effect in type II diabetes. Flavonoid glycosides exemplified by pedunculagin, isostrictinin and strictinin are the potent constituents, that have been used in clinical treatment of diabetes to improve insulin sensitivity [33]. Additionally, P. guajava stem bark ethanol extract showed a marked hypoglycemic effect, which may not be due to stimulating insulin release from pancreatic β-cells, but may be attributed to extra pancreatic mechanism exemplified by enhancing peripheral glucose metabolism [74].
Pterocarpus marsupium
It is also known as Vijayasar or the Indian Kino Tree belonging to family Fabaceae. The hypoglycemic effect of various extracts from P. marsupium bark was obvious in alloxan-induced diabetic rats. The results confirmed their efficacy on plasma glucose, total protein, cholesterol, triglycerides, alkaline phosphatase, alanine transaminase and aspartate transaminase. Moreover, butanol sub-fraction a marked hypoglycemic effect by adjusting body metabolism similar to insulin properties [75]. Marsupsin and pterostilbene, phenolic constituents of the heartwood of P. marsupium, significantly reduced blood-glucose level of approaching that of metformin [76].
Tecoma stans (Bignoniaceae) and Teucrium cubense (Lamiaceae)
These plants were mainly used as a diabetes mellitus remedy. Their aqueous extracts exert a potent antidiabetic activity via enhancing glucose uptake in both insulin-sensitive and insulin-resistant murine and human adipocytes with no marked proadipogenic or antiadipogenic adverse effects [77].
Tinospora cordifolia
It is commonly known as Gaduchi a member of family Menispermaceae. It is widely used as tonic and for treatment of endocrine metabolic disorders, including diabetes. The major constituents are diterpenoids, alkaloids, steroids, lactones, glycosides, phenolics, aliphatic compounds, sesquiterpenoid, and polysaccharides. Oral administration of T. cordifolia root aqueous or alcohol extracts to alloxan diabetic rats produced a significant antidiabetic effect through enhancing the glucose metabolism as evidenced by an obvious suppression in plasma glucose, brain lipid values, serum acid phosphatase, alkaline and lactate dehydrogenase and hepatic glucose- 6-phosphatase, with consequent elevation in body weight, hepatic hexokinase and total hemoglobin [29].
However, no pronounced effect on regeneration of β-cells of the islets of Langerhans was observed as confirmed by the histological examination of the pancreas. Moreover, T. cordifolia aqueous extract exerted certain inhibition on adrenaline-induced hyperglycemia while its ethyl acetate root extract showed certain antidiabetic potency that may be attributed to the presence of a pyrrolidine derivative [78].
Trigonella foenumgraecum
It is commonly known by Fenugreek seeds and is belonging to family Fabaceae. It is famous for the presence of mucilage, proteins, proteinase inhibitors, steroid saponins and saponin-peptide esters, sterols, flavonoids, nicotinic acid, coumarin, trigonelline and volatile oil [79]. Administration of the defatted seed decreased fasting and postprandial blood levels of glucagon, glucose, insulin, somatostatin, triglycerides, total cholesterol, while increased HDL-cholesterol levels. The intake of seed fiber of T. foenumgraecum decreases sugar absorption rate, delaying gastric emptying, thus inhibiting the increase in bloodglucose levels after meals. It also stimulates insulin receptor sites to burn cellular glucose at high-fiber diet. Its chemical analysis revealed that galactomannan constituted the major ingredient that of the seed fiber to which the antidiabetic activity may be attributed [80,81].
The underlying mechanism by which fenugreek seeds act as an orally effective hypoglycemic agent may be achieved through enhancing insulin synthesis and its release from the beta pancreatic cells of the islets of Langerhans. The relevant therapeutic role of Trigonella powdered seed in type 1 diabetes mainly attributed to the reversion of lipid and glucose metabolizing enzyme activities to normal levels, thus stabilizing glucose homeostasis in the liver and kidney [36].
Zingiber officinale
It is commonly known as ginger, belonging to family Zingiberaceae. The juice of Z. officinale rhizome exhibited a pronounced increase in serum insulin together with a marked decrease in FBG levels in STZinduced diabetic rats. It also exerted suppression in serum cholesterol, triglyceride and blood pressure in diabetic rats. This glycemic control particularly involves serotonin (5-HT) receptors [82]. Ginger extracts stimulate the 3T3-L1 preadipocytes differentiation. Recent studies showed that gingerol, its chief active constituent, enhanced cell-mediated glucose uptake via increasing insulin-sensitivity, thus improving chronic disease, as diabetes [83].
