Journal of Glycobiology
Open Access
ISSN: 2168-958X
![]() +44 1478 350008
+44 1478 350008
ISSN: 2168-958X
![]() +44 1478 350008
+44 1478 350008
Research Article - (2014) Volume 3, Issue 2
Keywords: Mucopolysaccharidosis; Total mucopolysaccharides; Alcian blue dye; Normal excretion in the pediatric group
Introduction
Mucopolysaccharide (MPS) storage diseases are clinically progressive, hereditary disorders characterized by the accumulation of mucopolysaccharides (MPS) in various connective tissues and their excessive excretion in urine [1].
The classic method for mucopolysaccharide determination in urine relies on their carbazole reaction [2]. However, this method is characterized by its inability to detect dermatan sulfate and utilization of caustic concentrated sulfuric acid.
The formation of soluble complexes between alcian blue dye and MPS provides the basis for an alternative quantitative spectrophotometric estimation of all classes of mucopolysaccharides [3-5]. In this method urinary MPS react with alcian blue dye reagent and the MPS complex is separated, washed and dissolved in a detergent [6]. However, complete dissolution of the complex is not easily achieved due to strong binding to the inner wall of the plastic centrifuge tube. Furthermore, on utilizing glass tubes for centrifugation, linearity could not be established due to nonspecific binding of excess dye to the tube.
A variant of the dye-MPS complex method was suggested by Gold [5]. This author used the very minute optical density (O.D.) changes observed at 480 nm resulting from complex formation to calculate MPS concentration. Although, it is simple and convenient, this method introduced a large margin of uncertainty Figure 1.
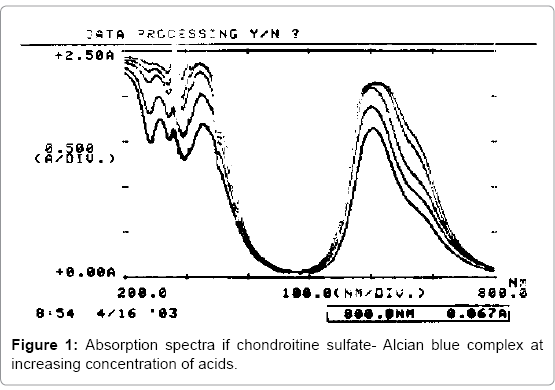
Figure 1: Absorption spectra if chondroitine sulfate- Alcian blue complex at increasing concentration of acids.
In this study, we present a modification of the dye binding method that requires no use of detergent and produces linear standard curves due to simple washing of non-specifically bound dye. Also the normal range in various age groups is reported.
Alcian blue dye was dissolved in a solution of 15% concentrated phosphoric acid and 2% concentrated sulfuric acid to produce a final dye concentration of 0.2 mg/ml. The dye dissolves completely and no filtration is recommended. The dye solution can be stored at room temperature. This contrasts with the limited stability of the dye solution prepared in sodium acetate which undergoes progressive aggregation of dye with a corresponding decrease in background absorbance, thereby requiring fresh preparation prior to use.
A standard curve is prepared using purified chondroitin 6-sulfate. Chondroitin sulfate functions as a convenient and inexpensive standard. Samples containing 4, 8, 12 and 16 μg of CS are adjusted to the volume of 50, 100, 150 and 200μl respectively. A blank containing 0.10 ml of water is also prepared. To each tube, 1.0 ml of the dye solution is added and the contents are thoroughly mixed and vortexed. Then the tubes were subject to centrifugation at 3500 RPM for 10 minutes; then after a careful decantation, they were subject to washing by adding 2 ml of a sodium acetate buffer solution (0.05M; pH=5.8) to the precipitated CS-dye complex for three times, the last time with no decantation. The tubes are thoroughly mixed and vortexed again, and the absorbance at 608 nm of each tube is measured against the blank in quartz cuvettes with a capacity of 1ml. The blue color imparted by the analyses can be removed by rinsing with concentrated sulfuric acid.
