Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 2
Background: Although thyroid nodules are less common in children and adolescents, the malignancy rate for nodules is higher among children and adolescents than adults. A nodule that is discovered in a patient presenting with hyperthyroidism is usually a benign nodule or benign toxic adenoma and, thus, nodules are biopsied only infrequently. Objective: To report a case of papillary thyroid carcinoma presenting with a hyperfunctioning (hot) thyroid nodule. Case report: A 14-year-old female presented with symptoms of thyrotoxicosis and multi-nodular goitre. Laboratory findings were consistent with the diagnosis of thyrotoxicosis. Thyroid ultrasonography showed an enlarged thyroid gland with cystic and solitary nodules, diffuse heterogeneous echo, and microcalcifications. Doppler scans revealed increased vascularity within the left thyroid lobe and a solitary nodule. Thyroid scintigraphy revealed an autonomous nodule. Cytological examination of fine-needle aspirations from the solid nodule and left thyroid lobe revealed papillary thyroid carcinoma. The patient underwent total thyroidectomy. Histopathology of the thyroid gland and lymph nodes were also consistent with papillary thyroid carcinoma with nodal metastases. Conclusion: Contrary to the guidelines published by major endocrine societies, the detection of an autonomously functioning thyroid nodule in children and adolescents does not exclude the possibility of thyroid carcinoma. Suspicious hot nodules should be evaluated cytologically.
<Keywords: Autonomously hyperfunctioning thyroid nodule (AHTN),Thyrotoxicosis,Papillary thyroid carcinoma: thyroid ultrasonography,Children,Adolescent
Although thyroid nodules occur less frequently in children and adolescents than adults, they are more often malignant compared with those observed in older patients [1-4]. Therefore, a major goal of the diagnostic evaluation of thyroid nodules is to differentiate thyroid cancers from benign adenomas. A number of features raise suspicion of malignancy. According to the algorithms reported by the major endocrine societies, a fine needle aspiration biopsy (FNA) is not necessary for the management of thyroid nodules in children in the presence of suppressed thyroid-stimulating hormone (TSH) levels and a hot nodule [1-4]. However, with the advent of high-resolution ultrasonography, 77 cases of biochemically-hyperthyroid patients with autonomous functioning thyroid nodules (AHTN) were discovered to harbor differentiated thyroid carcinoma [5]. Only 11 of these patients were children or adolescents, and there was a higher prevalence of papillary type of cancer and female gender [5,6]. Here, we present an additional case of papillary thyroid carcinoma presenting with thyrotoxicosis in a 14-year-old female.
A 14-year-old female presented to the local state hospital with heat intolerance, weight loss, palpitations, and insomnia for six months. Physical examination revealed an enlarged thyroid gland with a palpable nodule. She was referred to the Pediatric Endocrinology Division at the University Hospital of Eskisehir Osmangazi University because of thyrotoxicosis and nodular goiter symptoms. A detailed medical history revealed that she complained of weight loss (not quantified), nervousness, insomnia, fatigue, tremor, sweaty palms, heat intolerance, palpitations, and hair loss. Her past-medical history included a normal birth, several cases of enteritis, recurrent urinary tract and upper respiratory tract infections, a tonsillectomy at 5 years of age, and no history of previous radiation on her cervical region. Her family history revealed non-neoplastic thyroid disease.
On physical examination, she weighed 46 kg (10th percentile), her height was 155 cm (25th percentile), her body mass index was 19.1 kg/m2, her blood pressure was 115/75 mmHg, and her heart rate was 115 beats per minute. Her skin was warm and moist. Her thyroid gland was enlarged, and there was a palpable non-tender 9×8×8 mm nodule in the lower right lobe and a non-tender 9×7×6 mm nodule in the left lobe. There was no evidence of cervical lymphadenopathy or thyroid bruit. She also had no exophthalmoses or lid lag. She had fine tremor of hands with normal bicep deep tendon reflexes bilaterally, and Tanner stage V breast development.