Based on the aforementioned examples of natural antidiabetic agent, a summary of most plants used in folk medicine for the treatment of diabetes mellitus is tabulated at the end of the review (Table 1) [39].
Many classes of plants secondary metabolites, such as alkaloids, terpenoids, phenolics, flavonoids and many others (Figure 3) show promising antidiabetic potentials. These natural constituents may act as a promising source of delivering oral hypoglycemic effect with minimal side effects. Citing all natural antidiabetics is out of the scope of this review; however, most biologically relevant secondary metabolites are briefly summarized in Table 2. The wide range of phyto-constituents structures, which appear to be promising hypoglycemic agents, suggests variable sites of action inside our body.
| Class of Natural Compounds | Name | Occurrence | Pharmacological action & Uses |
|---|---|---|---|
| Alkaloids | Casuarine 6-O-α-glucoside | Syzygiummalaccense (Myrtaceae) [19] |
α-Glucosidase inhibitor |
| Isoquinoline alkaloids: Schulzeines A, B and C |
Marine sponge Penaresschulzei [95] |
α-Glucosidase inhibitor | |
| Tecomine 5β-Hydroxyskitanthine Boschniakine |
Tecomastans(Bignoniaceae) [96] | Stimulate basal glucose uptake rate in rat adipocytes | |
| Two new pyrrolidine alkaloids : Radicamines A and B |
Lobelia chinensis(Campanulaceae) [97] | α-Glucosidase inhibitor | |
| Three quinolizidine alkaloids: Javaberine A Javaberine A hexaacetate and Javaberine B hexaacetate |
Talinumpaniculatum (Portulacaceae) [19] |
Inhibitors of TNF-α production by macrophages and fat cells. Dietary supplement for prevention of diabetes |
|
| Three quinolizidine alkaloids: Lupanine 13-α-Hydroxylupanine 17-Oxo-lupanine |
Lupinusperennis(Fabacae) [98] | Glucose-induced insulin release enhancement from isolated rat islet cells which was dependent on the glucose concentration. | |
| Five isoquinoline alkaloids Berberine chloride Berberine sulfate Berberine iodide Palmatine sulfate Palmatine chloride |
Coptis japonica (Ranunculaceae) [99] |
Aldose reductase inhibitor | |
| Flavonoids | 6-Hydroxyapigenin 6-Hydroxyapigenin-7-O-β-D-glucopyranoside 6-Hydroxyluteolin- 7-O-β-D-glucopyranoside 6-Hydroxyapigenin-7- O-(6-O-feruloyl)-β -D-glucopyranoside 6-Hydroxyluteolin-7-O-(6-O-feruloyl)-β-D-glucopyranoside |
Origanummajorana (Lamiaceae) [100] |
α-Glucosidase inhibitor |
| Myrciacitrin I, II, III, IV and V | Myrciamultiflora. (Myrtaceae) [101] | Aldose reductase inhibitory activity. | |
| Quercetin 3-O-α-L-arabinopyranosyl-(1→2)-β-D-glucopyranoside Kaempferol 3-O-β-D-glucopyranoside (astragalin) Quercetin 3-O-β-D-glucopyranoside (isoquercitrin) |
Eucommiaulmoides (Eucommiaceae) [19] |
Glycation inhibitors | |
| Terpenes | Lactucain A, B and C | Lactucaindica (Compositae) [102] |
Moderate lowering of plasma glucose |
| 3 ,22 -Dihydroxyolean-12-en-29-oic acid Tingenone Tingenine B Regeol A Triptocalline A Mangiferin |
Salaciachinensis(Celastraceae) [103] | Aldose reductase inhibitory activity | |
