Anatomy & Physiology: Current Research
Open Access
ISSN: 2161-0940
ISSN: 2161-0940
Review Article - (2017) Volume 7, Issue 6
Human Merkel cells (MCs) were first described by Friedrich S. Merkel in 1875 and named “Tastzellen” (touch cells). Merkel cells are primarily localized in the basal layer of the epidermis and concentrated in touch-sensitive areas. Their density varies among each anatomical site. Mostly they are concentrated in the palms of hands, predominantly in the finger pads, also in the soles and toes than in any other parts of the body. Concentration of MC in the external genitalia has not been studied, but some researchers detected some MCs in the male prepuce and in the female clitoris. Last year they were first described in the labia minora. Functionally they can be classified into some subpopulations with different functions: mechanoreceptive, endocrine, chemo sensitive. They belong to mechanoreceptors detecting tissue deformations and release various neurotransmitters to nerve endings. Tumor arising from Merkel cells called Merkel cell carcinoma (MCC). This highly aggressive malignancy occurs most often in the elderly white peoples on the skin of the head, neck and extremities. Its incidence is generally higher in men than in women. The rate of mortality is higher than in patients with melanoma and prognosis is rather poor. MCC of the genitourinary system are very rare, aggressive and may be misinterpreted with other cancers of genitourinary system. Most cases of MCC reported in the English literature in the women are in the vulva. In general MCC have an aggresive behavior, but those in the vulva are virulent with a 100% rate of inguinal node and also distant metastases. Prognosis of this carcinoma is very poor than prognosis of the MCC arising in other parts of the body.
Keywords: Merkel cells; Merkel-like cells; Merkel cell carcinoma; MCC; Female genitalia
Merkel cells
Merkel cells (MCs) (Figure 1a and 1b) are post-mitotic, neuroendocrine cells found in the epidermis of vertebrates [1,2]. They named according the German anatomist and histopathologic Friedrich Sigmund Merkel in 1875 (Figure 2) who first described these interesting cells. They were referred to as “Tastzellen” or “touch cells.” [3]. In the glabrous skin they formed clusters connected with nerve endings and named as “touch corpuscles” (Tastscheiben) [3]. The human and animal MCs have been a subject of investigation in many studies for over a century, but their distribution, function and origin still remain unclear [4]. These rare cells are found in the basal layer of the epidermis and grouped in touch-sensitive locations in glabrous and hairy skin and in some mucosa [2]. Their density varies among each anatomical sites [5,6]. Mostly they are concentrated in the palms of hands, predominantly in the finger pads, also in the soles and toes than in any other parts of the body [7]. They are also present in the lips, hard palate, gingiva [4], oesophagus [8], and human eyelid [9]. Concentration of MCs in the external genitalia has not been studied, but Cold and Taylor [10] detected some MCs in the male prepuce and in the female clitoris. Last year Schober et al. [11] first described MCs in the labia minora. There is no occurrence information about the MCs in the vagina. The regions richer in MCs are involved in tactile perception, underlining the sensory receptor function of MCs [12]. Functionally, they are in close contact with nerve fiber endings to form a synapse-like contact zone and receive all environmental stimuli [11]. Some MCs are not associated with nerve axons [13]. Characteristic features of MCs are: oval shape, size about 10-15 μm in diameter, large, pale, lobulated nucleus, spike-like cytoplasmic projections called „microvilli” which interdigitate with adjacent keratinocytes [14]. They are attached to the neighbouring keratinocytes by relatively few; small desmosomes located on the cell body and occasionally on the dendritic-like processes [15]. Ultrasturcturally, they have dense-core secretory granules in the cytoplasm near the nerve fiber connection [15]. Visualisation of MCs in routine light microscopy is not possible, therefore we need special technique for their identification [16,17]. Antibodies against simple-epithelial cytokeratines, especially anti CK type 20 provide the highest degree of specificity and give an easy identification of MCs at the light microscopic level [17]. Other identification method in light microscopy is based on incorporation of fluorescence FM-dyes [water-soluble, lipophilic, styryl, nontoxic dyes] into living MCs. [18]. The uranaffin reaction has been used in electron microscopy, to detect mammalian intraepithelial MCs [19]. Uranaffin reaction was introduced as an ultrastructural stain for the localization of adenine nucleotide in organelles storing biogenic amines [19]. According Lucarz and Brand [15], functionally they can be classified into some subpopulations with different functions: mechanoreceptive, endocrine, chemosensitive. They belongs to mechanoreceptors detecting tissue deformations and release various neurotransmitters to nerve endings [15,20]. Thanks to dense-core granules in the cytoplasm they were considered to be cells of APUD system [group of cells with endocrine functions] [15]. According some scientist [21,22], they may play role in the proliferation and differentiation of the keratinocytes. Presumptive functions of Merkel a cell summarize (Figure 3).