Samples of purified dermatan sulfate, heparan sulfate, hyaluronic acid were studied also, using the same method. The reactivities of these MPS with respect to chondroitin sulfate were as follow: 80% for dermatan sulfate, 108% for heparane sulfate, and 91% for hyaluronic acid.
Random samples of urine were collected from normal individuals. Individuals were chosen of different age groups with the majority of them being of less than 5 years of age. The samples preferably first morning void, were freshly collected without addition of any preservative. All urine samples were refrigerated if not analyzed immediately.
The absorbance spectra from 200-800 nm of alcian blue dye and alcian blue-chondroitin sulfate complexes in different acid dye solutions (we used increasing phosphoric and sulfuric acid concentrations from solution containing 0.30% of H2PO4 and 0.04% H2SO4 up to solution containing 15.0% of H3PO4 and 2.0% H2SO4) with keeping the same concentration of the dye in all the acid-dye solutions) are shown in Figure 1. The spectra of dye alone and the acid dye-chondroitin sulfate complexes exhibit an absorbance maximum at 608 nm with decreasing of the absorbance as the concentration of the acids increases. This figure shows clearly the rationale for using the wave length 608 nm instead of 480, as used by prior investigators, because there is minimal difference between blanks (dye alone solution) and dye-chondroitin sulfate solution as compared to the net difference using the 608 nm wave length. For example [5], the change in optical density at 608 nm in contrast to 480 for the same amount of MPS was approximately 6.5 times larger when using a basic dye solution and 2.5 times when using an acid dye solution (13.75 mAbs/μg CS vs. 5.5 and 2.5 mAbs/ μg CS respectively).
The linearity was established using both pure chondroitine sulfate solution and urine, and it is shown in Figure 2. While the linearity of the purified compound is well established up to 160 μg/ml of dyemixture solution, the linearity for urine MPS is established up to 100 μl (equivalent to 100 μg/ml of MPS). Thus, we recommend using 50 μl of urine for the detection of MPS, for individuals more than 1 year of age and 100 μl for less than 1 year (the urine of neonates and infants is usually diluted, and they normally excrete less MPS per volume of urine compared to adults).
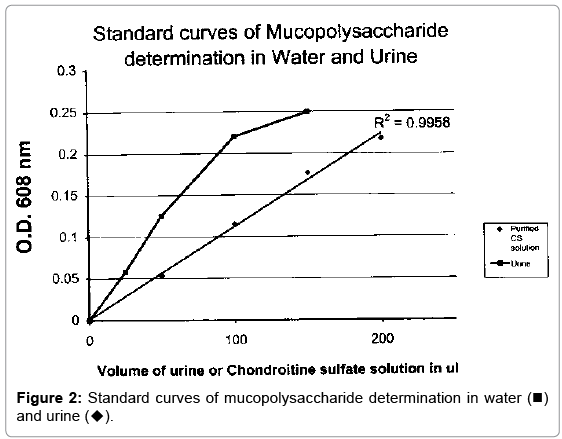
Figure 2: Standard curves of mucopolysaccharide determination in water (■) and urine (▴).
The normal urinary MPS excretion (measured in mg of MPS/mmol of creatinine) in relation to age was established using the standard curve and the results were: 18.5 ± 4 mg MPS/mmol creatinine for ages between 0 and 6 months; 15.3 ± 3 for ages between 6 and 12 months; 10.8 ± 2.5 for ages between 1 and 5 years and 8.2 ± 3 for older ages.
The fact that there is a breakpoint in the linearity of MPS in urine at lower levels compared to those established using pure compounds suggests the presence of other substances that might inhibit the reaction between MPS and the dye. The recognition of these substances is the subject of future study.
In conclusion, the proposed dye binding method is superior to the carbazole method since it includes dermatan sulfate a major MPS in urine; this has been proven by us as well as by others [5]. Moreover the change in optical density at 608 nm in contrast to 480 for the same amount of MPS is approximately 6.5 times larger. Hence the certainty of measurement is much higher. Furthermore, the sensitivity of this method is comparable to the direct method using dimethyl methylene blue proposed by Whitley [7] and de Jong [8]. Our normal values are comparable to those reported by Piraud [6] and others [9].