| Centellasaponin A | Centellaasiatica (Apiaceae) [19] |
Aldose reductase inhibitory activity | |
| Abietane-type diterpenoids: Danshenols A and B Dihydrotanshinone I Tanshinone I Cryptotanshinone Tanshinone IIA (-)-Danshexinkun A |
Salvia miltiorrhiza (Labiatae) [104] |
Aldose reductase inhibitory activity | |
| Triterpenedehydrotrametenolic acid | Sclerotia of Poriacocos(Polyporaceae) [105] | Insulin sensitizer | |
| Corosolic acid (GlucosolTM) | Lagerstroemia speciosa(Lythraceae) [106] | Glucose transport-stimulating activity | |
| Phenolics | 7’-(3’,4’-Dihydroxyphenyl)-N-[(4 methoxyphenyl)ethyl]propenamide 7’-(4’-Hydroxy-3’methoxyphenyl)-N-[(4butylphenyl)ethyl]propenamide |
Cuscutareflexa(Convovulaceae) [19] | α-Glucosidase inhibitor |
| (7S,8S)-Syringoylglycerol 9-O-β-D-glucopyranoside (7S,8S)-Syringoylglycerol-9-O-(6’- O-cinnamoyl)-β-D-glucopyranoside |
Hyssopusofficinalis(Lamiaceae) [19] | α-Glucosidase inhibitor | |
| Tetra- and penta-O-galloyl-β-D-glucose | Glycyrrhizaeuralensis (Leguminosae) Paeonialactiflora(Ranunculaceae) [19] |
Potent aldose reductase inhibitory activities. |
Table 2: Representatives of major classes of secondary metabolites showing antidiabetic activity.
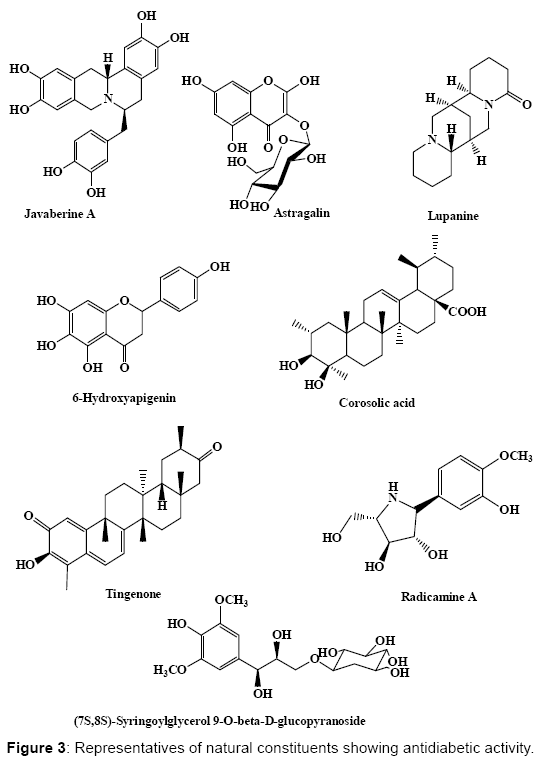
Figure 3: Representatives of natural constituents showing antidiabetic activity.
Assessment of the antidiabetic activity of different medicinal plant extracts, fractions as well as isolated compounds with the aim of finding promising candidates for the treatment of this widely spread disease could be achieved through preparation of various plant extracts, followed by preliminary phytochemical screening [84], lethal dose LD50 determination for the most relevant ones [85]. In vitro followed by in vivo antioxidant determination for the selected extracts and fractions will give a preliminary prediction for their antidiabetic activity. Pharmacological assessment for the most active candidates will be determined through measuring different biochemical parameters. This includes evaluating the serum glucose [86], serum insulin [87], glycosylated hemoglobin [88], total cholesterol [89], triglyceride [90], serum urea [91], serum creatinine [92], and plasma alanine transaminase (ALT) and plasma aspartate transaminase (AST) [93]. Finally, the antidiabetic activity will be further confirmed through microscopical examination of the histopathological pancreatic sections.
Serum glucose being the most important biochemical parameter for the evaluation of the antidiabetic can be assessed using the oxidase method, which principally based upon the oxidation of glucose to gluconic acid and hydrogen peroxide in the presence of glucose oxidase. Then, in the presence of peroxidase hydrogen peroxide combines with 4-aminophenazone and phenol to form a pink colored quinoneimine dye. Its intensity is subsequently measured at 546 nm and is directly proportional to the glucose concentration present in the specimen [86].