Thyroid function tests revealed that TSH level was undetectable (<0.001 mcIU/mL, reference range, 0.4-4.5 mcIU/mL), free triiodothyronine was 12.2 pg/mL (International System of Units [SI], 18.6 pmol/L; reference range, 2.3-4.4 pg/mL), and free thyroxin was 6.9 ng/dL (SI, 89 pmol/L; reference range, 0.7-1.8 ng/dL). Thyroid peroxidase antibody testing was negative (8.4 IU/mL, normal <10 IU/mL), as were thyroglobulin antibody (11 mIU/mL, normal <20 mIU/mL), and thyroid-stimulating hormone receptor antibody (<0.1 U/L, normal <1.0 U/L) tests. The thyroglobulin concentration was 112 µg/L (reference range, 2-35 µg/L). The thyroid ultrasonography (US) showed markedly enlarged right and left lobes, measuring 15×18×41 mm and 19×22×48 mm, respectively. There was a 9×8×8 mm nodule that included solid and cystic components in the right lower lobe with a homogenous parenchyma (Figure 1A), and a 9×8×7 mm solid nodule, multiple punctuate non-shadowing echogenic foci (Figure 1B, arrowheads) compatible with microcalcifications or psammoma bodies, and increased vascularity within the solitary nodule and left thyroid lobe (Figure 1C). 99mTc thyroid scintigraphy revealed a hyperactive nodule at the medial-lower segment of the left lobe accompanied by reduced activity in the remaining thyroid gland (Figure 1D). 131I scintigraphy confirmed the hyperactivity of the nodule, and the uptake of 131I at 24 h was 45% (normal reference, 15-35%).
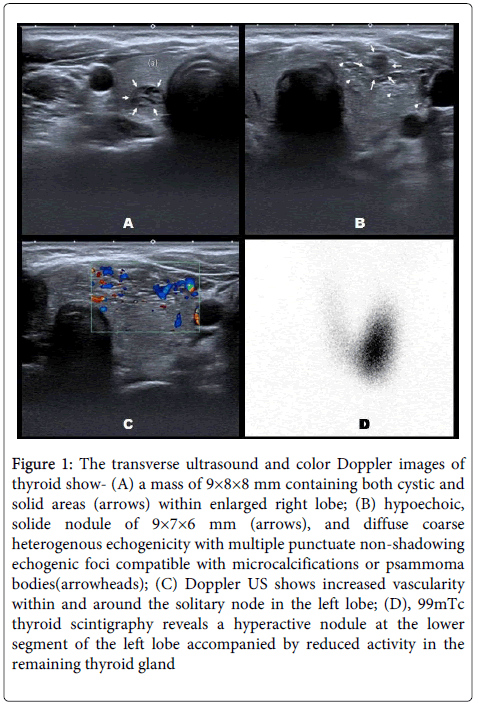
Figure 1: The transverse ultrasound and color Doppler images of thyroid show- (A) a mass of 9×8×8 mm containing both cystic and solid areas (arrows) within enlarged right lobe; (B) hypoechoic, solide nodule of 9×7×6 mm (arrows), and diffuse coarse heterogenous echogenicity with multiple punctuate non-shadowing echogenic foci compatible with microcalcifications or psammoma bodies(arrowheads); (C) Doppler US shows increased vascularity within and around the solitary node in the left lobe; (D), 99mTc thyroid scintigraphy reveals a hyperactive nodule at the lower segment of the left lobe accompanied by reduced activity in the remaining thyroid gland
Based on her clinical features, biochemical thyroid hormone levels, and imaging results, a diagnosis of autonomous hyperfunctioning thyroid nodule (AHTN) was made. Treatment with methimazole 0.2 mg/kg/24 h PO q8h and propranolol 2 mg/kg/24 hr PO q8h were started. She was euthyroid two months after starting the medical treatment. Because of the ultrasonographic signs on the left thyroid lobe, she was referred to the interventional radiology department for US-guided fine needle aspiration (FNA). The cytological investigation was positive for papillary thyroid carcinoma (PTC). After discussions with the parents and the patient, she underwent total thyroidectomy and bilateral central lymph node dissections. Histopathology of the thyroid gland and excised cervical lymph nodes confirmed the diagnosis of PTC and revealed lymph node metastases. The tumor cells showed characteristic nuclear features of PTC, including crowding or overlapping, occasional nuclear grooves, large and pale nuclei, and psammoma bodies (Figure 2A-D). Upon diagnosis of PTC, additional evaluation was performed. Chest X-ray and abdominal US showed no evidence of metastatic disease.