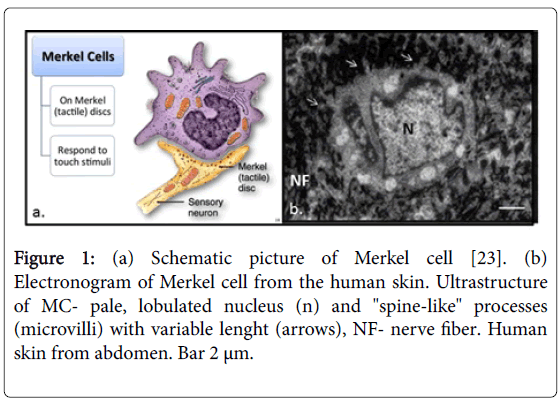
Figure 1: (a) Schematic picture of Merkel cell [23]. (b) Electronogram of Merkel cell from the human skin. Ultrastructure of MC- pale, lobulated nucleus (n) and "spine-like" processes (microvilli) with variable lenght (arrows), NF- nerve fiber. Human skin from abdomen. Bar 2 μm.
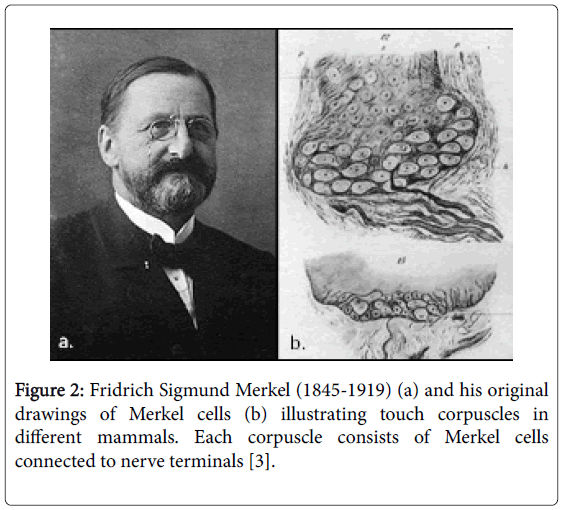
Figure 2: Fridrich Sigmund Merkel (1845-1919) (a) and his original drawings of Merkel cells (b) illustrating touch corpuscles in different mammals. Each corpuscle consists of Merkel cells connected to nerve terminals [3].
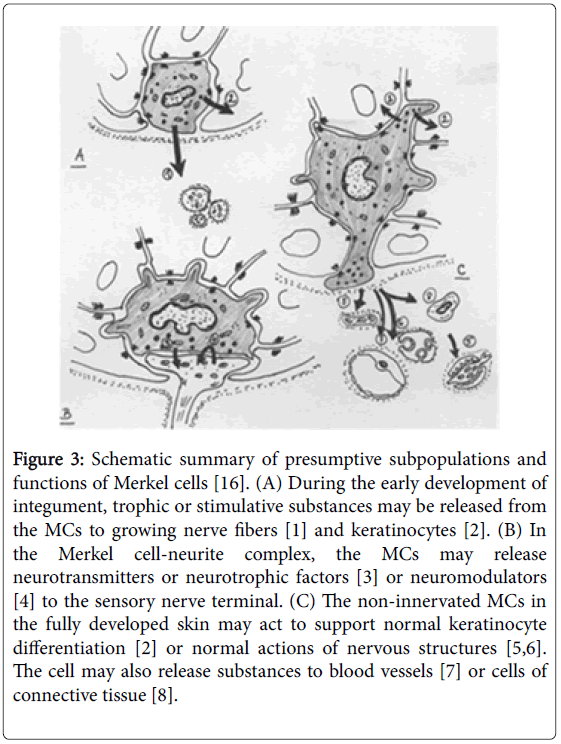
Figure 3: Schematic summary of presumptive subpopulations and functions of Merkel cells [16]. (A) During the early development of integument, trophic or stimulative substances may be released from the MCs to growing nerve fibers [1] and keratinocytes [2]. (B) In the Merkel cell-neurite complex, the MCs may release neurotransmitters or neurotrophic factors [3] or neuromodulators [4] to the sensory nerve terminal. (C) The non-innervated MCs in the fully developed skin may act to support normal keratinocyte differentiation [2] or normal actions of nervous structures [5,6]. The cell may also release substances to blood vessels [7] or cells of connective tissue [8].