Serum insulin is also one of the most decisive parameters in the estimation of hypoglycemic activity. It is evaluated using the radioimmunoassay (RIA) kit, which is a double-antibody batch method illustrated in Figure 4. Insulin in the sample competes with a fixed amount of 125I-labelled insulin for specific antibody’s binding sites. Then, addition of a second antibody is used to cause an effective separation of bound and free insulin followed by centrifugation and finally decantation. The radioactivity in the pellet is subsequently measured, and it is inversely proportional to the quantity of insulin present in the sample. This test is effective in the determination of insulin levels in the bloodstream and is also useful in the evaluation of pancreatic β-cell activity [87].
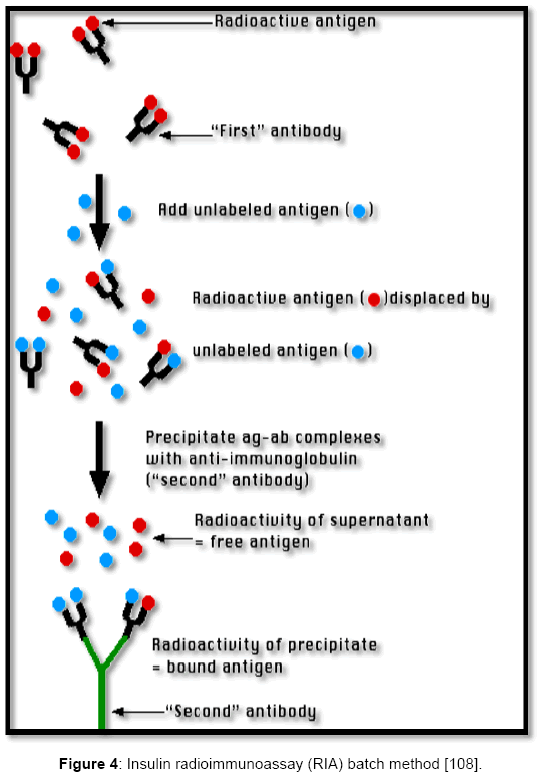
Figure 4: Insulin radioimmunoassay (RIA) batch method [108].
The last valuable parameter to be assessed is the glycosylated hemoglobin. It gives an indication on the blood-glucose level over the past period (usually three months). It is estimated by lysis of the blood specimen followed by exposure to severe protease digestion using Bacillus spp. protease. Amino acids, including glycated valines from the beta chains of hemoglobin are successfully released. These acids act as a substrate for recombinant fructosyl valine oxidase (FVO) enzyme, released by E. coli, which specifically cleaves N-terminal valines thus, producing hydrogen peroxide. The latter, is then evaluated using a horse radish peroxidase (POD) catalyzed reaction together with a suitable chromagen. For total hemoglobin estimation, it is performed through the conversion of all the specimen hemoglobin derivatives to hematin using an alkaline method. The blood specimens are then subjected to lysis with a consequent hemoglobin release. The same lysate undergoes two parallel tests; the first determines the glycated hemoglobin (GHb) content, while the second test evaluates total specimen hemoglobin (THb) content. Finally, HbA1c concentration is expressed as a concentration ratio of glycated hemoglobin to total hemoglobin [88].
Natural resources are still considered as potent candidates for drug discovery and are playing a pivotal role in drug development programs. Moreover, many medicinal herbs provide a rich mine for bioactive chemicals that are markedly free from undesirable side effects and of powerful pharmacological actions.
Nowadays, data on biological activities of many medicinal herbs are tremendously increasing. However, it is impractical to specify the performance of a multi-component mixture, as that present in plant extracts comprising a wide range of phytochemical constituents, to only a single component from that extract [94]. Secondary metabolites could act as lead compounds for the discovery of different new classes of possibly potent and safe antidiabetic agents. Further attention should be given for the identification of the typical modes of action of their extracts and the isolated pure compounds. However, because of the variable molecular biological reports, the field of speculations and interpretation seem to be infinite.
Consequently, much effort should be afforded to optimize a procedure for antidiabetic screening of different plants’ extracts as well as isolated bioactive compounds for the discovery of new natural herbal antidiabetic drugs. That can be used as alternatives to synthetic oral hypoglycemic drugs with less or even no prominent side effects.
The authors declare that they have no conflicts of interest to disclose.
This review received no grants from any funding agency in the public, commercial, or not-for-profit sectors.