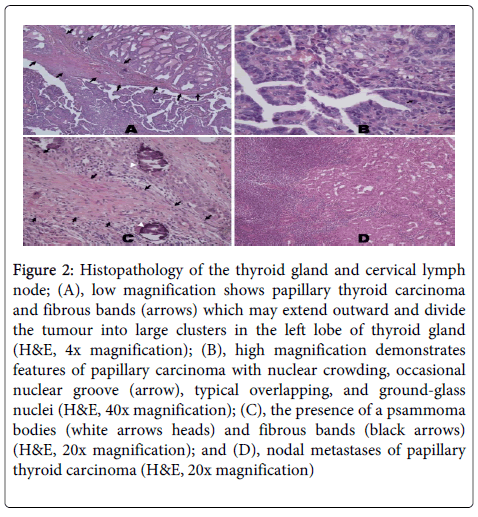
Figure 2: Histopathology of the thyroid gland and cervical lymph node; (A), low magnification shows papillary thyroid carcinoma and fibrous bands (arrows) which may extend outward and divide the tumour into large clusters in the left lobe of thyroid gland (H&E, 4x magnification); (B), high magnification demonstrates features of papillary carcinoma with nuclear crowding, occasional nuclear groove (arrow), typical overlapping, and ground-glass nuclei (H&E, 40x magnification); (C), the presence of a psammoma bodies (white arrows heads) and fibrous bands (black arrows) (H&E, 20x magnification); and (D), nodal metastases of papillary thyroid carcinoma (H&E, 20x magnification)
Six weeks after surgery, she was in frank hypothyroidism and underwent 131I radioactive ablation. A 125-mCi131I dose was administered; an 131I whole-body scan showed some uptake into the cervical area, and there was no evidence of metastatic disease.
Subsequently, levothyroxine was started at a dose of 150 g per day to restore normal thyroid function tests. One year after the total thyroidectomy, a, 131I scan showed no significant uptake in the thyroid bed or elsewhere in her body, and her Tg levels were undetectable, which is consistent with remission. She has been followed up at 8 month intervals, and the dose of levothyroxine was reduced to 125 g/day.
Although thyroid nodules generally occur less frequently in children and adolescents than in adults, the risk of malignancy is higher in the pediatric age group compared with adults [7,8]. Therefore, thyroid malignancy should be suspected when a thyroid nodule is found in children and adolescents because it has been reported that up to 20-25% of nodules in pediatric patients are malignant, compared with 5% in adults [1-4,9]. An increasing number of thyroid nodules in children have been discovered incidentally because of the widespread use of neck US. In addition, the vast majority of thyroid nodules occur in euthyroid conditions. The main objective of the diagnostic approach to thyroid nodules is to make a differential diagnosis as to whether a thyroid nodule is benign or malignant. This decision is made based on the patient’s past-medical history, family history, clinical presentation, and thyroid US characteristics. Clinical and ultrasonographic features of thyroid nodules that require FNA are summarized in (Table 1) [4,10-12].
| Nodule sonographic or clinical features | Recommended nodule threshold size for FNA |
|---|---|
| High-risk historya | |
| •Nodule WITH suspicious sonographic featuresb | >5mm |
| •Nodule WITHOUT suspicious sonographic featuresb | >5mm |
| Abnormal cervical lymph nodes | Allc |
| Microcalcifications present in nodule | ≥1cm |
| Solid nodule | |
| •AND hypoechoic | >1cm |
| •AND iso- or hyperechoic | ≥1–1.5cm |
| Mixed cystic–solid nodule | |
| •WITH any suspicious ultrasound featuresb | ≥1.5–2.0cm |
| •WITHOUT suspicious ultrasound features | ≥2.0cm |
| Spongiform nodule | ≥2.0cmd |
| Purely cystic nodule | FNA not indicated |
Table 1: Sonographic and clinical features of thyroid nodules and recommendations for fine-needle aspiration (FNA)s (Adapted from the reference [4]).