Merkel cell carcinoma [MCC]
This rare neuroendocrine, cutaneous neoplasm was first documented and described by Toker in 1972 [24]. Typical predilection sites are sun-exposed skin regions e.g. head, neck and extremities of elderly persons. [25-27]. This highly aggressive malignancy occures most often in the white population [28,29]. The incidence of MCC is generally higher in men than in women. Risk group includes the elderly people with immunosuppression from organ transplant and HIV infection [27,30]. MCC presents as a firm, painless, red- violet, rapidly enlarging, cutaneous nodule (Figure 4) [25,27,31]. Ethiology of MCC is linked to the presence of clonally integrated Merkel cell polyomavirus (MCPyV) and/or mutagenesis from ultraviolet [UV] light exposure [32]. Histologically, the tumor commonly involves the full thickness of the dermis (Figure 5) and frequently extends into the subcutaneous fat and adjacent skeletal muscle [33]. Histologically, MCC has been classified into three distinct subtypes: trabecular, intermediate, small-cell type [33]. Diagnosis is based on typical histology representation on haematoxylin-eosin stained slides together with the results of immunohistochemistry [34].
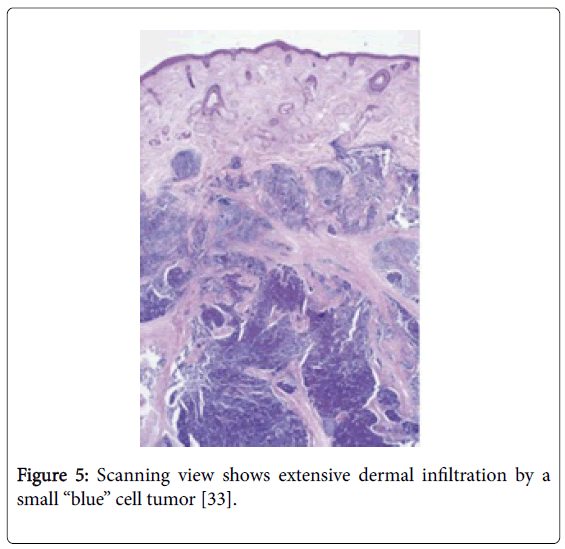
Figure 5: Scanning view shows extensive dermal infiltration by a small “blue” cell tumor [33].
v
CK-20 is specific, highly sensitive marker for MCC [positive in 89 to 100% of cases [35]. Mortality of the cancer is estimated to be between 33% and 46% [27,36] and the rate of mortality is higher than in patients with melanoma [27,37]. MCC is the second most common cause of death after melanoma [37,38]. Metastasis most commonly involved regional lymph nodes, followed by distant lung, skin, CNS, liver and bone [39]. The prognosis is rather poor. According by Kokoska [40] and Linjawi [41] the 2-year survival rate is 30%-50% in the patients of theirs study. Treatment, of MCC requires wide excision of the primary tumor, surgical biopsy of the draining lymph node bed, and adjuvant radiation therapy to the tumor bed and draining nodal basin [33]. Although the tumor is chemoterapy-sensitive, the role of chemotherapy is discutable, because responses to chemoterapy are seldom durable.
Merkel cell carcinoma [MCC] in the organs of genitourinary system
Primary MCCs of the genitourinary system are very rare, aggressive and may be misinterpreted with other cancers of genitourinary system. MCC of genitourinary tract occur in the patients aged between 30-80 years [42]. In the male genitourinary system, Best [43] reported case of MCC in the scrotum and Tomics [44] in the penis. Most cases of MCC reported in the English literature in the women are in the vulva (Table 1) [42].
| References | Age (y) | Location | Size (cm) |
|---|---|---|---|
| Tang et al., 1982 [45] | 67 | labium minus | 1,5 |
| Bottles et al., 1984 [46] | 73 | labium minus | 3 × 2 |
| Copeland et al., 1985 [47] | 59 | labium minus | 8 × 6 |
| Husseinzadeh et al., 1988 [48] | 47 | labium minus | 4,2 × 3 |
| Chandeying et al., 1989 [49] | 28 | labium minus | 4 |
| Cliby et al., 1991 [50] | 35 | vulva | low than 1 |
| Loret de Mola et al., 1993 [51] | 49 | Fourchette | 2 |
| Chen, 1994 [52] | 68 | vulva | 3 × 2,5 |
| Scurry et al., 1996 [53] | 68 | labium minus | 4 × 3 |
| Fawzi et al., 1997 [54] | 78 | vulva | 5,5 |
| Gil-Moreno et al., 1997 [55] | 74 | labium minus | 9 |
| Hierro et al., 2000 [56] | 79 | labium minus | 2,5 |
| Khoury-Collado et al., 2005 [57] | 49 | Bartholin gland | 2 |
| Pawar et al., 2005 [58] | 35 | labium majus | 6 × 4 |
| Mohit et al., 2009 [59] | 50 | labium majus | 12 × 10 |
| Sheikh et al., 2010 [60] | 63 | vulva | 7 × 5 |
| Lavazzo et al., 2011 [61] | 63 | labium majus | 9 |
Table 1: Merkel cell carcinoma of the vulva [42].
MCC arise from external squamous mucosa, Bartolin gland duct, or minor vestibular glands [40]. MCC in this location vary in size from 1-12 cm in the greatest dimension (Figure 6) [42]. MCC of the vulva presents as a firm, mobile mass with edema, erythema, ulceration and pain [35]. The work of Nguyen et al., [35] brings the main information about the clinical presentation (Table 2) and histopathological evaluation (Table 3) of the vulvar MCC.
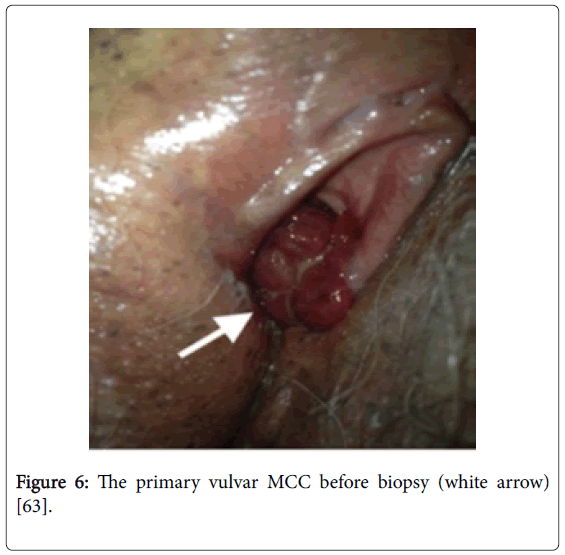
Figure 6: The primary vulvar MCC before biopsy (white arrow) [63].