A) High-risk history: History of thyroid cancer in one or more first degree relatives; history of external beam radiation as a child; exposure to ionizing radiation in childhood or adolescence; prior hemithyroidectomy with discovery of thyroid cancer, 18FDG avidity on PET scanning; MEN2/FMTC-associated RET protooncogene mutation, calcitonin >100 pg/mL. MEN, multiple endocrine neoplasia; FMTC, familial medullary thyroid cancer.
B) Suspicious features: microcalcifications; hypoechoic; increased nodular vascularity; infiltrative margins; taller than wide on transverse view.
C) FNA cytology may be obtained from the abnormal lymph node.
D) Sonographic monitoring without biopsy may be an acceptable alternative
Thyrotoxicosis is uncommon in children; the most common etiology is Graves’ disease, which presents with diffuse goiter [13]. AHTN is an extremely rare etiology of thyrotoxicosis in children that is always diagnosed as a toxic adenoma. The guidelines and recommendations published by major endocrine societies recommend that malignant thyroid nodules typically do not take up radionuclides and appear cold, and that hyperfunctioning nodules on scintigraphy are almost always benign adenoma [1-4]. The American Thyroid Association (ATA) guidelines for patients with thyroid nodules recommend that no cytological evaluation is necessary for hyperfunctioning thyroid nodules [4]. Therefore, in hot nodules, thyroid US and cytological evaluation are not recommended routinely. Differentiated thyroid carcinoma may be a co-incidental finding in a case of thyrotoxicosis presenting with thyroid nodule [14]. However, papillary thyroid carcinoma was not a coincidental finding in our patient. The AHTN in the left thyroid lobe was confirmed using both biochemical parameters of thyrotoxicosis, and scintigraphic evidence of increased uptake of 131I and 99Tc. Thyroid US, particularly in the left lobe, revealed several distinctive signs of thyroid malignancy, such as microcalcifications and heterogeneous echo texture. The ultrasonographic findings of microcalcifications, which were compatible with the psammoma body on the histological analysis (Figure 2), are one of the most specific signs of thyroid malignancy, particularly in PTC [11]. Therefore, we performed ultrasound-guided FNA, and cytological investigation revealed the diagnosis of PTC. She underwent total thyroidectomy, and histopathology of thyroidectomy specimens confirmed the cytological diagnosis with nodal metastases.
There have been several other reports of thyroid malignancies in an AHTN, and the estimated cancer risk in hot nodules ranges from 3.1-11% [5,15-22]. To the best of our knowledge, 77 cases of thyroid malignancy related to AHTN or thyrotoxicosis have been reported [5]. The mean nodule size in these patients was 4.13 ± 1.68 cm. The patient in our case report had no high-risk history, and the maximum dimension of the nodule was 0.9 cm. If we had used the =1.0-1.5 cm size criteria for suspicious nodules that is recommended by ATA guidelines [4], our patient would not have been diagnosed with PTC. Therefore, before deciding whether AHTN is benign, we suggest that thyroid US should be performed by an experienced radiologist in all patients with hot nodules. If the radiologist reports any suspicious findings that suggest thyroid malignancy, as seen in the present case, the patient should be referred for FNA.
In conclusion, in contrast to the guidelines published by major endocrine societies, AHTN does not exclude thyroid malignancy. To exclude the possibility of thyroid cancer, thyroid US should be performed in all patients with AHTN. If the radiologist reports any suspicious findings that suggest thyroid malignancy, all patients should be referred for FNA and cytological evaluation. Our case gives further support for the recommendation that surgery should be performed more frequently to treat thyroid nodules (both cold and hot) in children and adolescents because of the lower prevalence of thyroid nodules and the higher malignancy rate in this age group.