| Clinical presentation of vulvar merkel cell carcinoma (35) | |
|---|---|
| (n=17) | |
| Characteristic | n (% or range) |
| Mean age (years) (28-79) | 59.6 |
| Mean tumor diameter (cm) (1.8-47.5) | 7.5 |
| Mean disease duration (months) (1-18) | 4.7 |
| Location (a) | |
| Labia majora | 9 (52.9) |
| Labia minora | 3 (17.6) |
| Paraclitoral | 1 (5.9) |
| Bartholin gland | 3 (17.6) |
| Intravaginal extension | 4 (23.5) |
| Inguinal | 1 (5.9) |
| Vulva, Unspecified | 1 (5.9) |
| Clinical findings (a) | |
| Firm | 2 (11.8) |
| Painless | 3 (17.6) |
| Tender | 5 (29.4) |
| Mobile | 2 (11.8) |
| Pruritus | 2 (11.8) |
| Swelling/edema | 3 (17.6) |
| Ulceration | 4 (23.5) |
| Erythema | 2 (11.8) |
A Sum exceeds 100% due to non-mutually exclusive categories
Table 2: Clinical presentation of vulvar merkel cell carcinoma [35].
| Histopathological evaluation of vulvar merkel cell carcinomas [35] | |
|---|---|
| Characteristic | n (%) |
| Histologic finding (n=17) | |
| Small cells | 12(70.6) |
| High N/C ratio, scant cytoplasm | 12 (70.6) |
| Nests, islands, trabecular | 11 (64.7) |
| Hyperchromatic | 10 (58.8) |
| High mitotic index | 8 (47.1) |
| Necrosis | 6 (35.3) |
| Irregular nuclei | 4 (23.5) |
| Fibrous | 4 (23.5) |
| Apoptosis | 4 (23.5) |
| Sheets | 3 (17.6) |
| Hemorrhage | 2 (11.8) |
| Ulceration | 2 (11.8) |
| Electron microscopy (n=7)a | |
| Dense core granules | 6 (85.7) |
| Intermediate filaments | 5 (71.4) |
| Immunostaining (n=14)a | |
| Neuroendocrine markers | |
| Chromogranin | 7 (50) |
| NSE | 7 (50) |
| Synaptophysin | 6 (42.9) |
| PGP 9.5 | 2 (14.3) |
| Keratin stains (n=13)a | |
| Pancytokeratin AE1/AE3 | 7 (53.8) |
| CAM5.2 | 4 (30.8) |
| Low molecular weight CK | 3 (23.1) |
| CK7 | 1 (7.7) |
| CK8 | 2 (15.4) |
| CK18 | 3 (23.1) |
| CK19 | 1 (7.7) |
| CK20 | 4 (30.8) |
| Perinuclear dot/granular | 7(53.7) |
Table 3: Histopathological evaluation of vulvar merkel cell carcinomas [35].
Lesions were predominantly located on the labia majora. Histopathological evaluation revealed small, undifferentiated cells with high N/C ratio, scanty cytoplasm. Immunostain results demonstrated higher positivity for pancytokeratine, than other markers. Management of the treatment is based on the surgical excision, vulvectomy or wide excision with 2 cm margins [35]. Recurrence and progression of the tumor are very common complcations after the treatment. There are no standardized protocols for treatment of vulvar MCC due to the rarity [62,63] The guidlines are same like in extravulvar MCC. In general MCC have an aggresive behavior, but those in the vulva are virulent with a 100% rate of inguinal node and also distant metastases [62]. Prognosis of this carcinoma is very poor than prognosis of the MCC arising in other parts of the body [42].
The Merkel cells are still very interesting object of investigation because of its unique functions. They are not only the cells belong to one group with the same functions, but according Lucarz and Brand [15], functionally they can be classified into some subpopulations with different functions: mechanoreceptive, endocrine, chemosensitive. In clinical practice most studies are focus on their neuroendocrine functions and possible malignant transformation into the Merkel cell carcinomas [14]. Primary MCCs of the genitourinary system are very rare, aggressive and may be misinterpreted with other cancers of genitourinary system. There are no standardized protocols for treatment of vulvar MCC due to the rarity [62,63]. The guidlines are same like in extravulvar MCC. In general MCC have an aggresive behavior, but those in the vulva are virulent with a 100% rate of inguinal node and also distant metastases [62]. Prognosis of this carcinoma is very poor than prognosis of the MCC arising in other parts of the body [42]. For pathologists it is very important to differentiate it from other more common tumors of the genitourinary system.